care coordination

The Centers for Medicare & Medicaid Services (CMS) is driving a major transformation in healthcare payment models. Their goal is to have all Medicare, and most Medicaid beneficiaries participate in Value-Based Care (VBC) programs by 2030. Aligned with this, the healthcare landscape’s focus is shifting from simply treating illnesses to proactively managing the health of entire populations. This paradigm shift for healthcare organizations comes with many challenges.
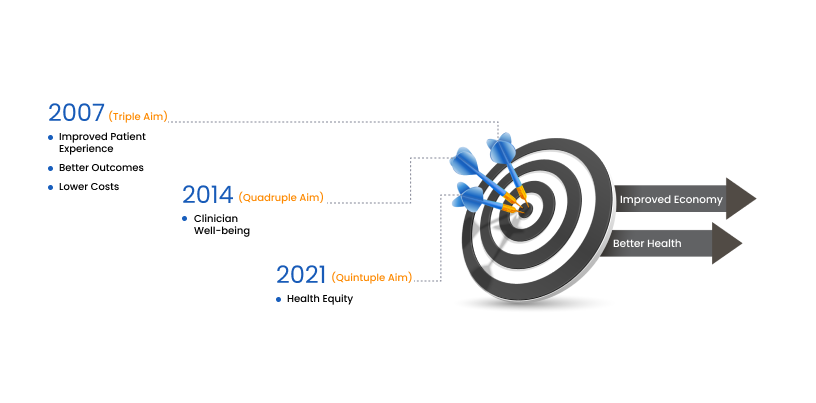
Many organizations like Institute for Healthcare Improvement, Health Catalyst and RTI Healthcare are providing guidelines and frameworks to ease this shift. The Institute for Healthcare Improvement’s (IHI) Triple Aim Framework, which was developed in 2007, aligned well with the recommendations of CMS for VBC implementation. IHI’s framework is considered the “North Star” for healthcare organizations shifting from traditional models to value-based care. In 2021, IHI introduced the Quintuple Aim Framework which included health equity as an important element of VBC. Population health continues to be a critical part of VBC through this framework evolution.
By implementing effective PHM strategies, healthcare providers can identify at-risk individuals, intervene early to prevent complications and deliver more coordinated care. In this blog, we’ll explore the key performance indicators of PHM and four key strategies that can help healthcare organizations achieve the population health management KPIs. We’ll also explore how blueBriX’s digital health solutions can support each strategy and empower healthcare providers to deliver exceptional population health management programs.

To meet and exceed the population health KPIs, the healthcare organizations must devise the right strategies. We suggest following strategies that focus on health outcomes – prevention, early intervention, and coordinated care to improve the overall health of a population.
Strategies to improve population health outcomes
1. Stratification and risk identification
PHM can be effective only when the patient population data is analyzed. This involves stratifying patients into different risk groups based on factors like demographics, social determinants of health, and medical history. blueBriX’s data analytics platform, blueIntelligence can be a powerful tool for this purpose. It can collect and analyze patient data from various sources, including electronic health records (EHRs), claims data, and patient-reported information from multiple connected clinics within the organization’s system and outside. By identifying individuals at high risk for chronic diseases or complications, healthcare providers can prioritize interventions and allocate resources more effectively.
Using data analytics to reduce hospital readmissions
A large healthcare system implemented a PHM program that utilized data analytics to identify patients at high risk for hospital readmission. The program leveraged a platform like blueIntelligence to analyze patient data and predict readmission risk. Based on these predictions, care teams proactively reached out to high-risk patients, provided them with personalized education and self-management tools, and ensured timely follow-up appointments. The program resulted in a significant reduction in hospital readmission rates and improved patient outcomes.
2. Care coordination and care management
Once at-risk individuals are identified, the next step is to ensure they receive coordinated and comprehensive care. This might involve collaboration between different healthcare providers, specialists, and social service agencies. blueBriX’s secure communication platform can facilitate seamless communication and care coordination among all stakeholders involved in a patient’s care journey. Additionally, blueBriX’s patient engagement tools can empower patients to take a more active role in their health management by providing them with educational resources, appointment reminders, and tools for self-monitoring health conditions.
Telehealth for improved chronic disease management
A medical group implemented a PHM program focused on improving chronic disease management for its diabetic patient population. The program utilized telehealth consultations facilitated by a platform similar to blueBriX. Patients could schedule remote consultations with their physicians or diabetes educators, receive medication management support, and participate in virtual group education sessions. The program led to improved patient engagement, better glycemic control, and reduced healthcare costs.
3. Preventive care and early intervention
Early detection and intervention are crucial for preventing disease progression and improving patient outcomes. PHM strategies should emphasize preventive care measures and screenings tailored to the specific needs of each patient population. blueBriX’s patient engagement tools can be used to send automated appointment reminders for preventive screenings, such as mammograms or colonoscopies. Additionally, educational content about healthy lifestyle choices and disease prevention can be delivered directly to patients through blueBriX’s communication platform.
4. Social determinants of health integration
Social determinants of health (SDOH) such as income, education, and housing have a significant impact on health outcomes influencing 30-55% of overall health. A comprehensive PHM program should consider SDOH and connect patients with relevant community resources. The ideal digital health platform can be used to screen patients for SDOH needs and integrate with social service agencies and community groups to facilitate referrals and resource access. Such agencies and group help:
• Improving Resource Accessibility
• Encouraging Health Education and Outreach
• Focusing on Health Disparities
• Creating Customized Interventions
• Campaigning for Policy Change
• Measuring and evaluating population health
The above population health management strategies will help healthcare providers to achieve significant improvements in patient outcomes amongst a larger population. blueBriX’s digital health solutions can play a critical role in supporting each of these strategies and empowering healthcare organizations to deliver exceptional population health management programs.
Empowering population health management with blueBriX
As discussed above, aligning unique strategies with advanced tools is crucial for success. blueBriX offers a suite of digital solutions that empower healthcare providers to implement these strategies effectively. Our comprehensive platform integrates various health apps, including diabetic patient companions and telemedicine solutions, facilitating seamless patient management. BlueBriX comes with many highly customizable pre-built modules to manage clinical workflow, adherence monitoring, and remote monitoring, enable providers to track and manage patient health data efficiently.
Through device integration, blueBriX ensures real-time health data collection from wearables, which is vital for proactive health management. Our advanced behavior change algorithms improve medication adherence and encourage healthier lifestyles, enhancing long-term patient engagement.
blueEHR, our customizable EHR solution, supports personalized patient data management, while blueIntelligence offers analytics and reporting insights to track outcomes and optimize care. Interoperability across systems ensures a holistic view of patient health, improving care coordination.
Additionally, blueNotes supports clinical documentation and personalized treatment plans, while central billing streamlines financial processes, freeing up resources for PHM activities. Our bluePatient App and patient portal enable patients to actively engage in their care by providing access to health data, video consultations, and seamless device integration for comprehensive management.
Conclusion
Population health management is a data-driven approach to healthcare that focuses on improving the overall health of a defined population. By implementing effective PHM strategies, healthcare providers can identify at-risk individuals, intervene early, and deliver coordinated care, ultimately leading to better patient outcomes and lower healthcare costs. blueBriX’s suite of digital health solutions can be a valuable asset for any healthcare organization looking to implement a successful population health management program.
Conclusion
Population health management is a data-driven approach to healthcare that focuses on improving the overall health of a defined population. By implementing effective PHM strategies, healthcare providers can identify at-risk individuals, intervene early, and deliver coordinated care, ultimately leading to better patient outcomes and lower healthcare costs. blueBriX’s suite of digital health solutions can be a valuable asset for any healthcare organization looking to implement a successful population health management program.