
Healthcare organizations across the United States are facing an unprecedented economic challenge. With annual healthcare spending exceeding $4.3 trillion and 20-40% of that classified as waste, the industry desperately needs solutions that don’t just improve care—they fundamentally transform how healthcare economics work. Enter Fast Healthcare Interoperability Resources (FHIR), a game-changing standard that’s not just about connecting systems, but about unlocking massive economic value across the entire care continuum.
The economic case for FHIR is not theoretical — it is grounded in documented savings across administrative burden, prior authorisation processing, and care coordination costs. The figures in this article are drawn from federal regulatory projections, peer-reviewed research, and named institutional sources. Where a specific dollar figure is cited, its source is identified. But this is just the beginning of a much larger economic transformation that could reshape healthcare delivery as we know it.
Annual Healthcare Cost Savings Potential Through FHIR Interoperability Implementation
The $935 billion problem: understanding healthcare's economic crisis
Before diving into FHIR’s economic impact, we need to understand the scope of healthcare’s cost crisis. The United States spends more per capita on healthcare than any other developed nation, yet ranks poorly in health outcomes. According to a landmark 2019 study in the Journal of the American Medical Association (JAMA), this inefficiency results in an estimated $760 billion to $935 billion in annual waste. The root cause? A fragmented system where fewer than one in three hospitals can electronically find, send, receive, and integrate patient information from other providers.
This fragmentation creates a cascade of economic inefficiencies:
- Administrative complexity accounts for more than $265 billion in wasteful annual spending, driven significantly by fragmentation across payers, coding systems, and billing requirements, according to the JAMA 2019 waste analysis.
- The National Academy of Medicine estimated that billing and insurance-related costs account for 8.5% of hospital care spending and 13% of physician care spending in the United States.
- The reported cost of medical errors is wide-ranging — some experts estimate $20 billion each year while others approximate costs of $35.7 to $45 billion annually for hospital-acquired infections alone, according to StatPearls / NCBI (updated February 2024). Separately, the JAMA 2019 study estimates failure of care delivery — which includes preventable errors — at $102–166 billion annually.
- Physicians and their staff spend an average of 13 hours per week completing prior authorisation requests — across an average of 39 requests per physician per week.
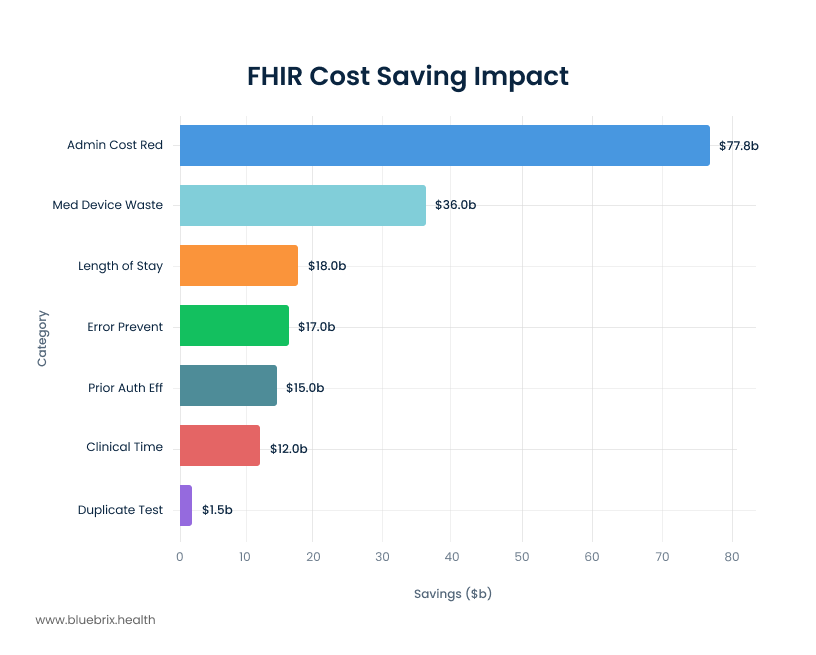
- The West Health Institute identified that widespread medical device interoperability could eliminate at least $36 billion in waste from inpatient settings — through reductions in adverse events ($1.9 billion), redundant testing ($1.5 billion), clinician time on manual data entry ($12 billion), and shorter length of stay ($18 billion).
The healthcare interoperability solutions market was valued at approximately $4.77 billion in 2024 and is projected to grow at a double-digit CAGR through 2029, driven by federal mandates under the 21st Century Cures Act and the CMS Interoperability and Prior Authorization Final Rule.
FHIR's unique position to drive economic value
FHIR represents more than just a technical standard—it’s an economic catalyst that transforms healthcare’s cost structure. Unlike previous interoperability attempts that were complex and expensive to implement, FHIR leverages modern web technologies to create a cost-effective, scalable foundation for data exchange.
The inherent design of FHIR positions it uniquely to drive substantial economic value across the healthcare spectrum. By providing a standardized means for representing and sharing information, FHIR ensures consistency regardless of how local EHRs may store their data. This consistency is paramount for reducing discrepancies and errors, which directly translate into tangible cost savings.
The ability to access data in real-time fundamentally transforms healthcare operations. It enables faster, more informed clinical decision-making, allowing providers to act swiftly and accurately. Moreover, this real-time capability streamlines administrative tasks, reducing the manual effort and associated costs. FHIR’s adoption of common web standards (RESTful APIs, JSON) and its modular “resource” approach makes it inherently easier for developers, including those outside traditional healthcare IT, to build and integrate applications. This ease of use, combined with its “free to use” status and major vendor support, creates a powerful network effect. The simplicity and accessibility of FHIR are not merely technical advantages; they are economic accelerators. By lowering the barrier to entry for innovation, FHIR fosters a more competitive and dynamic health tech market, driving down the cost of developing and integrating new solutions, and ultimately benefiting healthcare organizations through a wider array of affordable, interoperable tools.
Furthermore, FHIR’s role in creating a “single source of truth” for patient data and standardizing its representation, irrespective of local EHR storage methods, directly addresses the pervasive problem of fragmented data and inconsistencies that plague current systems. This capability is foundational to unlocking systemic cost savings. It moves beyond mere data exchange to data cohesion, which is essential for accurate diagnoses, reduced errors, and efficient resource allocation across the entire care continuum. This semantic interoperability represents a higher-order benefit than simple data transfer, enabling a truly unified and efficient healthcare environment.
Breaking down the $51+ billion opportunity
When the savings categories most directly addressable through interoperability are added together — the $36 billion in medical device waste identified by the West Health Institute, the $15 billion in projected prior authorisation savings from the CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F), and a conservative share of the $265 billion in administrative complexity waste documented in the JAMA 2019 analysis — the addressable opportunity comfortably exceeds $50 billion annually. This is not a figure drawn from a single external study. It is the aggregate of the specific, sourced categories discussed in this article.
Administrative cost reduction: the biggest win
Administrative complexity is the single largest category of waste in US healthcare, accounting for an estimated $265 billion annually according to the JAMA 2019 analysis — more than pricing failures, overtreatment, or fraud. A significant share of this waste is attributable to processes that interoperability directly eliminates: manual data entry, phone-based record requests, fax-based document transfer, and redundant data collection across disconnected systems. Organisations deploying health information exchange technology begin reducing these specific, measurable administrative burdens within months of implementation — as the prior authorisation and HIE evidence below demonstrates.
Medical device waste elimination: $36 billion opportunity
One of the most significant and well-documented cost drivers in healthcare is the duplication of diagnostic tests — lab work, imaging studies, and specialised screenings — when patients transfer between facilities or consult multiple specialists without accessible prior records.
The West Health Institute identified that widespread medical device interoperability could eliminate at least $36 billion of waste in inpatient settings through four specific mechanisms: reducing adverse events through safety interlocks ($1.9 billion), eliminating redundant testing ($1.5 billion), reducing clinician time on manual data entry ($12 billion), and shortening length of stay through faster information transmission ($18 billion).
The evidence on redundant testing is independently supported by peer-reviewed research. A study published in the American Journal of Managed Care, examining the Rochester Regional Health Information Organization in New York, found that providers using the HIE were 25% less likely to perform the same imaging test again within 90 days. A separate peer-reviewed analysis of ED settings in Western New York, published in the Journal of the American Medical Informatics Association, found that querying the HIE database led to a 25–26% reduction in laboratory tests and radiology examinations. In one ED setting, the reduction in radiology examinations reached 47%.
Prior authorization: from manual burden to automated efficiency
Prior authorization represents one of healthcare’s most expensive and time-consuming administrative processes. The AMA’s 2024 Prior Authorization Physician Survey found that physicians and their staff spend an average of 13 hours per week completing prior authorisation requests, across an average of 39 requests per physician per week. 89% of physicians report that prior authorisation leads to patient care delays, and 94% say it contributes to burnout.
CMS projects that automating prior authorizations through FHIR-based APIs could save the industry approximately $15 billion over ten years under the Interoperability and Prior Authorization Final Rule (CMS-0057-F). FHIR-based prior authorization solutions replace week-long manual approval cycles with real-time decisions, reduce claim rejections through better documentation, and directly reduce the 13-hour weekly burden on physician staff.
Health information exchange: measurable ROI
The economic evidence on health information exchange is among the most robust in the interoperability literature. Research published in Information Systems Research, drawing on nationally representative Medicare data, found that healthcare markets with established operational HIEs saw an average savings of $139 per Medicare beneficiary per year — a 1.4% overall decrease in Medicare spending. In markets where HIE maturity was high and financial incentives were aligned, spending reductions reached 6.7%. Extrapolated nationally, the researchers estimated this would represent a $3.12 billion annual reduction in Medicare spending alone.
New York’s statewide HIE was independently estimated to generate $160–195 million in annual savings, primarily through administrative efficiencies including reduced manual chart pulls, faxes, and record requests.
Clinical efficiency: time equals money
A large-scale descriptive study published in the Annals of Internal Medicine, drawing on data from approximately 100 million patient encounters with 155,000 physicians across 417 health systems, found that physicians spend an average of 16 minutes and 14 seconds per encounter using EHRs — with chart review (33%), documentation (24%), and ordering (17%) accounting for the majority of that time. For specialties such as gerontology, endocrinology, and internal medicine, time per encounter reached 18–22 minutes.
The interoperability argument here is specific: a significant share of that chart review time is spent searching for information that exists in another system and cannot be retrieved automatically. When patient data flows seamlessly across systems — referral notes, lab results, discharge summaries, medication histories — the chart review burden does not disappear, but the time spent locating fragmented records does. Reducing even four to five minutes of retrieval time per encounter across a clinic’s daily patient volume translates to measurable additional clinical capacity.
Minimising medical errors and improving patient safety
The patient safety argument for interoperability is straightforward: when clinicians have complete, accurate, and current patient information at the point of care, the conditions for preventable errors are reduced. Conflicting medication profiles, duplicate prescriptions, and missed allergy alerts are all more likely when patient data is fragmented across systems that do not communicate. The reported annual cost of medical errors ranges from approximately $20 billion to $45 billion, with the higher estimates including the cost of hospital-acquired infections and preventable adverse events across all settings, according to NCBI StatPearls (updated February 2024).
FHIR’s role here is structural rather than clinical: it does not make clinical decisions, but it eliminates the information gaps that make preventable errors more likely. A single, accessible patient record — medication history, allergy flags, prior diagnoses, current care plan — gives every clinician involved in a patient’s care the same starting point.
FHIR in practice: what the economic argument looks like for specific provider types
The economic case for FHIR plays out differently depending on the type of organisation implementing it. The $36 billion in medical device interoperability waste identified by the West Health Institute applies primarily to inpatient acute care settings. The imaging cost reduction examples are most relevant to hospital systems and multi-specialty groups. But the administrative burden argument — prior authorisation processing time, manual data entry, redundant data collection — applies across virtually every provider type, including outpatient specialty clinics.
Behavioral health is a useful example of how the economics scale to smaller provider organisations. Prior authorisation denial rates are disproportionately high for SUD treatment, intensive outpatient programmes, and community mental health services. The AMA’s 2024 prior authorisation survey found that 89% of physicians report prior authorisation leads to patient care delays, and 94% say it contributes to burnout. For any specialty where continuity of care is clinically critical, an authorisation delay carries consequences beyond the administrative cost.
The CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F), effective January 1, 2026 for most provisions, mandates FHIR-based prior authorisation APIs from Medicare Advantage, Medicaid managed care, and CHIP plans. This applies equally to payers funding primary care, specialty medicine, and behavioral health services. Organisations whose EHR platforms are not FHIR-ready cannot take advantage of this shift regardless of specialty — and will continue absorbing the manual processing costs that electronic authorisation is designed to eliminate.
FQHCs and health centres are a further example: HRSA now requires patient-level FHIR-formatted data submission via the UDS+ framework, beginning with the 2023 data year. The organisations best positioned for this requirement are those whose EHR platforms generate compliant FHIR Bulk Data exports natively — not those extracting data manually to meet the format requirement.
Value-based care: FHIR's strategic economic impact
FHIR’s most significant economic impact may be its role in enabling value-based care (VBC) models. As healthcare shifts from fee-for-service to outcome-based payments, organizations need sophisticated data capabilities to succeed:
Quality measure automation
FHIR enables automated quality measure reporting, eliminating the manual processes that traditionally consume significant resources:
- Digital quality measures (dQMs) provide real-time insights instead of retrospective reporting
- Automated HEDIS reporting reduces administrative burden on health plans
- Real-time population health management enables proactive interventions
Risk adjustment optimization
Up to 30% of conditions affecting risk adjustment scores are underdocumented by providers. FHIR-based systems enable:
- Real-time clinical data integration for more accurate risk assessments
- Better documentation through automated prompts and suggestions
- More appropriate reimbursements based on complete patient pictures
Care coordination atscale
FHIR facilitates the kind of seamless care coordination that VBC models require:
- 37% reduction in preventable ER visits through better care coordination
- 25% reduction in hospital readmissions via improved transitions of care
- $83-106 monthly Medicare cost reduction per point increase in care coordination scores
Chronic disease management and preventive care
Chronic conditions represent a massive financial drain on the U.S. healthcare system, accounting for approximately 90% of the nation’s $4.5 trillion in annual healthcare expenditures. VBC models strategically emphasize proactive interventions aimed at preventing disease progression and complications, thereby reducing reliance on more expensive emergency and inpatient care.
FHIR is instrumental in the effective management of chronic diseases, enabling continuous monitoring and dynamic adjustments to care plans. For example, FHIR-enabled systems can seamlessly integrate data from a variety of sources, including wearables and home monitoring devices, into electronic health records (EHRs). This allows care managers to track patient progress in real-time and adjust treatments as needed, ensuring timely and personalized interventions. This advanced integration supports the proactive management of prevalent conditions like diabetes and heart disease, leading to a reduction in hospital admissions and a significant improvement in patients’ quality of life. Studies consistently show that digital health interventions, such as remote patient monitoring, can substantially reduce healthcare utilization for individuals with chronic conditions.
Reducing hospital readmissions and emergency department utilization
Hospital readmissions are a persistent and costly challenge in healthcare, contributing to increased expenditures, significant resource strain, and poorer patient outcomes. In 2018, the U.S. experienced 3.8 million 30-day all-cause adult hospital readmissions, with an average cost of $15,200 per readmission. Notably, conditions such as septicemia, heart failure, diabetes, and COPD collectively accounted for one in five of all readmissions.
VBC models actively leverage data-driven approaches, including predictive analytics and sophisticated care coordination strategies, to minimize both readmissions and unnecessary ED utilization. FHIR’s capacity to facilitate real-time data sharing ensures that providers possess a complete and up-to-date picture of a patient’s health status, thereby significantly reducing the likelihood of avoidable readmissions. A compelling study revealed that remote patient monitoring, made possible by interoperable data exchange, resulted in a remarkable 44% reduction in hospital readmissions and a 38% reduction in emergency room visits for patients managing chronic conditions. Another case study highlighted a 30% reduction in patient hospital readmissions achieved through effective care coordination and the strategic implementation of remote patient monitoring features.
The regulatory imperative: mandating interoperability
The journey to a truly connected healthcare system is being accelerated not just by innovation, but by powerful regulatory mandates. While the clinical and economic benefits of interoperability have long been understood, a series of federal rules have turned the abstract idea of data sharing into a non-negotiable requirement. This regulatory push is fundamentally shifting the incentives for every player in the healthcare ecosystem, from data hoarding to data liquidity.
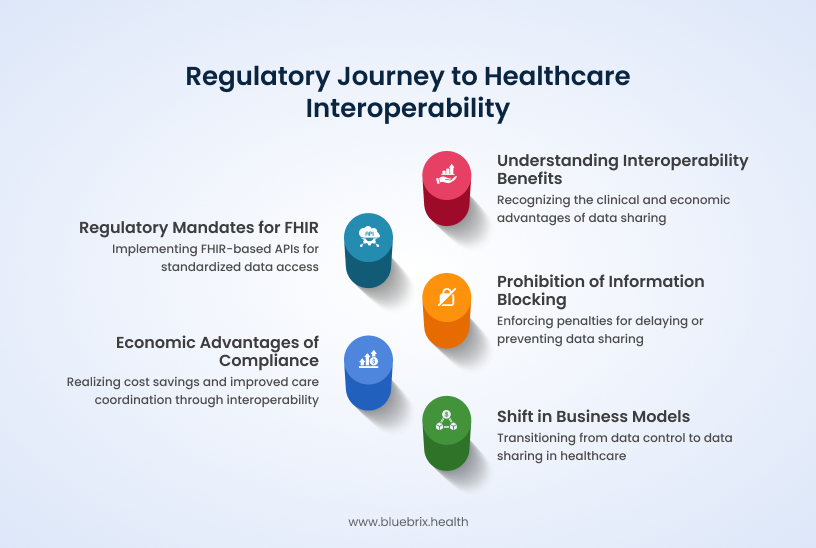
- The mandate for FHIR: Landmark legislation like the 21st Century Cures Act and subsequent rules from the ONC and CMS have mandated the use of FHIR-based APIs. These mandates require health IT vendors, EHRs, and even payers to make patient data available in a standardized, accessible format, creating a baseline level of interoperability across the industry.
- Penalizing information blocking: A core component of this regulatory framework is the explicit prohibition of “information blocking”—the intentional act of delaying or preventing the sharing of electronic health information. The government is backing this with stiff penalties, including fines of up to $1 million per instance for health IT developers and health information networks. This threat of severe financial repercussions creates a powerful incentive to invest in data-sharing solutions.
- From burden to benefit: While regulations can feel like a burden, compliance with FHIR mandates offers significant economic advantages. By embracing interoperability, healthcare organizations can streamline claims processing, reduce operational costs, and improve care coordination. The regulatory pressure is fostering a more competitive market, ultimately leading to lower interoperability costs and a wider array of innovative solutions.
- Reshaping the business model: The ongoing regulatory focus on information blocking signals a fundamental shift in the competitive landscape. It rewards those who embrace interoperability and penalizes those who resist, compelling a change in business models from data control to data sharing—a necessary step for the success of collaborative care and value-based payment initiatives.
Implementation economics: getting started with FHIR
The economic case for FHIR is made in the evidence above. What organisations typically want to understand before committing is what implementation actually costs and what a realistic return looks like. The honest answer is that both depend heavily on where you are starting from.
What FHIR implementation involves — and what it costs
FHIR itself is an open standard maintained by HL7 International. There are no licensing fees for using the FHIR framework. The implementation cost is the cost of connecting your existing systems to FHIR-based APIs — and that cost varies significantly based on your starting point.
At the most basic level — exposing core FHIR resources using an existing EHR vendor’s FHIR endpoint with minimal customisation — costs are relatively contained. At the intermediate level, which includes SMART on FHIR integrations, multiple vendor systems, and workflow alignment, costs rise with the number of integrations and data complexity. Full FHIR ecosystem implementations — multiple EHR vendors, write capabilities, Bulk Data exports, API gateway infrastructure — represent the largest investment.
The most significant cost variable is your current EHR platform. Organisations on a FHIR-native platform — one built on FHIR architecture rather than retrofitted with a FHIR layer — absorb significantly lower implementation overhead than those relying on middleware to translate legacy HL7 v2 feeds into FHIR format. Every translation layer adds cost, complexity, and a potential failure point at each compliance deadline.
ONC’s December 2025 proposed deregulatory rule estimated present-value cost savings of $1.53 billion in 2024 dollars from reducing certification requirements on health IT developers — a figure that reflects how significant the compliance overhead on the vendor side has been, and how the regulatory environment is beginning to account for implementation burden.
What a realistic ROI looks like
No peer-reviewed study currently publishes a universal ROI figure or average payback period for FHIR implementation. The published evidence does, however, quantify several of the specific return categories consistently:
Prior authorisation processing represents one of the most immediate and measurable returns. Moving from manual to FHIR-based electronic prior authorisation eliminates a documented 13-hours-per-week administrative burden per physician practice — with CMS projecting $15 billion in industry-wide savings over ten years from this shift alone under CMS-0057-F.
Redundant testing reduction is the second measurable category. Peer-reviewed research consistently shows 25–47% reductions in repeat laboratory tests and radiology examinations when providers have access to HIE data — a direct, trackable cost reduction from the first month of live data exchange.
Medicare spending at the market level shows a 1.4% overall reduction in healthcare markets with established HIE infrastructure, rising to 6.7% in markets with mature exchange systems and aligned incentives — per peer-reviewed research published in Information Systems Research.
These are the return categories the evidence supports. The aggregate return for any individual organisation depends on their payer mix, current manual process volume, programme type, and how deeply FHIR is integrated into clinical and administrative workflows. A CCBHC with high prior authorisation volume will see faster returns in that category than a private practice with a commercially insured panel. An FQHC facing UDS+ compliance obligations will see immediate value in a platform that generates Bulk Data exports natively versus one requiring manual data extraction.
The question worth asking
The implementation economics question most organisations get wrong is framing it as “what will FHIR cost us to implement” rather than “what is our current non-interoperability costing us.” The $265 billion in annual administrative complexity waste documented by JAMA, the 13 physician hours per week on prior authorisation, and the 1.4–6.7% Medicare spending reduction in HIE-enabled markets are all costs being absorbed right now by organisations that have not yet implemented. The implementation investment is finite. The cost of not implementing compounds with every new federal mandate, every new payer API requirement, and every year of manual processing that could have been automated.
How to conquer FHIR implementation headaches
While FHIR’s economic benefits are substantial, organizations often face implementation challenges that can be addressed through strategic planning.
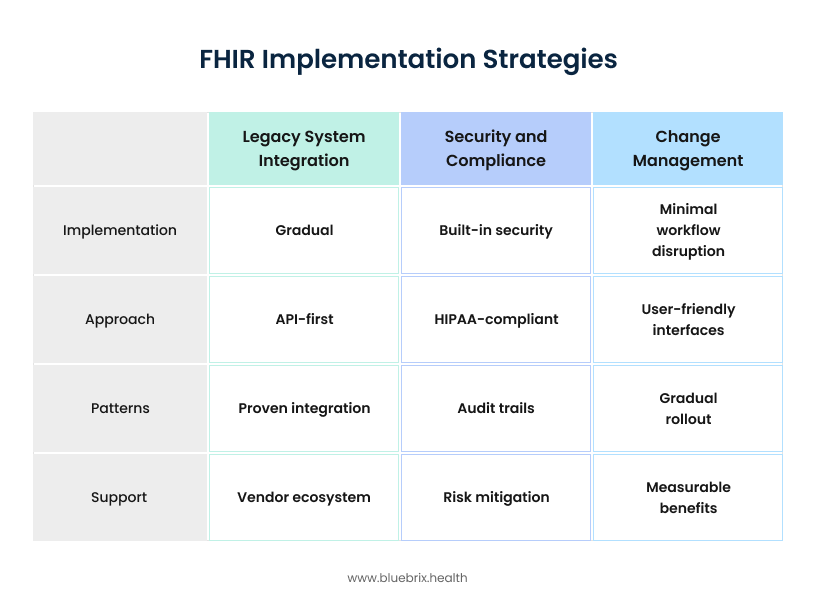
- Data standardization and legacy systems: Many hospitals operate on legacy EHR systems with siloed data stored in non-standard formats, making mapping to FHIR resources complex. Effective solutions involve conducting thorough data inventory and mapping exercises, utilizing middleware platforms or FHIR adapters to translate legacy formats, and implementing a Master Patient Index (MPI) to resolve duplicate records.
- Inconsistent FHIR implementation: Different EHR vendors may implement FHIR resources inconsistently, hindering seamless interoperability. Aligning on the US Core Implementation Guide (IG) and actively engaging with FHIR Accelerators like the Da Vinci Project can provide crucial guidance and promote standardization.
- Security and privacy concerns: FHIR’s open, API-first architecture necessitates robust security measures to prevent data breaches and unauthorized access. Implementing SMART on FHIR protocols with strong OAuth2 authentication, applying role-based access controls (RBAC), and conducting regular penetration testing and security audits are critical safeguards.
- Staffing shortages and lack of FHIR expertise: The implementation of FHIR requires specialized skills in architecture, development, and data analysis, which can be scarce. Investing in FHIR training programs and certifications, partnering with experienced interoperability consultants or health IT vendors, or leveraging low-code/no-code FHIR platforms can address this talent gap.
- Change management and workflow integration: Technical integration alone is insufficient; successful FHIR adoption requires a redesign of clinical workflows to ensure applications are effectively utilized by staff and do not disrupt care delivery. Involving clinical stakeholders early in the design phase, conducting pilot testing with iterative feedback loops, and integrating FHIR apps seamlessly into existing EHR interfaces are essential.
- Versioning and upgrades: FHIR is a dynamic standard, with new versions (R4, R5, and R6 in development) introducing changes. Hospitals must ensure their systems remain compatible over time. Standardizing on normative versions like R4 and implementing robust version control policies are best practices for managing this evolution.
- Upfront investment: Initiating FHIR implementation requires an initial investment of time, dedicated staff, and financial resources. However, the evidence suggests that investing early yields significant long-term returns through improved efficiency and superior patient outcomes.
The high adoption rates among hospitals and clinicians by 2019 and the continued anticipated increase demonstrate a growing momentum. The quantifiable ROI figures from early adopters provide a strong incentive for others. Conversely, the challenges faced by those still relying on legacy systems highlight the increasing cost of not adopting FHIR. Organizations that proactively invest in FHIR implementation are gaining a significant “early adopter advantage” in terms of cost savings and efficiency. Those lagging behind face not only higher operational costs but also increasing competitive disadvantage and potential regulatory non-compliance risks, effectively turning inaction into a growing financial liability.
The challenges section emphasizes “staffing shortages and lack of FHIR expertise” and “change management and workflow integration.” The solutions provided, such as investing in training and involving stakeholders, are not purely technical. This highlights that successful FHIR adoption and the realization of its economic benefits depend heavily on organizational readiness and human factors, not just technology. The ROI of FHIR is not solely dependent on the technology itself, but on the strategic investment in “soft” factors like workforce training, robust change management, and cultivating a culture that values data sharing. These investments are critical for maximizing the quantifiable financial returns and ensuring the long-term success of interoperability initiatives.
Looking forward: the future economics of FHIR
FHIR isn’t a static solution; it’s a dynamic framework that continuously evolves to meet the complex demands of healthcare. While FHIR Release 4 (R4) is the current standard, newer versions like R5 and the upcoming R6 are designed to improve security, streamline workflows, and ensure long-term stability with greater backward compatibility. This constant evolution ensures FHIR’s role as the indispensable foundation for future innovations.
Powering AI and advanced analytics
FHIR is the essential enabler for unleashing the full potential of AI in healthcare. AI models rely on accurate, real-time, and standardized data, which is precisely what FHIR provides. This powerful partnership between FHIR and AI enables several transformative capabilities:
- Predictive analytics: FHIR-fueled AI can identify at-risk patients, allowing providers to proactively intervene and prevent costly complications.
- Clinical decision support: FHIR’s architecture allows AI systems to provide real-time recommendations directly within EHRs, improving diagnostic accuracy and patient outcomes.
- Population health management: By analyzing vast amounts of standardized health data, AI can help organizations identify trends and effectively manage chronic conditions across entire patient populations.
- Personalized medicine: FHIR’s ability to aggregate comprehensive data from multiple systems enables AI to create highly tailored treatment plans, moving healthcare toward a truly personalized approach.
A vision for a truly interconnected ecosystem
The widespread adoption of FHIR is paving the way for a major shift in healthcare, moving from a reactive model of treating illness to a proactive one focused on prevention. By connecting with community-based organizations and incorporating data on social determinants of health (SDOH), FHIR allows for a holistic view of a patient’s well-being. This vision of a “fully digital health system” and “unified data platforms” suggests a future where data flows effortlessly, enabling true care coordination and unlocking new avenues for cost reduction. The economic potential of this ecosystem, fueled by FHIR’s pervasive adoption, is expected to drive substantial growth in the healthcare interoperability market.
As FHIR adoption accelerates, the economic benefits will compound:
Network effects
- Value increases as more organizations connect to FHIR-enabled networks
- Reduced costs for integration as standards become more widespread
- Enhanced capabilities through shared development and innovation
- Industry-wide efficiencies that benefit all participants
Innovation enablement
- AI and machine learning applications powered by standardized, accessible data
- New care delivery models enabled by seamless information sharing
- Patient engagement tools that leverage comprehensive health records
- Population health insights that drive system-wide improvements
Regulatory alignment
- CMS requirements that mandate FHIR adoption for certain programs
- Quality reporting that becomes automated rather than manual
- Public health integration that enables better disease surveillance and response
- Research capabilities that accelerate medical discoveries
Why your EHR's FHIR architecture matters more than you think
The economic case for FHIR only holds if your EHR platform can actually deliver it. Not every platform that describes itself as FHIR-compatible is built the same way. There is a meaningful operational difference between a platform built on a FHIR-native architecture and one that has added a FHIR layer on top of a legacy system. The difference becomes visible at the moments that matter most — a UDS+ submission deadline, a CMS-0057-F prior authorisation API requirement, a payer audit requesting structured clinical data on short notice.
An FHIR-native EHR generates compliant Bulk Data exports without manual extraction workarounds. It supports SMART on FHIR app integrations that connect to third-party clinical and analytics tools without custom interface development. It connects to TEFCA-aligned Qualified Health Information Networks for nationwide data exchange. And it handles the prior authorisation API requirements that most payers are now mandated to support under CMS-0057-F — without your team having to build the bridge between your platform and the payer’s system manually.
blueBriX is built on this architecture. For organisations evaluating whether their current EHR is positioned to meet the interoperability obligations already in effect — and those coming in 2027 — that is the starting point for the conversation.
The economics are clear. The technology is proven. The time is now.
If your organisation is approaching a UDS+ submission deadline, a CMS-0057-F compliance requirement, or an accreditation or quality reporting cycle and you are not confident your current EHR can generate the FHIR output your payers, regulators, or reporting obligations require, that is the right question to bring to a blueBriX consultation. Book a call to walk through your current interoperability infrastructure and where the gaps are.


