Choosing an EHR system is one of the most important decisions a healthcare practice will ever make. And yet it is often treated like buying a new piece of office software: a quick comparison of features, a pricing conversation, and a signature. That gap between how significant the decision is and how casually it sometimes gets made is where a lot of practices run into trouble.
The reality is that your EHR touches almost everything. It shapes how naturally clinicians can document a patient encounter, how smoothly your team hands off information, how accurately your claims go out the door, and how safely patient data moves between providers. It is not a back-office tool. It is the connective tissue of your entire practice.
Choosing the right EHR is not about finding the longest feature list or the best introductory price. It is about asking the right questions before committing to a platform that will shape how your practice runs for years to come.
Why your EHR choice matters more than you think?
If you’ve ever worked in a clinical setting, you already know that the tools you use every day can either make your job easier or make it miserable. The EHR system sitting at the center of your practice is no different. Get it right, and it quietly supports everything you do. Get it wrong, and you feel it in every single shift.
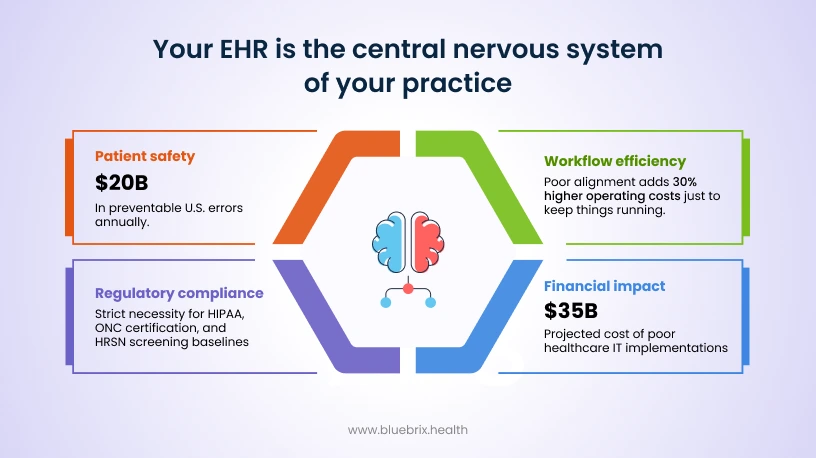
Patient Safety: Think about the last time a system flagged a drug interaction before it became a problem. That’s an EHR doing its job. The right system acts like a second set of eyes, catching medication errors, allergy conflicts, and dosing issues before they ever reach a patient. In the U.S. alone, these kinds of errors cost an estimated $20 billion a year, and a huge chunk of them are preventable.
But here’s the thing: a poorly designed system can actually make things worse. When clinicians are bombarded with constant alerts, nearly half of them get dismissed out of habit. That’s not a clinician problem, that’s a design problem. In behavioral health, a good EHR goes even further by tracking things like PHQ-9 scores over time, so care decisions are based on real data rather than memory or guesswork.
Workflow Efficiency: Nobody chose a career in healthcare to spend hours fighting with software. A well-suited EHR can cut documentation time by 30 to 50 percent, which means more time with patients and less time staring at a screen. It also means your care team can actually communicate across settings without chasing faxes or re-entering the same information twice.
When the system doesn’t fit the practice, the ripple effects are hard to ignore. Workflows slow down, integrations break, and some practices end up paying 30 percent more in operating costs just to keep things running. For behavioral health providers who are already managing heavy caseloads and emotional demands, a clunky system isn’t a minor frustration. It’s a real contributor to burnout.
Regulatory Compliance: Compliance isn’t the most exciting topic, but it matters more than most people realize until something goes wrong. HIPAA, HITECH, CMS requirements, ONC certification, these aren’t just boxes to check. They’re the framework that keeps patient data protected and your practice out of legal trouble.
A certified EHR handles a lot of this in the background through encryption, audit trails, and built-in reporting tools. It also positions your practice well for value-based care models, which are only becoming more important. For behavioral health practices involved in programs like HRSN screening, having a compliant system isn’t optional. It’s the baseline.
Financial Impact: A good EHR is genuinely one of the better investments a practice can make. Faster billing, fewer denied claims, and cleaner coding all add up over time. Poor implementations, on the other hand, are projected to cost U.S. healthcare around $35 billion, and that number comes from very real problems like staffing overruns, coding errors, and reimbursements that take far too long to arrive.
Some practices end up needing 62 percent more pharmacist hours just to clean up errors that a better system would have prevented in the first place. In behavioral health, the right EHR directly protects revenue by reducing the small but costly coding mistakes that quietly chip away at income month after month.
The trends shaping what vendors are building right now
A few things are clearly driving where the industry is headed, and they are worth paying attention to when you are evaluating what a vendor’s roadmap actually looks like.
- AI and automation have moved from buzzword to baseline expectation. Ambient voice scribes that listen and document during a clinical encounter are cutting documentation time by up to 50 percent. Predictive analytics are being used to flag everything from readmission risks to behavioral health relapses before they happen. And generative AI is starting to take on some of the coding burden for value-based reporting like MIPS.
- Cloud has essentially won. More than 90 percent of new EHR deployments are cloud-native, and consolidation across the market is rapidly merging older legacy systems into platforms built around FHIR-ready architecture. If a vendor is still primarily selling an on-premise solution in 2026, that is worth questioning.
- Interoperability is no longer optional. TEFCA and QHIN mandates are pushing FHIR R4 adoption across the industry, and health information exchanges are becoming a real part of how care coordination works in value-based models. Systems that cannot participate in that ecosystem are going to create problems.
- Patient-facing features have become a competitive differentiator. Practices using portals with remote monitoring, self-scheduling, and Cures Act compliant data transparency are seeing no-show rates drop by as much as 25 percent. Patients are expecting more, and the EHRs that help practices deliver it are pulling ahead.
What this means specifically for behavioral health?
Behavioral health EHRs are growing faster than the broader market, at around 9 percent annually. That reflects the very real surge in mental health demand that practices across the country are navigating. The specialty systems gaining the most traction are those built around 42 CFR Part 2 compliance, PHQ-9 and outcome tracking, and AI tools that can model therapy adherence and flag patients at risk of disengaging from care. Telehealth integration is essentially table stakes at this point.
How to choose the right EHR for your practice?
Picking the right EHR comes down to asking the right questions before you commit. There are a handful of criteria that separate a system that genuinely works for your practice from one that just looks good in a demo.
Does it actually fit how you work?
This is the starting point. A system built for a large clinical network is going to feel like a bad fit in a behavioral health clinic, and vice versa. Think about the specific things your practice needs every day: therapy notes, outcome tracking like PHQ-9 scores, role-based access for therapists and psychiatrists, scheduling, e-prescribing, lab integration, billing. If the EHR doesn’t handle those things smoothly, no amount of features elsewhere will make up for it.
Is it something your team will actually use?
Even the most powerful EHR is useless if your team dreads opening it. Look for interfaces that feel intuitive, templates that can be customized to your workflows, and AI-assisted documentation that cuts down on the repetitive stuff. Mobile access matters too, especially for providers who move between settings. Before you sign anything, run a demo. Better yet, get a trial period and put it in front of the people who will use it every day.
Can it talk to your other systems?
Care doesn’t happen in one place, and your EHR shouldn’t act like it does. Look for systems that support modern interoperability standards like FHIR and TEFCA, and check whether it connects comfortably with your labs, pharmacies, payers, and patient portal. Telehealth integration and MIPS reporting compatibility are worth verifying early too. Data silos slow everything down and create real risks for patients moving between providers.
Is it built to keep data safe?
In healthcare, and especially in behavioral health, data sensitivity is not something to treat lightly. Your EHR needs to be HIPAA compliant and ONC certified, with proper encryption, audit trails, and regular security reviews baked in. For behavioral health specifically, look for role-based access controls and support for multi-program compliance reporting like HRSN assessments.
What is it really going to cost?
The sticker price is rarely the whole story. Factor in implementation fees, ongoing subscriptions, training time, and what it will take to migrate your existing data. On the flip side, think about what a good revenue cycle management tool could recover in denied claims or billing errors. And as your practice grows, can the system grow with you? Review vendor contracts carefully and watch for anything that makes it difficult to leave if the relationship stops working.
Is it built for the cloud?
This one matters more than most people realize. Cloud-native EHRs are designed to scale up automatically when demand spikes, push updates without taking the system offline, and recover quickly from outages without someone manually intervening. For behavioral health practices, this is especially relevant when telehealth demand surges unexpectedly. Compared to older on-premise systems that require constant hardware maintenance and carry real vulnerability risks during migrations, cloud-native platforms can reduce IT overhead by 40 to 60 percent. When evaluating vendors, ask whether they run on certified infrastructure like AWS or Google Cloud, not just whether they are technically “cloud-based.”
Does it protect your revenue?
Billing in behavioral health is complicated, and a disconnected billing system is quietly costing practices more than they realize. Mental health claims see around 15 percent revenue loss from denials alone. The best EHRs have revenue cycle management built right in, with claim scrubbers that catch errors before submission, AI tools that predict which claims are likely to be denied, automated payment posting, and NLP that links clinical notes directly to billing codes. Look for dashboards that show you AR days and first-pass rates at a glance, so nothing slips through unnoticed.
Does it use AI in a way that actually helps?
AI is everywhere in EHR marketing right now, but not all of it is worth the hype. What you actually want is AI that does specific, useful things: flagging patients at risk of readmission, surfacing PHQ-9 trend alerts in real time, generating clinical notes that cut documentation time in half, and supporting value-based care contracts through cohort analytics. For behavioral health, outcome forecasting tools like therapy adherence models can be genuinely valuable. One important caveat though: avoid any system using AI that cannot explain its recommendations. ONC rules are moving in the direction of explainability, and black-box algorithms create both compliance and trust issues.
Does it help patients stay engaged in their own care?
Patients today expect more than a portal where they can download a PDF of their visit summary. They want to self-schedule, message their care team securely, join video visits, and in some cases submit remote monitoring data like depression screeners from their phone. Practices that meet patients where they are see no-show rates drop by as much as 25 percent. Under the Cures Act, patients also have stronger rights to access their own data, so transparency is no longer optional. In behavioral health, engagement tools take on even more weight: think crisis check-in features, family portal access, and integration with apps like Apple Health.
Can it grow with you?
A system that works well for 10 providers should still work well when you have 50. That sounds obvious, but a lot of EHRs hit a wall when practices expand, merge with other clinics, or onboard new service lines. Look for systems that use auto-provisioning and multi-tenant architecture, and ask vendors directly how they handle enterprise growth. Before you commit, push them on load testing. How does the system perform under pressure? Poor scalability does not just slow things down; it can strand your data at exactly the moment you need it most.
What does getting started actually look like?
Implementation is where a lot of EHR relationships go wrong, and it is worth being direct with vendors about your expectations upfront. A 90-day go-live timeline with proper data migration and validation above 99 percent accuracy is a reasonable standard to hold vendors to. Role-specific training matters too: a therapist and a billing coordinator need very different onboarding experiences. Once you are live, you need real support, meaning a team you can call at any hour, not just a help portal. Ask for their NPS score and look for anything above 70 as a baseline. Check their SLA for uptime guarantees and find out whether upgrades are included or come with an added cost. And before you sign, talk to at least three practices similar to yours who have been through their implementation process.
No single EHR is going to be perfect, but the right one for your practice is out there. The key is knowing what to look for before you start the search, not after you’ve already signed a three-year contract.
Beyond the demo: what to find out before you commit?
Evaluating an EHR on features and pricing is one thing. Figuring out whether the vendor behind it is actually going to show up for you is another. These are the things that do not show up on a feature comparison sheet but can make or break your experience after the contract is signed.
Watch what they do during the demo, not just what they show you
A polished demo tells you very little about what day-to-day support actually looks like. So, use the demo to run some real tests. Call their support line while you are in the room with them and see what happens. Ask them to build a therapy note template on the spot rather than showing you a pre-built one. Request a live FHIR R4 integration with a lab rather than a slideshow of how it works. Vendors with genuinely good systems will welcome this. Vendors with something to hide will stall, redirect, or suddenly discover that the demo environment does not support it.
Listen carefully to how they handle pushback
Pay attention to the language vendors use when you ask hard questions. Phrases like “portal tickets are sufficient for most issues,” “setup costs are to be determined,” or “one workflow fits all practices” are not just vague answers. They are previews of how the relationship will feel when something goes wrong. A vendor who cannot give you straight answers before you sign is unlikely to become more transparent afterward.
Know your 42 CFR Part 2 exposure
For behavioral health practices, this one deserves its own conversation. 42 CFR Part 2 governs how substance use disorder and sensitive behavioral health data can be shared, and not every EHR vendor understands it well enough to keep you protected. If a vendor cannot clearly explain how their system handles 42 CFR Part 2 compliant data sharing, including how it interacts with health information exchanges, that is a serious gap. The compliance consequences in this area are not abstract.
Build exit clauses into every contract
Before you sign anything, make sure you have a clear, contractually protected way out if the relationship stops working. Vendor lock-in is real, and some contracts are written specifically to make leaving painful and expensive. Ask for itemized pricing, a full three-year cost projection, and explicit terms around data portability if you ever need to migrate. A vendor who pushes back on exit clauses is telling you something important about how they view the relationship.
Do not settle for two references
Most vendors will offer you two or three references, and those calls are usually scripted. Ask for five, request that the conversations happen without a vendor representative present, and specifically seek out practices that are similar to yours in size and specialty and have been through the full implementation process, not just the sales cycle. Client churn above 20 percent is a meaningful warning sign worth asking about directly. The vendors who have nothing to hide will connect you without hesitation.
What sets blueBriX apart?
A lot of EHR vendors will check the same boxes on a feature list. What tends to separate a good long-term partner from a frustrating one is everything that sits around the product itself: how it is priced, how easy it is to make it your own, who built it and with whose input, and what happens when you need to leave. This is where blueBriX makes a different kind of case.
Designed with the people who actually use it
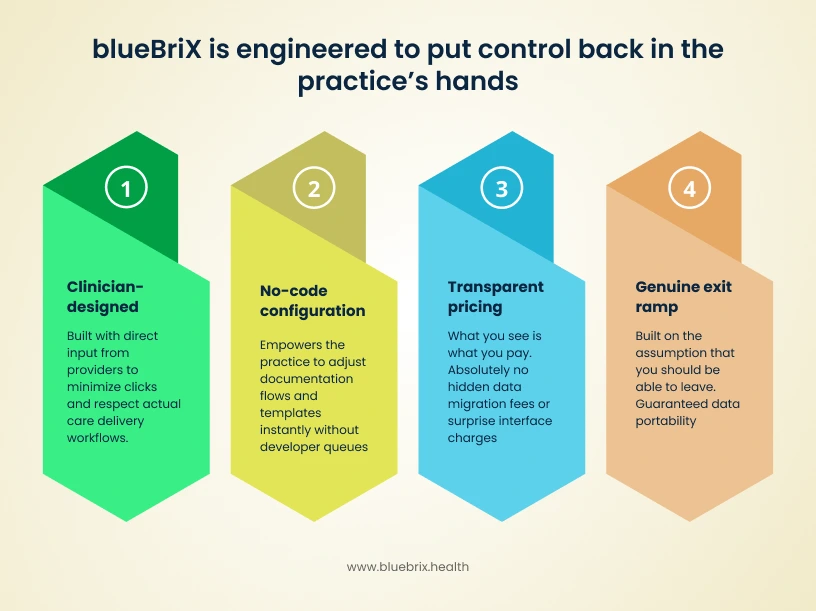
Most EHR interfaces were designed by engineers optimizing for data capture, not by clinicians optimizing for care delivery. blueBriX was built with direct clinician input from the start, and that shows up in the small things that add up over a day: fewer unnecessary clicks, faster charting, specialty-specific templates that reflect how real workflows actually run rather than how someone imagined they might. Mobile access means providers are not anchored to a workstation. The result is a system that people actually want to open rather than one they dread.
No-code configuration that puts control in your hands
Customizing a legacy EHR to fit your specialty typically means submitting a request, waiting weeks, and paying for developer time. blueBriX takes a fundamentally different approach by making workflow configuration something your own team can do without writing a single line of code. Whether you need to adjust documentation flows, create new templates, or adapt the system as your practice evolves, that control sits with you rather than with a vendor’s development queue.
Pricing that says what it means
Legacy EHR contracts are notorious for costs that only reveal themselves after you are already committed: migration fees, interface charges, per-location premiums, and upgrade costs that were never mentioned in the original conversation. blueBriX operates on transparent, predictable pricing where what you see is what you pay. There are no hidden fees for data migration or interface setup, and the contract is structured to keep you as a partner rather than lock you in as a captive account.
A genuine exit ramp if you ever need one
Most legacy vendors make leaving deliberately difficult, whether through proprietary data formats, punishing contract terms, or migration fees designed to make staying feel like the only realistic option. blueBriX builds the relationship on the assumption that you should be able to leave if it stops working, which paradoxically tends to make the partnership work better. Knowing your data is portable and your options are open changes the dynamic entirely.
Why 2026 is the year to get your EHR decision right?
There has never been a more consequential time to get your EHR decision right. The pressures bearing down on clinical practices in 2026 are not abstract or distant. They are showing up in reimbursement statements, staff resignation letters, and patient satisfaction scores right now. Legacy systems that were tolerable five years ago are actively creating risk today, and the window for making a comfortable transition is narrowing.
The regulatory environment has real teeth now
The 21st Century Cures Act is no longer just a policy framework. CMS and ONC are actively enforcing information blocking rules, with fines reaching up to $1 million per violation. MIPS bonuses are also on the line for practices whose systems cannot demonstrate compliant data sharing. For behavioral health practices navigating HRSN screening mandates, the reporting requirements are becoming more specific and more scrutinized. An EHR that cannot keep up with these requirements is not just an inconvenience. It is a financial liability.
TEFCA is live and practices without FHIR readiness are already behind
TEFCA’s QHIN networks are rolling out nationally, and participation requires FHIR R4 APIs. Practices whose EHRs are not TEFCA-ready are effectively cut off from the coordinated care networks that ACOs, CCOs, and value-based contracts increasingly depend on. This is not a future problem. It is happening now, and the practices that are not connected are already being sidelined in conversations about shared savings and population health contracts.
Fee-for-service is fading faster than most practices realize
More than 60 percent of Medicare lives are now in value-based care arrangements, and that number is only going in one direction. The problem with legacy EHRs in this environment is not just that they are slow. It is that they often cannot track the quality metrics that determine whether a practice earns shared savings or bundled payments. PHQ-9 trends, readmission risks, population health analytics: these are no longer nice features. They are the infrastructure of getting paid.
Clinician burnout is a workforce crisis and bad EHRs are making it worse
The physician shortage is real and growing. The AAMC projects a gap of 124,000 physicians by 2034, and burnout is one of the primary drivers of early exits from the profession. AMA research has found that EHR frustration triples the odds of burnout, and rigid, poorly designed systems are adding roughly two hours of unnecessary documentation to every clinical day. In behavioral health, where therapist shortages are already acute, a system that drives clinicians away is not just a productivity problem. It is an existential one.
Patients have moved on and outdated systems are struggling to keep up
According to ONC data, around 80 percent of patients now expect portal access, telehealth options, and mobile scheduling as standard parts of their care experience. Practices that cannot deliver these things are seeing it in their no-show rates, which run more than 25 percent higher when access is clunky or inconvenient. In behavioral health, where virtual check-ins and between-session touchpoints have become part of standard care, falling short on patient engagement tools is a direct threat to continuity of care.
The competitive gap is widening every quarter
Practices that have already modernized their EHR infrastructure are running 20 to 30 percent more efficiently in their revenue cycle and clinical workflows. Industry benchmarks put the annual cost of staying on a legacy system at over $500,000 per practice in revenue leakage and operational drag. That is not a one-time cost. It compounds. Every quarter spent on an outdated system is a quarter spent handing efficiency and market share to competitors who made the move earlier.