

Healthcare fragmentation is not an abstract inefficiency. It has a measurable cost. Research published in the American Journal of Managed Care found that patients receiving care from high-fragmentation providers faced $4,542 higher annual healthcare spending compared to those with low-fragmentation care — and significantly higher rates of preventable hospitalisation. A 2025 analysis of 21,876 adults from the Medical Expenditure Panel Survey found that high fragmentation affected 57.9% of the adult population, with costs rising disproportionately among patients with multiple chronic conditions.
These figures exist because fragmentation is not primarily a cultural or attitudinal problem. It is an infrastructure problem. Data silos, disconnected workflows, and misaligned incentives are not fixed by mission statements or care coordination training alone. They are fixed by the underlying technology systems either enabling or preventing the connections that coordinated care requires. This article examines where those connections break down, what the consequences are when they do, and what integrated infrastructure needs to provide to make coordinated care operational rather than aspirational.
What causes healthcare fragmentation? 4 root factors
To effectively combat fragmentation, we must first understand its origins. It’s rarely a single culprit but rather a complex interplay of interconnected factors deeply embedded in the US healthcare landscape.
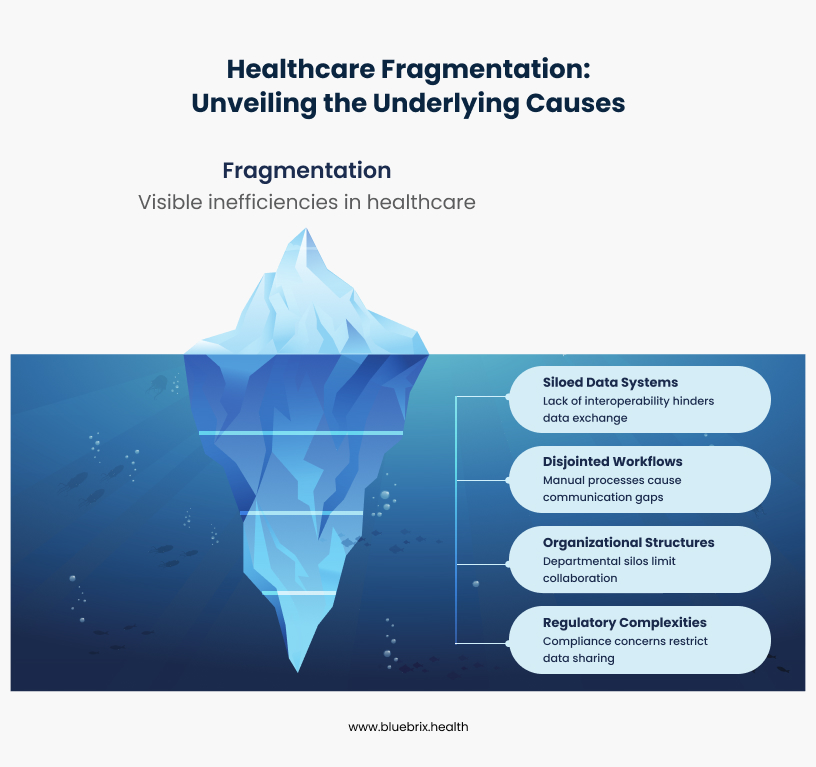
1. Siloed data systems
While Electronic health records were introduced with the promise of digitalization and efficiency, they’ve often become paradoxically part of the problem.
- Proprietary systems and interoperability challenges: A significant challenge in the US is the prevalence of diverse, proprietary EHR systems from various vendors (e.g., Epic, Cerner, Meditech, athenahealth). Each vendor often uses its own data structures and formats, making it incredibly difficult for different systems to “talk” to each other seamlessly. This lack of true plug-and-play interoperability means a patient’s record in one hospital’s EHR often cannot be easily accessed or understood by another hospital using a different system, or even by an outpatient clinic using a separate EHR.
- Lack of standardization in data formats: Even when data is digital, the absence of universal, strict standards for how clinical information (like lab results, medication lists, or diagnoses) is represented further exacerbates the problem. Imagine trying to integrate patient data where one system records blood pressure as “BP,” another as “Blood Pressure,” and a third uses “Systolic/Diastolic” in separate fields – the data simply isn’t consistently structured for easy exchange.
- The “My system” mentality and data blocking: A cultural and sometimes even competitive hurdle exists where individual healthcare facilities or health systems prioritize their own internal systems and data “ownership” over a collaborative, system-wide approach to data sharing. The issue of information blocking, where healthcare providers or IT vendors knowingly and unreasonably interfere with the access, exchange, or use of electronic health information, has been a significant concern, leading to regulatory efforts by the ONC (Office of the National Coordinator for Health Information Technology) to curb this practice.
2. Disjointed workflows and communication gaps
Beyond data, the way healthcare is delivered is often riddled with inefficiencies:
- Manual processes and paper-based handoffs: Despite technological advancements, many critical patient handoffs, referrals, and information exchanges still rely on manual, paper-based processes or faxes, even in large health systems. This is not only time-consuming but also highly susceptible to errors, delays, and lost information, such as missed follow-up appointments after an emergency room visit.
- Lack of centralized communication platforms: Healthcare teams, even within the same organization, often communicate through fragmented channels – phone calls, unsecured emails, faxes, and even personal messaging apps. This lack of a secure, centralized, and auditable platform makes it challenging to track conversations, ensure information reaches the right person at the right time (e.g., during shift changes), and maintain a comprehensive communication log.
- Inefficient scheduling and referral management: Booking appointments across multiple specialties or referring a patient to an external specialist can be a cumbersome, manual process involving phone calls, faxes, and long wait times. This leads to delays in care, patient frustration, and revenue leakage for practices.
3. Organizational structures and cultural barriers
The very structure and culture within US healthcare organizations can inadvertently contribute to fragmentation:
- Departmental silos and lack of cross-functional collaboration: Departments often operate in isolation, focusing on their specific functions rather than viewing the patient journey holistically. For example, a hospital’s discharge planning team might not have direct, real-time communication with the patient’s primary care provider, leading to poor post-discharge follow-up.
- Resistance to change and adoption of new technologies: Implementing new systems and workflows requires significant change management. Resistance from staff due to fear of the unknown, a perceived increase in workload, lack of adequate training, or simply a preference for established (even if inefficient) methods can be a major barrier.
- Insufficient training and support for digital transformation: Even with the best technology, inadequate training and ongoing support can lead to low adoption rates, user frustration, and a failure to realize the full potential of digital tools, resulting in underutilized features and continued reliance on old, fragmented processes.
4. Regulatory and compliance complexities
While regulations like HIPAA (Health Insurance Portability and Accountability Act) are vital for protecting patient privacy and ensuring data security, their complexity can sometimes inadvertently create perceived barriers to legitimate data sharing. Healthcare organizations often err on the side of caution, leading to reluctance in sharing information even when legally permissible and clinically beneficial. Efforts like the 21st Century Cures Act aim to clarify and enforce interoperability and prevent information blocking.
How does fragmented care affect patients, providers, and organizations?
The cumulative impact of these fragmented systems and workflows extends far beyond mere inconvenience. It can have severe, even life-threatening, consequences across the entire healthcare ecosystem.
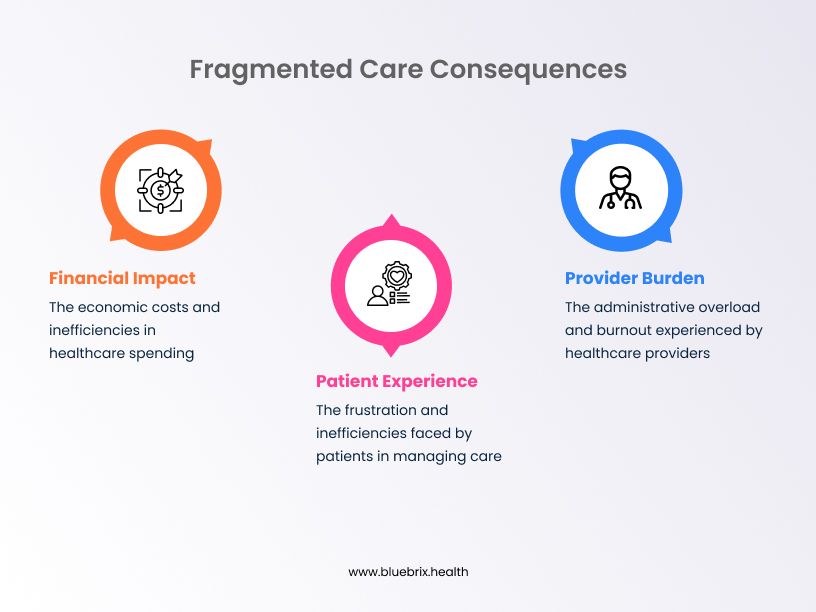
For patients
- Delayed or missed diagnoses: Critical information scattered across different providers can lead to a delay in connecting crucial symptoms or test results, postponing essential diagnoses and interventions. A patient visiting an ER might have vital information in their PCP’s EHR that the ER physician can’t access, leading to an incomplete clinical picture.
- Medication errors and adverse events: Without a consolidated, real-time view of a patient’s complete medication list, allergies, and existing conditions, the risk of prescribing errors, adverse drug interactions, or contraindications increases significantly. This is a leading cause of preventable harm in healthcare.Preventable adverse drug events are estimated to cost between $37.6 billion and $50 billion in added healthcare costs, disability, and lost productivity annually.
- Duplicative tests and unnecessary procedures: When information isn’t readily shared, patients frequently undergo repeated diagnostic tests (e.g., blood work, imaging scans like MRIs or CTs) or procedures simply because the new provider isn’t aware of previous ones. This leads to unnecessary costs for patients and payers, increased radiation exposure, and discomfort.
- Poor adherence to treatment plans: Patients can become overwhelmed and disengaged when their care plan is disjointed, receiving conflicting advice or struggling to coordinate appointments across multiple specialists. This often leads to lower adherence to prescribed treatments and ultimately, poorer health outcomes.
- Erosion of trust and dissatisfaction: The constant friction, inefficiency, and feeling of being “just a number” erode patient trust in the healthcare system. This leads to dissatisfaction, negative patient reviews, and a reluctance to seek necessary care, impacting patient loyalty and health-seeking behaviors.
For healthcare providers
- Increased administrative burden and documentation overload: A significant portion of a clinician’s day can be consumed by administrative tasks – searching for patient information, chasing down lab results, calling other providers, and inputting redundant data into multiple systems – instead of focusing on direct patient care. This is a major driver of physician burnout.
- Missed patient information and incomplete records: The inability to access a complete and accurate patient history due to fragmented records can lead to suboptimal clinical decisions, increased diagnostic uncertainty, and potential safety risks, especially in emergency situations or complex cases.
- Communication breakdowns and misunderstandings: Ambiguous, delayed, or missed communication between care team members (e.g., during patient handoffs from the ICU to a general ward, or between primary care and specialists) can result in critical errors, impacting patient safety and care quality.
- Legal and compliance risks: Incomplete documentation, failure to share critical information, or breaches in data security due to uncontrolled sharing methods can expose healthcare organizations to significant legal liabilities, malpractice claims, and non-compliance penalties from regulatory bodies.
- Burnout and decreased job satisfaction: The constant struggle against inefficient, fragmented systems, coupled with overwhelming administrative tasks, takes a heavy toll on healthcare professionals. This leads to high rates of burnout, compassion fatigue, and a decline in overall job satisfaction, contributing to workforce shortages.Prior authorisation — one of the most friction-heavy administrative processes created by fragmented payer-provider systems — alone accounts for 13 hours per week of physician and staff time, across an average of 39 requests per week, according to the AMA’s 2024 Prior Authorization Physician Survey.
For healthcare organizations
- Financial losses due to inefficiency and rework: The costs associated with duplicated services, wasted resources (e.g., unnecessary supplies for repeated tests), administrative overhead due to manual processes, and penalties for poor outcomes (e.g., readmission penalties) can be substantial, directly impacting an organization’s bottom line.
- Reduced patient throughput and capacity issues: Inefficient workflows lead to longer wait times for appointments, delayed patient discharges, and ultimately, a reduced capacity to serve more patients effectively, impacting revenue and access to care.
- Damaged reputation and loss of patient loyalty: In an increasingly competitive and patient-centric healthcare market, organizations known for fragmented, disjointed care risk losing patient trust and loyalty to competitors offering a more seamless and integrated experience. This can directly impact patient volume and market share.
- Hindered innovation and growth: The energy and resources spent on managing fragmented, legacy systems detract from an organization’s ability to innovate, adopt new value-based care models, invest in advanced technologies, and strategically expand its services to meet evolving community needs.
But there is a good news! There’s a powerful and growing movement towards coordinated care – a holistic, integrated approach that seeks to bridge these gaps, ensuring that all aspects of a patient’s care are connected and aligned.
How can healthcare organizations eliminate care fragmentation?
The regulatory framework for addressing fragmentation has shifted materially since 2022. Three developments are directly relevant to any organisation evaluating how to close its coordination gaps:
The 21st Century Cures Act information blocking rule, now actively enforced by ONC, prohibits healthcare providers and IT vendors from knowingly interfering with the access, exchange, or use of electronic health information. Enforcement actions began in 2023. Organisations whose systems cannot produce patient data on request — to patients, to other providers, or to authorised third parties — now face regulatory liability, not just operational inconvenience.
The CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F), effective January 1, 2026 for most provisions, requires payers to implement FHIR-based APIs for prior authorisation and patient data exchange. For provider organisations, this means the payers funding the majority of services are moving to electronic, standards-based data exchange. Providers whose EHR infrastructure cannot connect to FHIR-based payer APIs will absorb the manual processing costs that electronic exchange is designed to eliminate.
CCBHC quality measure reporting, mandatory from calendar year 2025 under SAMHSA’s 2023 updated certification criteria, requires CCBHCs to capture and submit quality measure data — including care coordination metrics — on a defined schedule. Fragmented data capture at the point of care directly undermines the quality reporting these organisations are now required to produce.

1. Use standardized APIs and FHIR to break down data silos
This is the foundational element of connected care. Without the ability to seamlessly exchange patient information, true coordination remains elusive.
- The role of standardized apis (application programming interfaces): APIs act as sophisticated bridges between different software applications, allowing them to communicate and share data securely and efficiently. By adopting standardized APIs, healthcare systems can unlock their data, making it programmatically accessible to authorized users and applications, moving beyond batch file transfers to real-time data exchange.
- FHIR (Fast healthcare interoperability resources) as new standard: FHIR is rapidly emerging as the global and de facto standard for exchanging healthcare information electronically. It’s designed to be flexible, developer-friendly, and to facilitate real-time data sharing through modular “resources” (e.g., Patient, Observation, Medication). The 21st Century Cures Act strongly promotes FHIR as the basis for interoperability, mandating its adoption for certified EHRs.
- Data warehousing and analytics for holistic views: Beyond real-time exchange, consolidating and normalizing data from various disparate sources into a central, cloud-based data warehouse (often a Health Data Platform) enables powerful population health analytics. This allows organizations to gain a holistic, longitudinal view of patient populations, identify trends (e.g., chronic disease prevalence), stratify risk, and make data-driven decisions for improving care delivery and population health management initiatives.
- Centralized patient portals and shared records: Empowering patients with a single, secure, and user-friendly portal to access their complete health records, schedule appointments, request refills, and communicate with their care team fosters transparency and active participation in their own care. Initiatives like the CommonWell Health Alliance and Carequality in the US are working to establish networks for shared medical records among participating organizations.
2. Get digital tools to streamline clinical workflows for care coordination
Technology must be strategically applied to transform disjointed, manual processes into smooth, integrated workflows that follow the patient’s journey.
- Digital patient intake and onboarding: Moving away from clipboards and paper forms, digital intake solutions streamline the patient registration process, capture accurate demographic and clinical information upfront, and integrate it directly into the patient’s electronic record, reducing administrative burden and errors.
- Automated appointment scheduling and reminders: Advanced online scheduling platforms, often integrated with EHRs, reduce no-shows, optimize clinic capacity, manage waitlists, and provide convenience for patients through automated text or email reminders.
- Electronic referrals and consultations: Secure, integrated electronic referral systems ensure that patient information, clinical notes, and specific referral questions are transmitted seamlessly and securely to the appropriate specialist, reducing delays, lost paperwork, and ensuring proper handoffs.
- Secure messaging and collaboration platforms: Integrated communication tools within EHRs or dedicated, HIPAA-compliant platforms allow care teams (e.g., physicians, nurses, social workers, case managers) to communicate securely, in real-time, about patient care. This ensures everyone is on the same page, especially during complex cases or transitions of care.
- Task management and workflow automation tools: Automating repetitive administrative tasks, such as insurance eligibility verification, prior authorizations, prescription refills, or even patient outreach for preventive screenings, frees up staff time, reduces errors, and accelerates critical processes.
3. Building a care coordination culture beyond technology
Technology is merely an enabler; a deeply collaborative culture is the essential engine that drives its successful adoption and sustained impact.
- Cross-departmental training and workshops: Breaking down organizational silos requires a conscious and sustained effort. Regular training and workshops that bring together different departments to understand each other’s roles, challenges, and the collective benefits of integrated workflows can be transformative. This includes interdisciplinary grand rounds and shared learning opportunities.
- Establishing clear communication protocols: Defining standardized communication channels, escalation procedures, and expectations ensures that critical information flows efficiently, effectively, and transparently across the entire care continuum, from inpatient to outpatient settings.
- Promoting a patient-centric mindset: Reorienting the entire organization around the patient’s comprehensive journey, rather than individual departmental or specialist functions, helps foster a collective commitment to coordinated care and shared accountability for patient outcomes.
4. Use AI, telehealth, and remote monitoring as care coordination enablers
The ongoing digital health revolution offers even more powerful tools to enhance and solidify coordinated care, pushing beyond basic data exchange.
- AI and machine learning for predictive analytics and Risk stratification: AI algorithms can analyze vast amounts of structured and unstructured patient data (e.g., EHR notes, lab results, claims data) to identify at-risk patient populations for specific conditions (e.g., readmissions, chronic disease exacerbations), predict potential health issues, and enable proactive interventions. This shifts healthcare from a reactive “fix-it” model to a proactive, preventative approach.
- Telehealth and remote patient monitoring for continuity of care: These technologies extend care beyond the traditional clinic walls, enabling virtual consultations, continuous monitoring of vital signs and biometric data for patients with chronic conditions, and proactive management of health. This is particularly vital for improving access to care in rural or underserved areas of the US.
- Mobile health applications for patient engagement: User-friendly, secure mobile apps empower patients to actively manage their appointments, access their health information, track their progress, adhere to medication schedules, and communicate directly and securely with their care team, significantly increasing engagement and self-management capabilities.
blueBriX's role in building a coordinated care ecosystem
The problems documented in this article including medication errors from fragmented records, duplicate testing from inaccessible prior results, preventable hospitalisations from poor care transitions, and administrative overhead from disconnected payer-provider workflows all share a common infrastructure root. Solving them requires a platform where data capture, exchange, and clinical decision support operate as a single integrated system, not as connected modules from different vendors.
- blueBriX is built on a FHIR R5 architecture and not a legacy EHR platform with a FHIR layer added. This matters because the infrastructure gap between a FHIR-native system and a retrofitted one becomes visible at exactly the moments where fragmentation is most costly: real-time medication reconciliation at care transitions, quality measure data capture at the point of care for CCBHC reporting, prior authorisation API connections under CMS-0057-F, and Bulk Data exports for HRSA UDS+ submissions. Each of these requires not just the ability to format data in FHIR, but the underlying data model to be structured around FHIR resources from the point of capture.
- On the AI side, blueBriX operates on a human-in-the-loop principle: the AI agent suggests, the contract validates, the workflow executes. This architecture is a compliance posture. For organisations subject to CCBHC quality measure accuracy requirements, payer audit review, or OIG oversight, AI-generated documentation that is not reviewed and validated before submission creates liability. blueBriX’s Trust Engine enforces the validation step as a structural requirement, not as a user option.
- blueBriX is live in production with Immunet, Florida SHOTS, and CAIR, the three state and regional immunisation registries, demonstrating real-world FHIR exchange across diverse systems. For organisations evaluating whether a platform’s interoperability claims extend beyond demonstration environments, production evidence with named systems is the relevant test.
Where care coordination is heading in 2026 and beyond
The direction of federal policy on care coordination is unambiguous. The permanent CCBHC state plan benefit established by the Consolidated Appropriations Act of 2024, mandatory CCBHC quality measure reporting beginning calendar year 2025, the CMS-0057-F prior authorization rule taking effect in 2026, and ONC’s active enforcement of information blocking provisions are all moving in the same direction: towards a healthcare system where data exchange is a baseline requirement and where care coordination failures carry regulatory and financial consequences, not just clinical ones.
The organisations best positioned for this direction are those that have already moved their coordination infrastructure from aspirational to operational — where data flows without manual intervention, where care transitions are tracked in real time, where quality measures are captured at the point of care rather than abstracted retroactively, and where AI tools surface coordination gaps before they become clinical or financial failures.
The gap between where most organisations are today and where federal policy is pointing is, at its core, an infrastructure gap. The clinical vision for coordinated care has existed for decades. The regulatory pressure to achieve it is now structural. The remaining variable is whether the technology foundations are in place to make it operational.