Your EHR has a bigger job than you think
Let’s start with an uncomfortable truth.
Most behavioral health organizations chose their EHR the same way they chose their office chairs, based on what was available at the time, what fit the budget, and what a few other people in the space were already using. And for a long time, that worked out reasonably well. Document the session. Bill the payer. Move on.
Where the reality is:
Payers are moving from volume to value. CMS launched the Innovation in Behavioral Health (IBH) Model in 2024, pushing rural health clinics and Federally Qualified Health Centers (FQHC) to bill new Behavioral Health Integration CPT codes tied to outcome metrics like depression-remission rates. The CY 2026 Physician Fee Schedule finalized by CMS in October 2025 and effective January 1, 2026 continues that trajectory, exempting time-based behavioral health services from the efficiency adjustments being applied to traditional fee-for-service codes, while expanding reimbursement for care management, digital mental health treatments, and chronic care coordination. Telehealth parity for behavioral health is now effectively permanent. The message is unmistakable: reimbursement follows outcomes, and outcomes require coordination.
Here’s the problem nobody in EHR marketing wants you to say out loud: most behavioral health EHRs were not built for this. They were built to be really good digital filing cabinets. And a digital filing cabinet, no matter how elegantly designed, cannot orchestrate care across a crisis team, a primary care partner, a peer support specialist, and a payer’s quality dashboard all at once.
That’s the difference we’re going to unpack in this guide. This is not a features versus features guide. But philosophy versus philosophy. And ultimately, which software architecture is actually capable of supporting you in a value-based care world.
The behavioral health EHR landscape: 3 types of EHRs
Walk into any HIMSS conference or behavioral health leadership summit today, and you’ll find dozens of vendors claiming to be purpose-built for behavioral health. Some of them are telling the truth (most are not).
The market is highly fragmented, with a large number of small and medium-sized vendors competing alongside a handful of established players. Cloud-based solutions now dominate, holding over 83% of the market. Cloud architecture is what enables real-time data sync, embedded telehealth, and mobile charting for your community-based teams. If any vendor is still leading with an on-premise pitch as their primary offering in 2026, that alone should give you pause.
But cloud-based isn’t automatically good. The more important question is what the platform is designed to do with the data it collects. And this is where behavioral health EHR evaluation gets genuinely complex.
There are really three types of software competing for your signature right now:
Type 1: General medical EHRs with a behavioral health module
These platforms were built for physical health workflows and bolted on behavioral health functionality as an afterthought. They’ll have the checkboxes. They’ll struggle with the nuances of 42 CFR Part 2 data segmentation, SUD-specific treatment workflows, crisis documentation, peer support notes and more. The customization costs add up fast.
Type 2: Standalone behavioral health EHRs
These were built ground-up for behavioral health. They handle clinical documentation well, often have good billing workflow support, and may include some telehealth. The limitation is interoperability — getting these platforms to talk meaningfully to primary care partners, HIEs, and payer quality reporting systems is often where things get painful.
Type 3: Care coordination orchestration platforms with behavioral health EHR at the core
This is the category that matters most right now. These platforms don’t just document what happened in the session, they actively manage what needs to happen next. Referral tracking, multi-disciplinary team communication, population health dashboards, payer quality measure reporting, crisis care coordination, and care gap identification all live in the same ecosystem as the clinical note. The EHR becomes a command center, not a chart room.

If you’re a single-provider outpatient clinic, Type 2 might be entirely sufficient for where you are today. But if you’re operating as a CCBHC, a multi-site community mental health center, or an enterprise organization serving thousands of patients under value-based contracts, Type 3 is not optional — it’s existential.
The seven features that actually define a behavioral health EHR in 2026
Vendor feature checklists will give you a hundred bullet points. Here are the seven that genuinely separate platforms when the rubber meets the road.
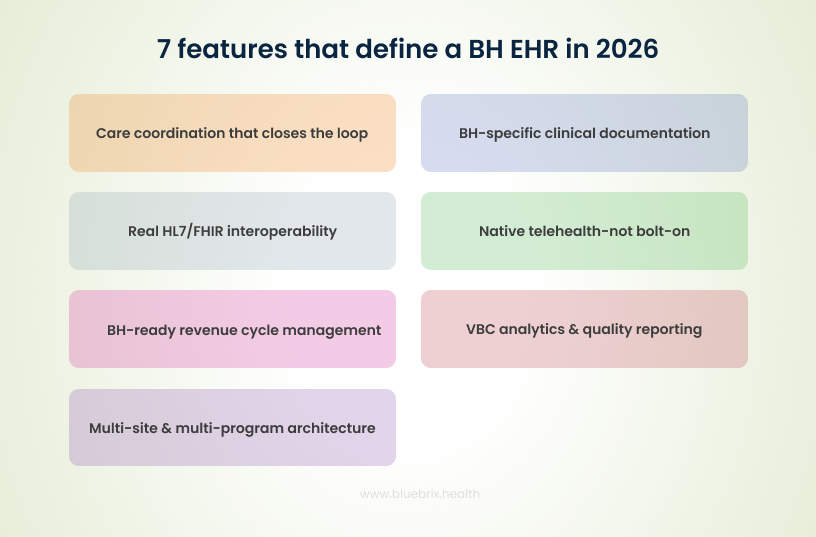
1. Care coordination that closes the loop automatically
SAMHSA’s CCBHC certification criteria make this unambiguous: care coordination is the linchpin of the CCBHC model. Not a nice-to-have. The linchpin. That means your EHR needs to do more than let you document a referral. It needs to confirm the referral was kept, flag the ones that weren’t, trigger follow-up workflows, and support real-time patient tracking across your entire care team.
The CCBHC 2024 impact data illustrates what’s possible when coordination is built in: 76% of CCBHCs reported that referrals to primary care increased after becoming a CCBHC, including 30% that saw increases of 20% or more. That’s not happening with manual referral processes. That’s technology closing the loop.
This is also where AI starts pulling real weight. Predictive analytics embedded in the care coordination layer can surface patients at risk of disengaging from care before a missed appointment becomes a dropout. AI-driven care gap identification means your coordinators aren’t manually scanning caseloads for patients overdue for follow-up; the platform flags them automatically, prioritized by risk. The best platforms in 2026 are moving from reactive care coordination to predictive care orchestration and AI is what makes that shift possible.
Look for: bi-directional referral tracking, multi-disciplinary care team dashboards, automated follow-up triggers, real-time patient status visibility across programs, and AI-powered risk stratification that surfaces care gaps before they widen.
2. Behavioral health-specific clinical documentation
This one sounds obvious, but the gap between general EHR documentation and behavioral-health-specific documentation is wider than most buyers realize. You need pre-built templates for therapy notes, psychiatric evaluations, SUD treatment plans, and crisis intervention documentation, not generic SOAP notes you’ve jury-rigged to fit a behavioral context.
AI is reshaping this area faster than any other. Ambient documentation is in production at behavioral health organizations today. But the key word is behavioral health-specific: ambient AI trained on general medical encounters handles psychiatric evaluations and therapy sessions poorly. Ask your vendor specifically whether their AI documentation tools are trained on behavioral health clinical content, or whether you’re adapting a general medical model to fit your workflows.
More importantly, you need 42 CFR Part 2 compliance baked in, not patched on. Substance use disorder records have stricter privacy protections than standard HIPAA-covered records, and the data segmentation your EHR provides needs to reflect that at a technical architecture level, not just through a policy document your vendor hands you at onboarding.
3. Interoperability that’s real, not theoretical
HL7/FHIR isn’t a marketing term. It’s the technical standard that determines whether your behavioral health record actually integrates with a patient’s primary care provider, the state HIE, the prescription drug monitoring program (PDMP), and the payer’s quality reporting system. After the 2024 revisions to 42 CFR Part 2 which aligned SUD data sharing more closely with HIPAA, the regulatory groundwork for broader interoperability is finally in place. Your EHR needs to be ready to capitalize on that.
Ask specifically: does your vendor have live HL7/FHIR integrations in production today, or are they promising a roadmap? There is a meaningful difference.
4. Telehealth that’s native, not bolt-on
Telehealth integration is one of the fastest-growing components in the behavioral health EHR market. The 2026 CMS rules have made behavioral health telehealth flexibilities effectively permanent, and major payers have broadly aligned in-person and telehealth reimbursement rates. The hybrid care model isn’t going anywhere. But there’s a world of difference between a Zoom link embedded in a scheduling email and a true telehealth integration where the video session flows directly into the clinical note, with e-prescribing, patient engagement, and billing charge capture happening within the same encounter.
HIPAA-compliant in-session documentation and ePrescribing capability, including DEA EPCS compliance for controlled substances are the benchmarks. Anything less is a workaround that creates clinical and compliance risk.
5. Revenue cycle management built for behavioral health complexity
Behavioral health billing is not the same as medical billing. You’re managing multiple payer types including Medicaid, commercial insurance, grants, self-pay, sliding scale etc. often for the same patient within the same month. CCBHC Prospective Payment System (PPS) rates add another layer of complexity that general RCM tools handle poorly.
AI is changing the calculus here meaningfully. Intelligent claims scrubbing, where AI reviews a claim before submission and flags likely denials based on payer-specific patterns, reduces your denial rate before it becomes an A/R problem. AI-driven coding suggestions reduce undercoding and overcoding errors that behavioral health practices are particularly prone to, given the complexity of time-based and complexity-based billing. And when denials do occur, AI-assisted appeals workflows can identify the right clinical documentation to attach and prioritize appeals by revenue recovery potential.
What you need: automated eligibility verification, ERA/X12 claims processing, multi-payer support, one-click claims submission, real-time denial tracking, AI-assisted coding and claims intelligence, and reporting that maps directly to your value-based care quality metrics. When your billing system knows whether a quality measure was met before the claim goes out the door, you’ve moved from reactive to proactive revenue management.
6. Value-based care analytics and quality measure reporting
This is where many platforms talk a big game and underdeliver. Value-based care contracts require you to demonstrate outcomes such as depression remission rates, follow-up after hospitalization, initiation and engagement in substance use treatment. These are not metrics you can cobble together in a spreadsheet at the end of the quarter. They need to be embedded in your clinical workflow from day one, so that the data you’re documenting in the session is the same data powering your quality dashboard.
CCBHC certification alone requires reporting on 18 mandatory quality measures, with optional reporting on seven additional ones. If your EHR doesn’t have pre-built, automated reporting for these measures, you’re building that infrastructure yourself and that cost rarely shows up in any vendor proposal.
AI makes this layer significantly more powerful. Rather than waiting until the end of a measurement period to discover a quality measure shortfall, AI-driven analytics can monitor measure performance continuously, flagging in real time when a patient cohort is trending below target and recommending specific interventions. The difference between a static reporting dashboard and an AI-powered quality intelligence layer is the difference between knowing you missed a measure and knowing early enough to do something about it. For organizations operating under value-based contracts where bonus payments hinge on measure performance, that distinction has direct revenue implications.
7. Scalable multi-site and multi-program architecture
This is the feature that separates a good outpatient platform from a true enterprise solution. For organizations operating across multiple locations, multiple programs, and multiple provider types, the EHR architecture itself needs to support centralized management without flattening the nuance of each program’s workflow.
Think about what that actually means operationally: a clinician at your SUD outpatient program shouldn’t have to navigate the same system view as your crisis team. But your COO and your compliance officer should be able to see across all programs in a single reporting dashboard. A scalable architecture covers role-based access, program-level configuration, and enterprise-level analytics that still respect clinical workflow specificity.
What scalability actually means for behavioral health EHR
Every behavioral health EHR vendor will tell you their platform scales. What they mean varies enormously.
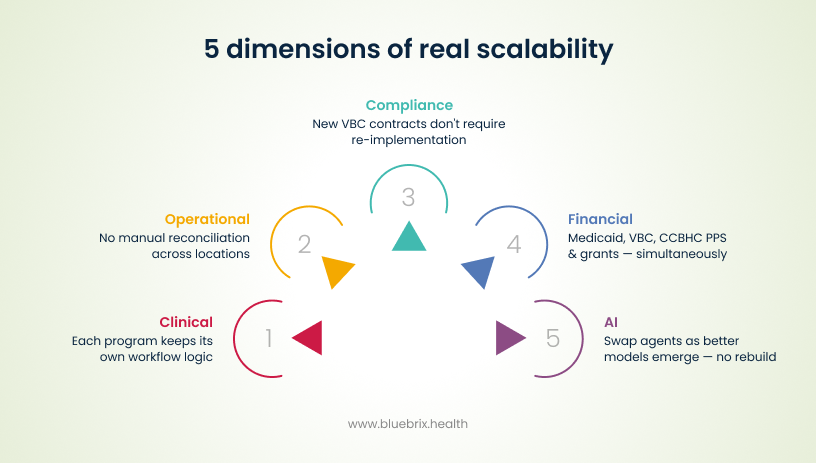
For some, scalability means you can add more user seats and the system won’t crash. That’s not scalability — that’s basic cloud infrastructure. True scalability in a behavioral health context means:
- Clinical scalability — The platform supports diverse program types under one organizational umbrella without forcing clinical workflow compromises. Your assertive community treatment (ACT) team and your outpatient therapy group have genuinely different documentation needs. A scalable platform accommodates both without requiring each program to abandon its workflow logic.
- Operational scalability — Multi-site coordination doesn’t become a manual aggregation exercise. Scheduling, billing, and reporting work across locations without siloed data that your team reconciles in Excel at month end.
- Compliance scalability — As your organization takes on new value-based contracts, new grant requirements, or new CCBHC programs, the reporting engine adapts without a six-month implementation project every time. Pre-built compliance reporting for Medicaid, CCBHC, and value-based care programs is table stakes for any enterprise-serious platform.
- Financial scalability — The RCM layer grows with your payer complexity. When you’re operating under five different reimbursement models simultaneously, your billing system needs to manage that without a team of billing specialists manually adjusting each claim type.
- AI scalability — This is the dimension most buyers aren’t thinking about yet in 2026, but should be. As new AI models emerge and your VBC contracts evolve, can you swap or add AI tools without re-implementing the underlying platform? A closed AI architecture where your EHR vendor controls which models you can access is a strategic risk as the AI ecosystem continues to evolve rapidly.
Here’s the vendor trap to watch for: a platform that handles all of these functions competently at small scale often hits a wall at enterprise volume.
The value-based care mandate: why your EHR is now a strategic asset
Let’s put some numbers around this.
In a fee-for-service world, your EHR’s financial role was relatively straightforward: document the service, code it correctly, submit the claim, collect the payment. The EHR was an administrative tool.
In a value-based care world, the same system now determines whether you hit the quality measures that unlock bonus payments, avoid the performance penalties that claw back revenue, demonstrate the population health outcomes that renew your contract, and generate the cost-of-care data that earns you a seat at the payer’s network table.
That’s a strategic asset (or a liability) depending on how well it’s built.
The CY 2026 Physician Fee Schedule which was finalized in October 2025, sends a clear signal: behavioral health integration, care management, and time-based coordination services are specifically protected from the efficiency adjustments being applied to traditional office-based fee-for-service codes. CMS is also expanding payment for Digital Mental Health Treatment (DMHT) services to include new conditions like ADHD, and has permanently streamlined the telehealth services list for behavioral health. Every one of these policy moves rewards coordinated, outcome-driven behavioral health care. Organizations whose EHRs can generate the data to prove they’re delivering it will win and others will be flying blind in negotiations.
This is the context in which care coordination orchestration goes from buzzword to business requirement. An EHR that simply records what happened is insufficient. You need a platform that actively manages care trajectories — identifying patients who’ve missed follow-up appointments, flagging gaps in care before they become crises, tracking quality measure completion in real time, and connecting your clinical teams across program silos.
Enterprise behavioral health: the specific challenges that break generic platforms
If your organization is operating at enterprise scale with multiple sites, multiple programs, hundreds of providers, thousands of patients etc. there are a few specific scenarios where generic platforms (even good generic platforms) consistently fall apart.
Multi-payer complexity under value-based contracts. At enterprise scale, you may be managing Medicaid managed care contracts, commercial payer VBC agreements, CCBHC PPS rates, federal grants, and self-pay all simultaneously. Each has different quality measure definitions, different documentation requirements, and different reporting timelines. A platform that hasn’t been specifically engineered for this complexity will force your billing and compliance teams to absorb that complexity manually which is expensive, error-prone, and doesn’t scale.
Crisis service integration. SAMHSA’s updated CCBHC criteria require tight alignment with the 988 Suicide and Crisis Lifeline. CCBHCs need to ensure every patient has a crisis plan, and that the CCBHC has a care coordination partnership with the local 988 center. Your EHR needs to support crisis documentation, real-time mobile crisis team coordination, and referral tracking that captures whether the follow-up care after a crisis visit actually happened. Only 11% of CCBHCs are currently using formal coordination relationships for primary care screening and monitoring, a gap that thoughtfully designed technology can close.
Data segmentation for SUD records. 42 CFR Part 2 compliance at enterprise scale requires that your EHR can segment patient records at a granular level, ensuring that SUD data is only shared with the appropriate consented parties even when that patient’s record exists across multiple programs within your organization. This is a genuine technical architecture challenge, not a workflow configuration. Ask your vendor specifically how their data model handles this, not just whether they say they’re compliant.
Workforce documentation across disciplines. An enterprise behavioral health organization might have psychiatrists, licensed clinical social workers, peer support specialists, case managers, and community health workers all contributing to the same patient’s care. Each discipline has different documentation requirements, different billing implications, and different supervision workflows. What you need is a platform that can manage all of these within a coherent clinical record without creating documentation silos.
blueBriX purpose-built behavioral health EHR for care coordination and value-based care
blueBriX was built from the ground up to address exactly these challenges — not as an afterthought or an acquired module, but as core architectural decisions.
What makes blueBriX distinctly different from most platforms competing in this space is its approach to AI. Rather than bolting on a single AI tool and calling it done, blueBriX operates as an open AI orchestration platform, meaning it can integrate and coordinate AI agents from multiple sources, governed by a unified Trust Engine that validates every AI-driven action against your specific VBC contract terms, payer rules, and compliance requirements before it executes.
In practice, this means three things:
- You’re not locked into one AI vendor’s roadmap. As better models emerge for specific workflows — HCC coding, care gap closure, prior authorization, denial prevention — you can swap or add agents without rebuilding your platform.
- Every AI suggestion, whether from a blueBriX native agent, a pre-validated partner agent, or your own existing AI tool (Bring Your Own Agent) passes through the same governance layer before touching your contracts, data, or patients.
- Because blueBriX owns the full stack — EHR, RCM, care coordination, and patient engagement — AI agents don’t just suggest, they execute. A care gap identified by an AI agent can trigger an outreach workflow, update a care plan, and capture the quality measure credit, all within the same platform.
For CCBHCs and community mental health centers, the platform integrates care coordination, compliance reporting, ePrescribing with DEA EPCS support, telehealth, and RCM into a single system. The care coordination layer tracks patient progress, manages referrals, and supports multidisciplinary collaboration across programs — so your care coordinators spend their time on patient relationships, not chasing paperwork.
For enterprise organizations managing multiple sites, blueBriX provides HL7/FHIR interoperability with HIEs, PDMPs, payers, and external EHRs; centralized multi-site management with role-based access and data segmentation; pre-built reporting for CCBHC quality measures, Medicaid, and value-based care models; and ERA/X12 claims processing with real-time eligibility verification across multiple payers.
For virtual and hybrid care, the telehealth platform is HIPAA-compliant and natively integrated — meaning in-session documentation, ePrescribing, and billing charge capture happen within the same clinical encounter, not as disconnected workarounds.
The underlying principle is that care coordination can’t be an add-on to a documentation platform, and AI can’t be an add-on to either. All three have to be the platform’s central organizing logic — with documentation, billing, compliance, and analytics built around them.
A practical evaluation framework: the four questions that matter
Before you issue your next RFP or sit through your next demo, here are the five questions that will cut to the center of what you actually need to know:
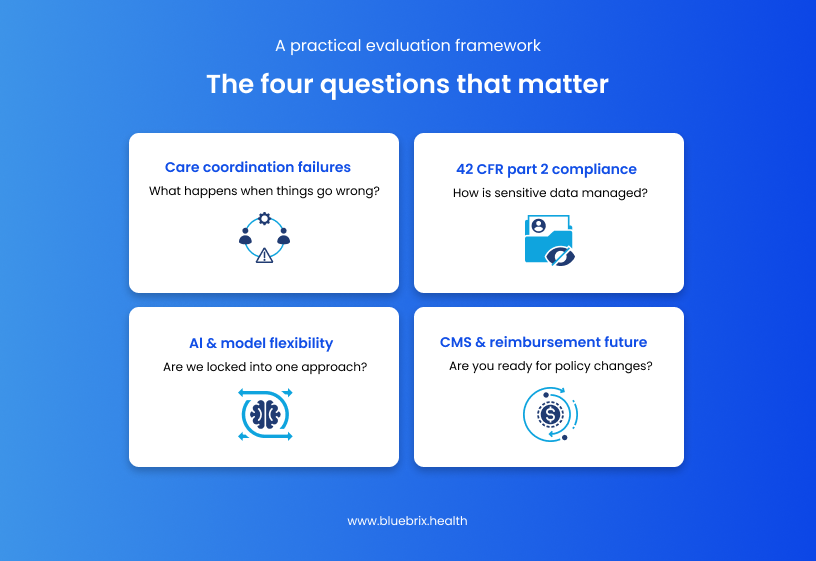
How does your platform handle care coordination failures?
Ask: when a referral isn’t kept, when a follow-up appointment is missed, when a quality measure falls behind target – what does the system do automatically? The answer tells you whether you’re looking at an orchestration platform or a documentation tool.
What does 42 CFR Part 2 compliance look like in your data architecture?
Get technical. Ask about record-level data segmentation, consent management workflows, and how the system handles a scenario where a patient has both SUD and non-SUD records that may be accessed by different care team members. Policy documents are not architecture.
What is your AI strategy and are we locked into your chosen models?
Find out whether AI capabilities are native, sourced from a single third-party vendor, or orchestrated across multiple agents with open connectivity. Ask: what AI use cases are live in production today, which ones are on the roadmap, and if a better AI model emerges for a specific workflow can we adopt it without rebuilding the platform? A vendor locked into one AI provider’s roadmap is betting your organization’s future on that provider’s product decisions.
How does your roadmap align with where CMS reimbursement is heading over the next three years?
If your vendor doesn’t have a clear, specific answer about how their platform is evolving to support the IBH Model, collaborative care billing, and population health requirements, they are not building for where behavioral health is going, they are maintaining where it has been.
Ready to see what care coordination orchestration looks like in practice?
If you’re evaluating behavioral health EHR platforms for a multi-site or CCBHC context or if you’re facing a renewal decision and wondering whether your current platform can genuinely grow with your value-based care ambitions, we’d like to show you how blueBriX approaches these challenges differently.
Schedule a personalized demo and bring your toughest workflow scenario. We’ll show you exactly how the platform handles it live (not in a slide deck).
Request a demo