The Centers for Medicare and Medicaid Services (CMS) announced the Long-term Enhanced ACO Design (ACO LEAD) model in December 2025 as the direct successor to ACO REACH – the first ten-year ACO model CMS has ever tested, one that introduces prospective capitated payments, stable benchmarks, and expanded access for independent and rural providers[1]. With the January 1, 2027 launch now six months away and Performance Year 2027 applications closed as of May 17, 2026, this guide is for two audiences: the organizations accepted into the first cohort that are now entering the optional pre-implementation period, and the organizations building the foundation for a future cohort application. Both groups need the same operational and financial groundwork – the difference is urgency, not direction.
For the past few years, ACO REACH (Realizing Equity, Access, and Community Health) served as CMS’ primary testing ground for advanced value-based care. Launched in 2023, it introduced critical innovations specifically, a focus on health equity and a shift toward provider-led governance rather than hospital-centric control. However, as a short-term model set to expire at the end of 2026, REACH presented a challenge: its volatility and limited timeline made it difficult for smaller, independent, and rural practices to invest in the necessary long-term infrastructure.
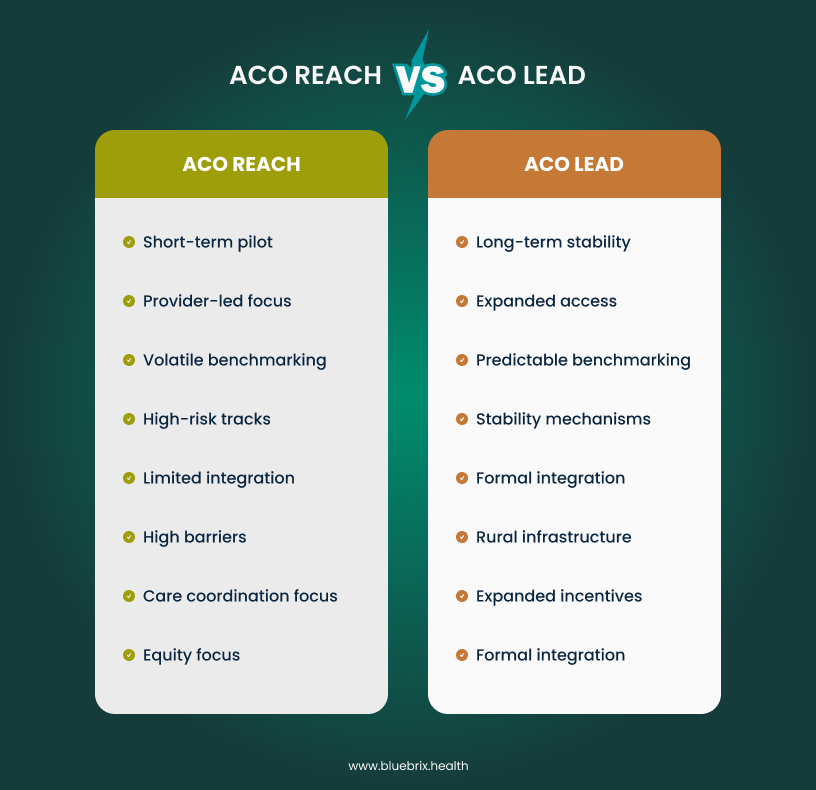
While ACO REACH proved that equity and risk could coexist, ACO LEAD provides the predictability and financial support required to make that model viable for the next decade.
For independent practices, small physician groups, and rural healthcare providers struggling with the complexity of prior ACO models, this announcement signals a critical opportunity. But only for those who understand what makes LEAD different, how to prepare for it, and crucially, how much time they have left to make it happen. If you’re still operating under the assumption that you have “time to think about it,” you’re already behind.
Understanding ACO LEAD: the next generation of accountable care
The ACO LEAD model, which will begin operations on January 1, 2027, is purposefully designed to address the barriers that have discouraged provider participation in advanced value-based care arrangements over the past several years. Rather than continuing with the iterative tweaks that characterized earlier CMS approaches, LEAD represents a comprehensive rethinking of how to make accountable care sustainable for diverse provider types.
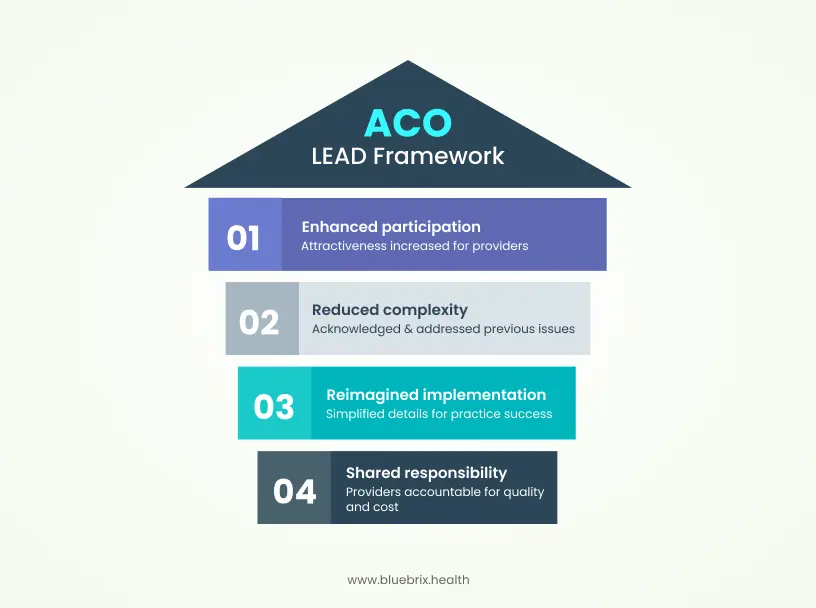
At its core, ACO LEAD maintains the fundamental principle underlying all accountable care organizations: providers accept shared responsibility for both the quality and cost of care delivered to a defined population of Medicare beneficiaries. However, the implementation details have been substantially reimagined. This distinction is critical. CMS leadership explicitly acknowledged that previous ACO models, while well-intentioned, created unnecessary complexity and financial risk that made participation unattractive to many providers, particularly those without large hospital system backing.
The financial architecture: how payment changes in ACO LEAD
One of the most substantive differences between ACO LEAD and its predecessors involves how payments flow to participating providers. ACO LEAD introduces a 10-year performance period with stable benchmarks, a dramatic departure from models that rebased benchmarks periodically. For a practice evaluating whether to participate, this change directly affects cash flow predictability and long-term financial planning.

Prospective capitated payments and monthly cash flow
Rather than waiting for year-end settlement based on actual claims experience, ACO LEAD provides prospective monthly capitation payments. This means practices know in advance what payment they can expect, enabling more confident investment in care infrastructure and staff. The predictability is intentional—CMS heard consistently from providers that retrospective risk arrangements created cash flow volatility that made it nearly impossible to invest in the care coordination capabilities that actually drive better outcomes.
Practices in ACO LEAD will have two voluntary risk-sharing tracks available:
- Global risk track: ACOs can retain up to 100% of savings but bear responsibility for up to 100% of losses relative to an established benchmark. Global ACOs face a benchmark discount of approximately 1.75–3%[2],2 reducing the starting benchmark relative to the Professional track – a trade-off for the maximum savings potential.
- Professional risk track: ACOs can receive up to 50% of savings while assuming responsibility for up to 50% of losses.
This optionality is deliberate. Not every practice has the same tolerance for downside risk, and CMS explicitly rejected the one-size-fits-all mentality that characterized earlier models.
Enhanced financial support for rural and independent providers
Recognizing that infrastructure investment represents a genuine barrier for smaller providers, ACO LEAD includes add-on payments specifically for rural healthcare providers to help them develop the operational foundations necessary for accountable care participation. This is actual financial assistance to offset the genuine costs of implementing the systems and workflows that value-based care requires.
Additionally, providers new to ACOs – a category that disproportionately includes independent practitioners – can participate with patient panel requirements calibrated to their actual organizational scale. The confirmed minimum for standard LEAD participation is 5,000 aligned Medicare beneficiaries per performance year, with at least 3,000 claims-based aligned beneficiaries in at least one base year[3]. High-needs-focused ACOs serving dually eligible, homebound, or complex populations may qualify with lower minimums. A financial guarantee is also required before joining: typically 2% of prior-year Medicare Part A and B revenue for Professional Risk track participants, and 4% for Global Risk participants, to cover potential losses[4]. This is higher than ACO REACH required, reflecting the longer performance period and greater potential payouts in LEAD. For Global Risk ACOs that incur losses but remain in the model, CMS’s Extended Repayment Option allows payback to Medicare over time rather than immediate settlement[5].
Risk adjustment and complex patient integration
Previous ACO models inadvertently created perverse incentives around patient risk. Providers caring for complex, costly populations faced higher benchmarks that were difficult to beat, while those with healthier populations could more easily claim savings. This dynamic discouraged providers from actively engaging with high-needs populations, counteracting the entire purpose of accountable care.
ACO LEAD addresses this through more accurate risk adjustment and enhanced integration of complex patients. CMS has recognized that caring for dual-eligible beneficiaries (those eligible for both Medicare and Medicaid), patients with behavioral health conditions, and individuals with multiple chronic diseases requires different capabilities than managing a general population. Rather than forcing complexity into a standardized framework, LEAD creates specific accommodations.
The model also includes initial planning for Medicare-Medicaid partnerships at the state level, beginning with a planning phase from March 2026 through December 2027. This represents a fundamental shift in how CMS approaches patients who experience fragmentation across two payment systems. For providers serving populations with substantial Medicaid overlap, this coordination capability will ultimately prove more valuable than any single payment mechanism.
Episode-based risk and the specialist coordination problem
A persistent challenge in earlier ACO models involved how to fairly and efficiently coordinate care with specialists. Primary care physicians felt the pressure of bearing risk for specialist-driven costs without having real influence over specialist decision-making or access to timely data about specialist activities.
ACO LEAD introduces CMS administered risk arrangements (CARA), a mechanism specifically designed to enable specialists to participate in shared risk arrangements without requiring primary care ACOs to manage complex contracting relationships. Under CARA, CMS administers the arrangement on standardized terms, and specialists can share in savings from specific episodes they help manage. This is not semantic complexity but genuine operational simplification that removes a significant barrier to specialist engagement.
As a concrete example, CMS has designed a falls prevention episode as part of the CARA framework. This reflects evidence that falls are the leading cause of both fatal and nonfatal injuries among adults aged 65 and older[6], with approximately 1 million fall-related hospitalizations and more than 38,000 deaths in this population annually[7], and yet previous models made it difficult to coordinate systematic falls prevention across multiple providers. By creating a standardized episode structure, CMS enables ACOs to easily contract with physical therapy practices, geriatric assessment programs, and home modification services to deliver coordinated prevention.
Technology infrastructure: the foundation nobody mentions during announcements
The most striking aspect of ACO LEAD, from an operational perspective, receives minimal discussion in CMS announcements but proves absolutely essential to success: the model is explicitly designed to function with integrated data, real-time analytics, and intelligent workflow support. This is not optional infrastructure or nice-to-have functionality. It is foundational to the model’s design.
CMS’s own design documentation for ACO LEAD explicitly acknowledges that previous models created the right incentive structure but failed to deliver timely data to providers to enable proactive intervention – a fundamental design limitation the agency committed to address in LEAD’s technical architecture. This acknowledgment signals that ACO LEAD assumes participating organizations will have the technological capabilities to see patients approaching risk thresholds, identify care gaps in real time, and execute coordinated interventions before costs accumulate.
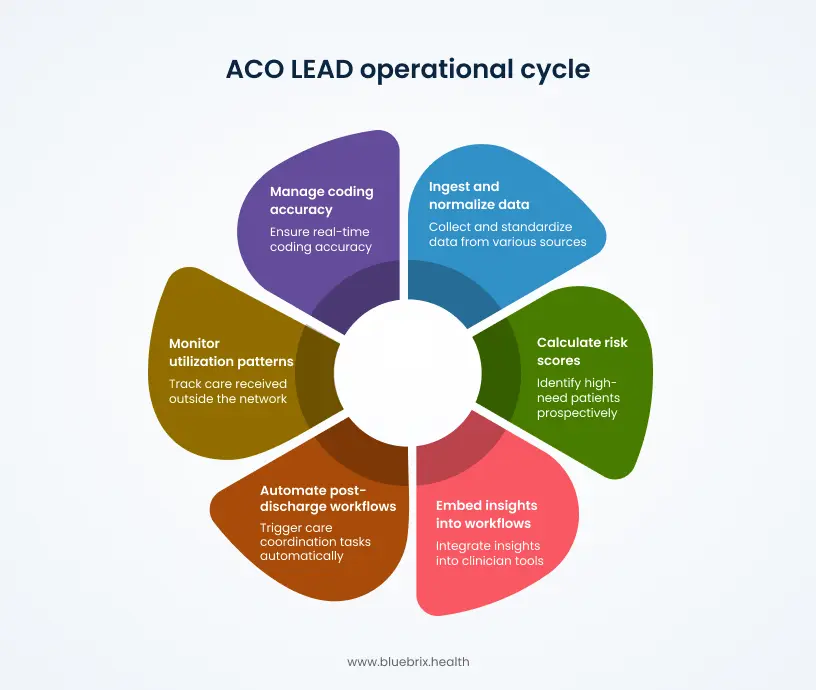
It means ACOs must be able to:
- Ingest and normalize data from multiple sources (claims, clinical records, pharmacy, lab, social determinants) into a unified patient view accessible to care teams
- Calculate risk scores and identify high-need patients prospectively, not retrospectively after costs have already been incurred
- Embed insights directly into clinician workflows so that risk information, care gaps, and recent utilization appear where physicians actually work, in their EMR or daily schedule, rather than forcing them to navigate separate portals
- Automate post-discharge workflows and event triggering, so that when a patient is hospitalized, care coordination tasks automatically generate for the care team
- Monitor utilization patterns and “leakage“ (care received outside the ACO’s preferred network) to maintain the connection between invested resources and financial performance
- Manage coding accuracy and risk stratification in a continuous, real-time manner rather than handling it as a year-end cleanup process
The capacity to do these things is not a competitive advantage in ACO LEAD but a baseline requirement. Practices that attempt to operate this model using legacy systems, manual processes, or point-solution tools bolted onto fee-for-service infrastructure will find themselves structurally disadvantaged.
This is where care coordination orchestration platforms become essential. Organizations like blueBriX specialize in exactly this infrastructure challenge: creating a unified ecosystem where clinical data, claims information, and patient-centric analytics inform care coordination in real time, without requiring providers to operate across fragmented systems. The operational pressure of ACO LEAD where monthly prospective payments create immediate accountability for performance and where data quality directly impacts financial results makes integrated technology not just valuable but necessary.
CEHRT requirements and transition pathways
One participation requirement not prominently discussed in most LEAD coverage: all participating organizations must use Certified Electronic Health Record Technology (CEHRT). Recognizing that smaller and independent providers may face implementation complexity, the RFA includes two flexibility provisions:
- A one-year transitional CEHRT pathway for ACOs and individual clinicians for whom 100% compliance is operationally complex in the first performance year
- A three-year CEHRT deferral pathway for providers utilizing advanced custom health IT implementations that require additional time to meet certification requirements.
Organizations should confirm their EHR’s current certification status and engage their vendor on the applicable pathway before finalizing participation plans. This is particularly relevant for rural practices, FQHCs, and behavioral health organizations that may operate on non-certified or partially certified platforms.
CMS is also launching a Tech Enabler program within LEAD specifically to assist ACOs – particularly smaller ones – in adopting high-value digital health tools and data-sharing capabilities. Details on scope and funding will be published in CMS technical materials.
The quality reporting evolution
ACO LEAD includes modifications to quality reporting requirements that aim to reduce administrative burden while maintaining meaningful performance measurement. The model creates focused accountability around a defined set of quality measures while allowing practices flexibility in how they achieve those targets.
Unlike models where quality reporting feels disconnected from daily clinical work, ACO LEAD is designed to integrate quality measurement into routine documentation and care delivery. This means that the clinical decisions providers make every day whether to screen for depression, manage blood pressure targets, or ensure medication reconciliation automatically generate the data needed for quality reporting rather than requiring separate, retrospective data abstraction.
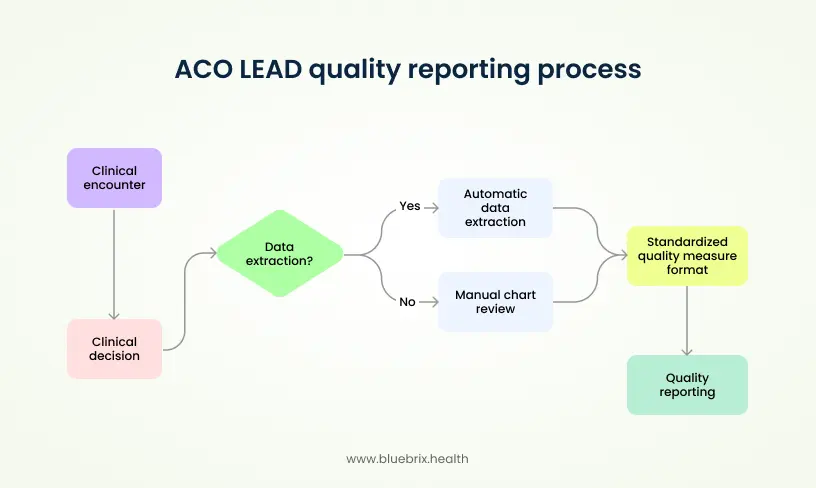
This integration depends entirely on having clinical systems capable of extracting data automatically from clinical encounters and translating it into standardized quality measure formats. The alternative manual chart review and administrative abstraction is both expensive and error-prone.
Beneficiary engagement and patient experience
While ACO LEAD fundamentally restructures the financial incentives and operational requirements for providers, it simultaneously creates new tools to engage beneficiaries themselves. Starting with the model’s launch, beneficiaries can enjoy enhanced cost-sharing benefits, including reductions in copayments for outpatient services. By 2029, the model will expand to allow beneficiaries to “buy down” their Medicare prescription drug premiums using savings generated by the ACO.
This direct link between ACO financial performance and beneficiary benefit improvements is intentional. It acknowledges that accountable care only succeeds when patients understand why they should engage with coordinated care and when they have tangible reasons to do so. A patient whose copay is reduced or whose medications cost less has a direct incentive to use the ACO’s preferred providers and to engage in preventive care rather than waiting for acute problems.
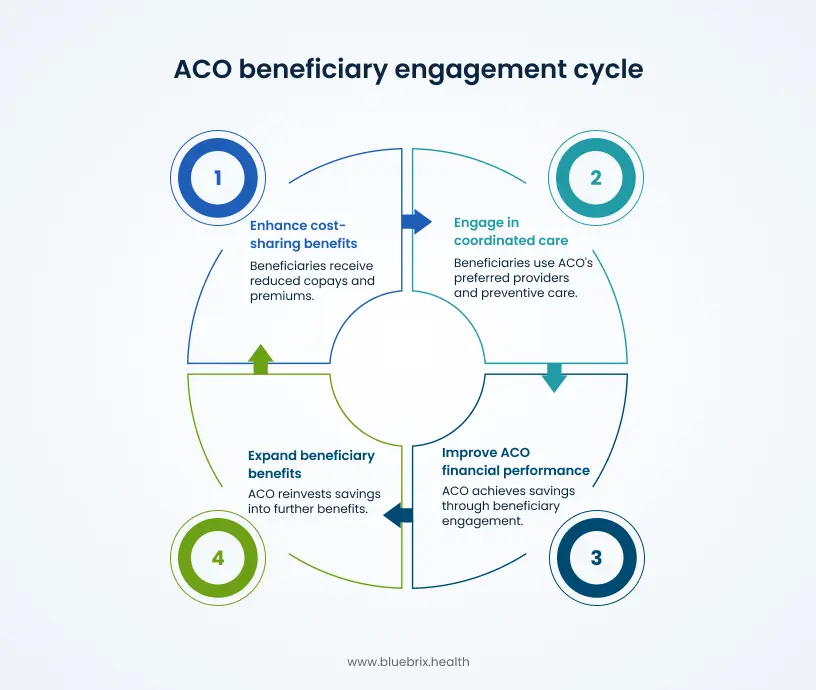
From a care coordination perspective, this also creates additional tools for outreach and engagement. Care teams can communicate clearly to patients: “By staying engaged in our care coordination program and using our network, you save money on your premiums and copays.” This value proposition is far simpler and more motivating than abstract discussions of “better outcomes.”
The geographic expansion opportunity
ACO LEAD explicitly targets geographic expansion and the participation of previously underserved markets. CMS has committed to actively recruiting rural practices, small independent practices, and practices caring for specialized or complex patient populations. For regions that have historically been overlooked in value-based care adoption, particularly rural areas, underserved urban markets, and practices focused on behavioral health, LEAD creates a genuine opportunity.
The minimum patient panel requirements are substantially lower for new entrants, the financial benchmarks include special adjustments for new ACOs, and the infrastructure investment support targets exactly the organizations most likely to lack capital for technology and hiring. If you practice in an area where value-based care has felt irrelevant or inaccessible, ACO LEAD may represent the first genuinely viable pathway to participation.
Timeline and transition planning
The CMS Request for Applications for ACO LEAD Performance Year 2027 was released March 31, 2026, with applications due May 17, 2026. CMS is reviewing submissions and will notify accepted applicants by mid-2026. For accepted REACH participants, ACO REACH ends December 31, 2026 – LEAD begins the following day with no gap in participation. Organizations that did not apply for the first cohort can submit a Letter of Interest (LOI) at the CMS LEAD model page for consideration in future performance year cohorts; CMS has indicated it anticipates additional application windows beyond PY2027.
For organizations currently operating under MSSP or other CMS models, note that Participant TINs cannot simultaneously participate in LEAD and the Shared Savings Program, ACO PC Flex, or several other specified CMS models. The question is whether to transition to LEAD proactively or plan for a future cohort window.
The critical question is no longer whether to participate in value-based care – it is whether your organization has the operational infrastructure to succeed when Performance Year 1 begins on January 1, 2027, or when a future cohort application becomes available. The difference between those two scenarios is preparation depth, not direction.
The implementation period: your structured on-ramp to January 2027
All applicants accepted under the PY2027 RFA will have the opportunity – but not the obligation – to participate in an optional Implementation Period from September 15, 2026 through December 31, 2026, with no financial risk. During this period, accepted participants can:
- Establish their provider network at the TIN-NPI level
- Conduct voluntary alignment activities to build their attributed beneficiary base before Performance Year 1
- Configure care coordination workflows, risk stratification logic, and automated care gap tools
- Complete staff training and pilot clinical protocols
Beneficiaries are not formally aligned to the ACO during the Implementation Period – alignment begins January 1, 2027. ACOs wishing to carry voluntary alignment from ACO REACH into LEAD are required to participate in the Implementation Period. Accepted participants must sign an Implementation Period Participation Agreement (IPPA); signing does not obligate participation in Performance Year 1.
For accepted organizations, this window is the single most important operational preparation period available before financial accountability begins.
Why ACO LEAD matters now
The announcement of ACO LEAD represents CMS’s most explicit acknowledgment to date that previous value-based care models created unnecessary barriers, particularly for independent and small practices. The 10-year benchmark stability, the enhanced financial support for rural providers, the simplified specialist contracting, and the prospective payment structure are structural changes designed to make accountable care sustainable for a broader range of organizations.
For providers who have watched value-based care become increasingly dominated by large hospital systems, ACO LEAD offers a genuine alternative pathway. For practices that have attempted ACO participation and found it operationally overwhelming, the simplified framework and technology assumptions may make a second attempt worthwhile.
However, success in ACO LEAD requires honest assessment of your current capabilities. Most critically, it requires technology infrastructure robust enough to deliver real-time insights to care teams, integrate data across multiple sources, and support the workflows that actually drive coordinated care. Organizations that attempt to operate ACO LEAD with fragmented, legacy systems will find themselves unable to translate the model’s financial incentives into actual performance improvement.
For organizations accepted into the first cohort, “now” means the pre-implementation period – the September 15 to December 31, 2026 window to establish provider networks, configure care coordination workflows, and complete staff readiness before financial accountability begins January 1, 2027. For organizations that did not apply for PY2027, “now” means beginning the technology and operational assessments that will make a future cohort application competitive.
The underlying argument is the same for both groups: success in ACO LEAD requires technology infrastructure that delivers real-time insights, integrates data across multiple sources, and supports the workflows that actually drive coordinated care. Whether your go-live is January 2027 or a subsequent year, the infrastructure requirements do not change.
The clock is ticking. Let’s have a conversation about where your practice stands and what readiness actually looks like.
Preparation and due diligence: essential steps for 2026
| Accepted PY2027 participants Sep 15 – Dec 31, 2026 | Future cohort candidates Ongoing |
|---|---|
| Finalize provider network at TIN-NPI level | Submit Letter of Interest to CMS |
| Configure care coordination workflows and risk stratification | Assess patient population risk profile and comorbidity burden |
| Complete staff training on protocols and coding accuracy | Evaluate EHR certification status against CEHRT requirements |
| Conduct beneficiary outreach for voluntary alignment | Identify network gaps and missing service lines |
| Sign Participation Agreement with CMS | Begin financial modeling under both risk tracks |
As of June 2026, ACO LEAD Performance Year 2027 applications have closed and CMS is reviewing submissions. Accepted organizations are preparing for the optional September 15–December 31, 2026 Implementation Period before the January 1, 2027 go-live. For organizations that did not apply for the first cohort, CMS has indicated it anticipates additional application windows for future performance years – submitting a Letter of Interest at the CMS LEAD model page is the recommended next step.
The preparation guidance below applies to both groups: accepted participants should use the Implementation Period to complete these foundational steps; future cohort candidates should treat this as the readiness framework that will determine whether their application is competitive when the next window opens.
For accepted PY2027 participants – Implementation Period priorities (September–December 2026):
- Finalize your provider network at the TIN-NPI level and complete voluntary alignment activities before January 1, 2027
- Configure care coordination workflows, risk stratification logic, and automated care gap tools in your technology platform
- Complete staff training on care coordination protocols, coding accuracy, and network management
- Conduct beneficiary outreach to drive voluntary alignment before Performance Year 1 begins
- Sign your Performance Year Participation Agreement with CMS
For future cohort candidates – ongoing readiness work:
- Submit a Letter of Interest at https://www.cms.gov/priorities/innovation/innovation-models/lead to remain informed of future application rounds
- Assess your patient population’s risk profile, complexity, and comorbidity burden – this directly informs benchmark modeling and risk-track selection
- Evaluate your current EHR’s certification status against CEHRT requirements and identify the applicable compliance pathway.
- Identify network gaps: where are patient care patterns fragmented and which critical service lines are missing?
- Begin financial modeling under both Global and Professional risk tracks using your actual patient population and cost baseline
- Build internal stakeholder alignment around a 10-year value-based care commitment – this is not a pilot