

Healthcare is changing, and not slowly. The old “see more patients, bill more services” model is giving way to something that actually makes sense: rewarding providers for better outcomes, smarter care, and lower costs. Programs like ACOs and CMS initiatives are leading that charge, tying reimbursements directly to how well you perform, not just how much you do. But here’s the thing. You can’t make that shift with the wrong tools.
Your EHR sits at the center of all of it. It’s how your care teams coordinate, how you report quality metrics, how you manage risk, and ultimately, how you get paid. And yet, a lot of organizations are still running on systems that were built for a world that no longer exists. If your EHR was designed for fee-for-service, it’s probably quietly working against your value-based care goals, even if everything looks fine on the surface. That’s what this blog is about.
The role of EHR in a successful VBC strategy
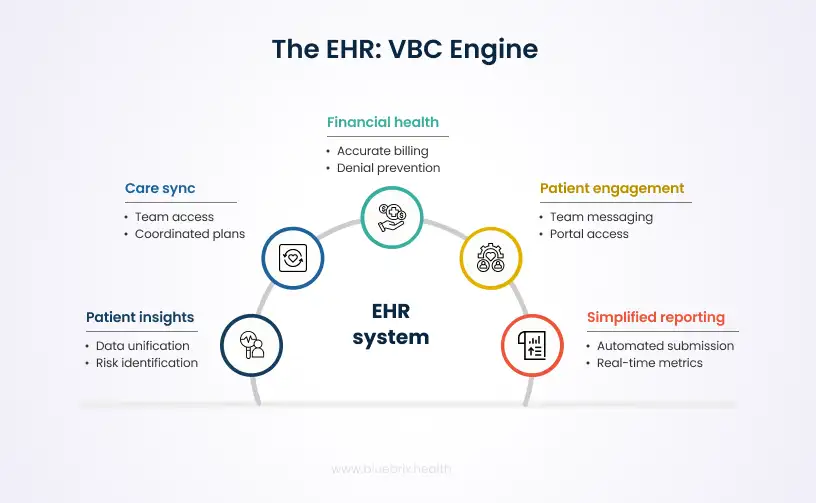
Most people still think of an EHR as a place to store patient notes. But in a value-based care model, it’s a lot more than that. It’s the engine that keeps everything running. As healthcare shifts away from fee-for-service toward outcome-driven reimbursement, programs like ACOs, MSSP, and CMS initiatives such as MIPS and eCQM reporting are fundamentally changing how providers get paid. Success in these models depends on coordinating care across settings, managing patient populations proactively, and demonstrating quality performance through structured data. The EHR sits at the center of all of that, connecting clinical care, operations, quality reporting, and financial performance all at once.
Seeing your patients more clearly
You can’t manage what you can’t measure. A good EHR pulls together clinical, demographic, and behavioral data into one cohesive picture, making it possible to identify which patients are at highest risk before things escalate. Built-in analytics help teams track quality measures like HEDIS and eCQMs, the metrics that value-based contracts are actually scored on, so you’re not scrambling to pull numbers together at reporting time.
Keeping care teams in sync
Gaps in communication are expensive. Duplicate tests, missed handoffs, delayed treatments, they all happen when providers are working from different information. A shared EHR means everyone caring for a patient is on the same page, with access to the same notes, care plans, and task lists. For patients with complex needs, like those receiving behavioral health support alongside primary care, that continuity is not a nice-to-have. It’s what good care coordination actually looks like.
Making reporting less painful
Reporting requirements under value-based contracts can be exhausting if you’re doing them manually. A well-built EHR captures structured data during normal clinical workflows and maps it directly to the metrics you need to submit, whether that’s eCQMs, MIPS measures, or payer-specific requirements. Real-time dashboards mean you can see where you stand before a deadline, not after. Flowsheets and longitudinal tracking tools also help document preventive care activities over time, which matters a lot when those activities are tied to reimbursement.
Protecting your revenue
In a value-based model, financial health depends on accurate, timely documentation. Billing errors, missed codes, and denied claims all eat into the margin. EHRs with integrated revenue cycle tools, including automated coding support, eligibility verification, and denial prevention, help make sure claims go through cleanly the first time. Predictive analytics can also flag reimbursement risks tied to risk adjustment or quality scoring before they turn into actual losses.
Getting patients more involved
Outcomes improve when patients are active participants in their own care. Patient portals give people access to their care plans, test results, and appointment reminders, and let them message their care team directly. That kind of engagement doesn’t just feel good. It shows up in satisfaction metrics and preventive care completion rates, both of which value-based contracts often measure and reward.
Is your current EHR actively undermining your VBC goals?
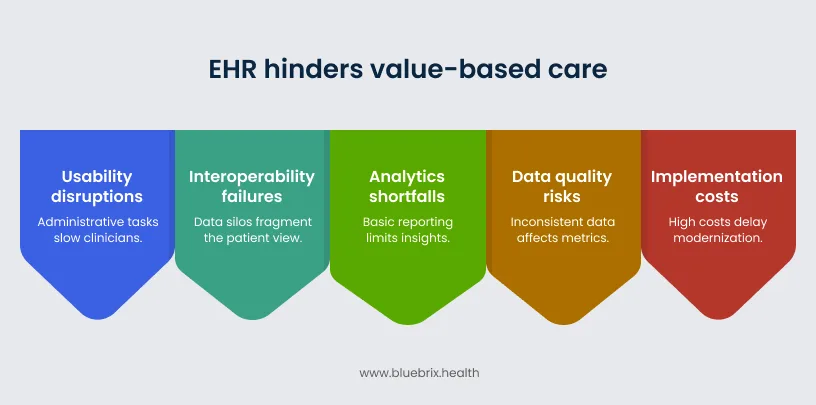
Many healthcare organizations entered the value-based care era carrying EHR systems that were built for a very different time. Most legacy platforms were designed around fee-for-service workflows, focused on documentation, billing, and compliance. As care models shift toward outcomes, care coordination, and population health management, these systems often can’t keep up. The result is a quiet but costly disconnect. Instead of supporting outcomes-driven workflows, your EHR may be introducing friction that slows down clinicians, fragments patient data, and limits the insights you need to manage risk effectively.
Usability and workflow disruptions
One of the most visible problems is poor usability. Many legacy EHR interfaces require clinicians to navigate multiple screens, fill in repetitive documentation fields, and work within rigid workflows that were never designed for modern care delivery. This adds up. The more time clinicians spend on administrative tasks, the less time they have for actual patient care. In value-based care environments where preventive care, care coordination, and patient engagement are directly tied to performance metrics, that lost time has real consequences. Over time, these inefficiencies also contribute to clinician burnout, which compounds the problem further.
Modern EHR platforms are increasingly designed with clinician experience in mind. Streamlined documentation workflows, automated data capture, and integrated care coordination tools reduce the time providers spend navigating administrative tasks. By lowering documentation burden and minimizing system friction, a well-designed EHR can help reduce clinician burnout while allowing providers to focus more on patient care.
Interoperability failures
Value-based care depends on having a complete, continuous view of the patient across providers, care settings, and community services. But many EHR systems still operate in silos. When data can’t move freely between systems, organizations struggle to build accurate population health insights. Care teams may not see visits that happened outside their network. Social determinants of health information often stays disconnected from clinical records. Referral follow-ups become difficult to track. These interoperability gaps make it harder to identify high-risk patients early, coordinate care effectively, and hold up your end of value-based contracts.
Analytics shortfalls
Value-based care requires continuous monitoring of patient populations, quality metrics, and cost performance. Yet many legacy EHR systems offer only basic reporting capabilities. Advanced functions like risk stratification, population health management, and clinical-financial integration are either weak or missing entirely. As a result, organizations end up relying on external tools to fill the gaps, creating fragmented data environments and slowing down decisions that should ideally be happening in real time.
Data quality risks
Value-based reimbursement models are only as good as the data behind them. When clinicians are navigating complex, poorly designed documentation workflows, data entry tends to get rushed or inconsistent. Incomplete or inaccurate records can affect risk adjustment calculations, quality reporting scores, and performance measurement under CMS programs. Even small documentation gaps can translate into missed care opportunities, inaccurate quality scores, or reduced reimbursement. Add to that the data security and privacy challenges that come with sharing patient information across multiple care settings, and the risks compound quickly.
Implementation and operational costs
Even when organizations clearly see the limitations of their current systems, making the switch is not straightforward. High implementation costs, staff training requirements, and the temporary productivity dip that comes with any major system transition can delay modernization for years. For smaller practices or behavioral health providers already operating on tight margins, these barriers can feel insurmountable. So they keep running on technology that was never designed for the performance-driven care models they’re now being held accountable to.
The real cost of inaction: what happens when you do nothing
It’s easy to understand why organizations put off EHR modernization. A system transition is disruptive, expensive, and time-consuming. Staying put feels like the safer call. But in a healthcare landscape increasingly shaped by value-based reimbursement, doing nothing carries its own very real risks. And those risks tend to grow quietly in the background until they’re hard to ignore.
Financial penalties and revenue leakage
Value-based contracts depend on accurate documentation, proper risk adjustment, and reliable quality reporting. When your EHR can’t support those functions well, the financial consequences follow. Organizations may face withheld reimbursements, missed incentive payments, and direct penalties tied to programs like MIPS and other CMS quality initiatives. Coding errors, delayed billing, and claim denials become more frequent when clinical and financial workflows aren’t properly integrated. Over time, these inefficiencies don’t just create administrative headaches. They translate into substantial, compounding revenue loss.
Poor quality reporting and patient outcomes
Quality measurement is at the heart of value-based care. Programs like HEDIS, MIPS, and Star Ratings require organizations to track and report detailed patient outcomes and preventive care activities. Without automated reporting capabilities, staff are left doing manual data abstraction and spreadsheet-based tracking to pull these numbers together. That approach is slow, error-prone, and pulls people away from higher-value work. More importantly, outdated systems often lack risk stratification and clinical decision support tools. High-risk patients may not be flagged early enough. Care gaps go unnoticed. Preventive interventions get delayed. And those delays show up downstream as avoidable emergency visits, hospitalizations, and poorer patient outcomes overall.
Operational burdens and clinician burnout
Inefficient EHR systems create a steady drain on clinicians and administrative teams alike. Complex documentation workflows, multiple system logins, and disconnected platforms force clinicians to spend significant chunks of their day navigating software rather than caring for patients. This administrative burden is one of the leading contributors to clinician burnout, which has become a serious and growing challenge across the healthcare industry. High turnover among physicians and clinical staff creates additional financial and operational pressure, particularly for organizations already managing tight margins under value-based contracts.
Compliance and security risks
Regulatory requirements around interoperability and data sharing are moving fast. Standards like FHIR and policies tied to the 21st Century Cures Act require healthcare organizations to make patient data more accessible and interoperable across systems. Legacy EHR platforms often struggle to meet these requirements, raising the risk of compliance violations or information blocking penalties. At the same time, older systems tend to lack modern security frameworks, making them more vulnerable to threats like ransomware attacks. The consequences go beyond financial penalties. A serious security incident can damage patient trust and disrupt care delivery in ways that are hard to recover from.
Competitive and strategic disadvantages
Organizations that delay EHR modernization also face a growing competitive gap. Providers investing in modern, interoperable platforms gain better visibility into their patient populations, stronger care coordination capabilities, and more efficient reporting for value-based contracts. Patients increasingly expect digital engagement tools and coordinated care experiences across providers. Younger physicians and clinical staff often factor in usability and modern workflows when deciding where to practice. Organizations running on outdated technology may find it harder to retain patients, recruit talent, and participate meaningfully in expanding value-based initiatives like ACOs and risk-based payment models.
Why blueBriX is the right EHR partner for your VBC journey?
Choosing the right EHR is one of the most important technology decisions healthcare organizations make when transitioning to value-based care. The platform must go beyond documentation and support the operational, clinical, and financial requirements of value-based reimbursement models. blueBriX is designed with these needs in mind. Built to support coordinated, outcome-driven care, the platform combines clinical workflows, analytics, interoperability, and revenue management into a unified system that helps organizations succeed in value-based care environments.
Purpose-built capabilities for value-based care
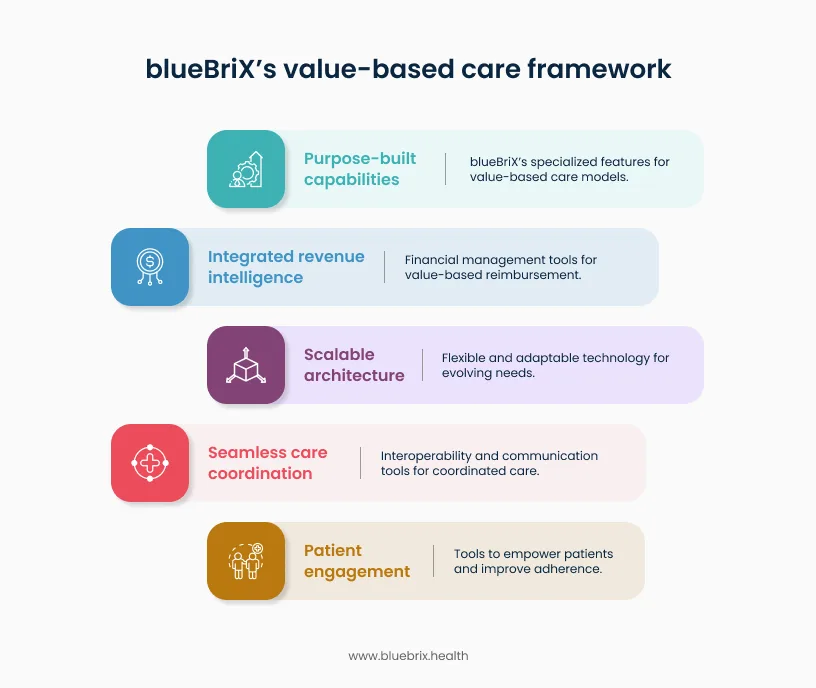
blueBriX is designed to support healthcare organizations operating in value-based models such as Accountable Care Organizations (ACOs), Independent Practice Associations (IPAs), and delegated care entities. The platform integrates clinical, claims, and social determinants of health data into unified patient records, giving care teams a comprehensive view of each patient’s history and risk profile.
Longitudinal patient timelines, care gap identification, and risk stratification tools enable providers to identify high-risk patients and intervene earlier. Real-time performance dashboards and scorecards for measures such as HEDIS and Star Ratings help organizations track progress against quality benchmarks while simplifying compliance with payer and CMS reporting requirements.
Seamless care coordination across the continuum
Effective value-based care requires coordination across multiple providers and care settings. blueBriX includes a centralized care team workbench that brings together tasks, alerts, shared care plans, and patient updates in one place. Through interoperability standards such as FHIR and HL7 APIs, the platform enables secure data exchange across primary care providers, specialists, behavioral health clinicians, and post-acute care teams. Closed-loop referral management and transition-of-care alerts help prevent care fragmentation and ensure that patients move smoothly across the care continuum. Additional capabilities such as remote patient monitoring, telehealth integration, and patient-reported outcomes tracking provide clinicians with greater visibility into patient health between visits.
Integrated revenue and performance intelligence
Financial success in value-based care requires close alignment between clinical performance and reimbursement outcomes. blueBriX integrates revenue cycle management capabilities directly into clinical workflows to support accurate coding, billing, and contract performance monitoring. Built-in revenue intelligence tools provide visibility into payer performance, claim denials, and reimbursement trends. Automated eligibility checks, denial prevention tools, and multi-entity billing capabilities help reduce revenue leakage and improve claim acceptance rates. At the same time, self-service reporting tools allow healthcare organizations to generate audit-ready reports for quality programs, payer contracts, and regulatory compliance requirements.
Patient engagement and AI-driven insights
Patient engagement is a key driver of better outcomes in value-based care. blueBriX supports this through patient portals that enable secure messaging, appointment reminders, and easy access to care plans and clinical information. The platform also incorporates behavioral health engagement tools such as mood tracking and journaling features that support long-term patient adherence. These capabilities are particularly valuable for organizations managing complex or high-risk patient populations. blueBriX also includes an AI-enabled analytics framework designed to support predictive insights and care management workflows. With human oversight built into the system, these AI-driven tools help care teams identify emerging risks, prioritize interventions, and deliver more proactive care.
Scalable and adaptable architecture
Healthcare organizations require technology that can evolve with changing care models and payer requirements. blueBriX is built on a flexible, cloud-based architecture that allows organizations to scale operations without major infrastructure changes. The platform integrates with widely used healthcare and enterprise systems, including leading EHR platforms and CRM solutions, enabling organizations to extend existing technology investments. Customizable workflows and no-code configuration tools allow organizations to adapt the system to their unique programs and care delivery models without requiring extensive development resources.

