Every March, the Medicare Payment Advisory Commission (MedPAC) sends Congress a report that quietly shapes the financial future of every healthcare provider in America. It doesn’t make headlines the way a budget vote does. But its recommendations on who gets paid more, who gets paid less, and what behaviors the payment system will reward tend to become policy. And the 2026 edition carries some of the most consequential signals in years.
Why this report should be on every leader's desk
This isn’t just a document for hospital administrators or Washington insiders. Whether you run a behavioral health clinic, lead an RCM team, manage a care coordination program, or are building a value-based care strategy, the MedPAC March 2026 report tells you something important about the environment you’ll be operating in by 2027 and beyond. You may need to check if your EHR software supports these recommendations.
Here’s what the 671-page report actually means for you, broken down by the issues that matter most.
- $1.1 Medicare spend in 2024 — up 8% year-over-year
- 18% Share of U.S. GDP consumed by healthcare spending in 2024
- 50% Annual nursing home staff turnover — directly linked to quality scores
- 2× Projected Medicare spend by mid-2030s (nominal)
The 2027 payment landscape: winners, losers, and what it takes to stay on the right side
MedPAC’s headline recommendations for 2027 follow a clear logic: providers with demonstrably efficient operations and positive quality indicators get protected or rewarded; those where margins are deemed excessive relative to Medicare’s contribution face cuts. Here’s how it breaks down:
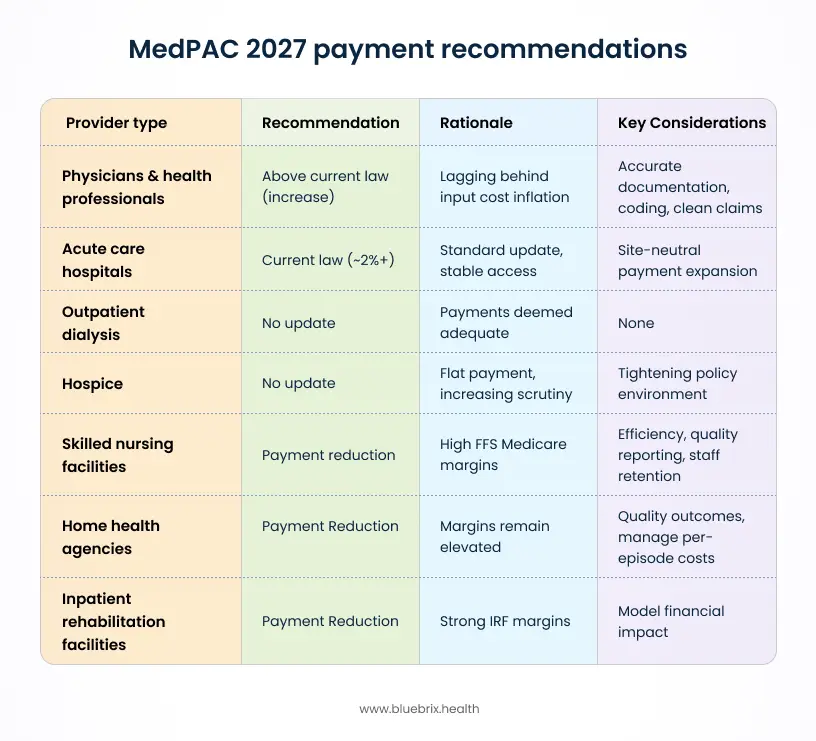
Physicians & health professionals — above current law (increase)
MedPAC recommends a payment update above what current law would provide. Physician payment rates have consistently lagged behind input cost inflation, and this recommendation acknowledges that gap. However, providers only capture the full value of this increase when their documentation accurately reflects patient complexity, comorbidities are coded correctly, and claims submit cleanly. Does your current EHR support detailed documentation and suggest the right codes for billing? Organizations with coding gaps or high denial rates will see the rate increase partially eroded before it reaches their revenue.
Acute care hospitals — current law (~2%+)
Hospitals receive the standard update reflected in current law with no additional uplift and no reduction. Access indicators remain stable, hospital occupancy is within normal range, and all-payer margins have improved. That said, MedPAC’s continued push for site-neutral payment expansion means hospital outpatient revenue could still face pressure even with a flat base rate update. Finance teams at hospital-affiliated organizations should model that exposure separately.
Outpatient dialysis — no update
Payments are deemed adequate as-is. Dialysis provider margins remain at a level MedPAC considers sufficient to support efficient care delivery, so no payment update in either direction is recommended for 2027.
Hospice — no update
Flat payment with increasing scrutiny. Quality concerns, particularly around very long stays close to end of life, are noted in the report. No uplift is recommended, and the policy environment around hospice utilization patterns is likely to tighten over the coming years.
Skilled nursing facilities — payment reduction
MedPAC judges that FFS Medicare margins for SNFs remain high enough to warrant a cut. For SNF operators, this means the margin buffer many have relied on is narrowing. Efficiency, quality reporting accuracy, and staff retention which directly affects quality star ratings become critical levers for protecting revenue in this environment.
Home health agencies — payment reduction
The Patient-Driven Groupings Model (PDGM) introduced in 2020 already reduced visits per episode, but margins have remained elevated. MedPAC’s position is that payments exceed what is needed to support efficient care delivery. Home health providers will need to demonstrate quality outcomes and manage per-episode costs more tightly as payment pressure increases.
Inpatient rehabilitation facilities — payment reduction
IRF margins relative to Medicare costs are strong enough that MedPAC recommends a reduction. Congress has historically aligned with MedPAC on post-acute payment recommendations, so IRF operators should treat this as a likely outcome rather than a distant possibility and begin modeling the financial impact now.
For post-acute and home health providers
MedPAC’s payment reduction recommendations for SNFs, home health, and IRFs don’t automatically become law, but they have a strong track record of influencing Congressional action. If you operate in these spaces, now is the time to model the revenue impact and accelerate your RCM and quality reporting capabilities.
What behavioral health providers need to hear
The MedPAC report doesn’t call out behavioral health by name but it shapes the environment BH providers operate in at every level. Several of its findings land directly on the issues BH organizations are already wrestling with.
The VBC migration is accelerating
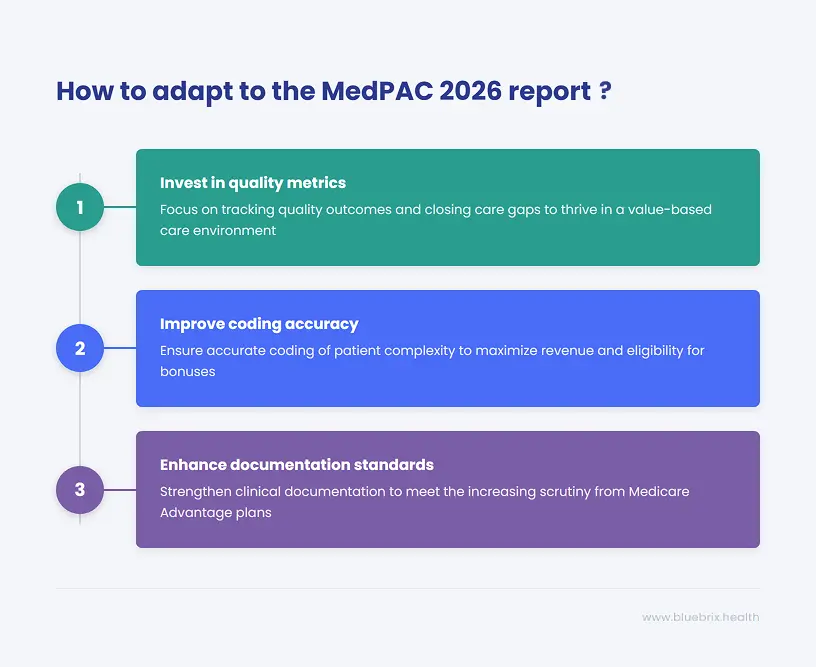
MedPAC’s consistent recommendation across provider types is a push toward value-based care: alternative payment models, quality-linked reimbursement, and away from pure fee-for-service volume. For CCBHCs and CMHCs, VBC has been part of your compliance landscape for years. But the report signals that this trajectory is hardening. Federal policy is moving toward a world where quality outcomes, not claim volume, determine revenue. Organizations that have invested in a purpose-built behavioral health EHR with quality metrics tracking, care gap closure, and SDOH documentation are building assets. Those still managing these processes manually in spreadsheets are accumulating risk.
Physician payment update
The above-current-law update recommended for physicians and health professionals is genuinely good news for behavioral health clinicians. But there’s a catch that the report makes clear through its broader analysis: providers who undercode patient complexity (failing to capture comorbidities like depression alongside primary diagnoses) systematically leave money on the table. HCC (Hierarchical Condition Category) coding accuracy directly affects risk scores, shared savings eligibility, and quality bonuses. This isn’t a billing technicality; it’s a strategic revenue issue that grows in importance as VBC spreads.
Medicare advantage scrutiny is intensifying
Nearly half of all Medicare beneficiaries are now enrolled in MA plans and a growing share of behavioral health patients are MA members. The report dedicates extensive analysis to the fact that MA plans are overpaid due to coding intensity and favorable selection. CMS is expected to respond with tighter coding scrutiny and risk-score audits. For BH providers operating in MA contracts, this means documentation standards are going up, not down. Accurate, complete, audit-ready clinical documentation isn’t optional anymore.
The BH workforce signal
MedPAC’s workforce chapter projects national shortages of RNs and LPNs, with nursing home staff turnover running at ~50% annually. For behavioral health, which already faces severe clinician shortages, this compounds the documentation burden on remaining staff. Every hour a clinician spends on manual billing, prior authorizations, or compliance paperwork is an hour not spent with patients. You need a care coordination solution or EHR with administrative automation. That’s a workforce retention strategy.
The RCM perspective: billing accuracy becomes crucial
Revenue cycle management teams often operate at one remove from federal policy discussions. But MedPAC’s 2026 report has direct implications for how RCM functions need to evolve over the next 12–18 months.
Site-neutral payments: a growing revenue risk for hospital-based billing
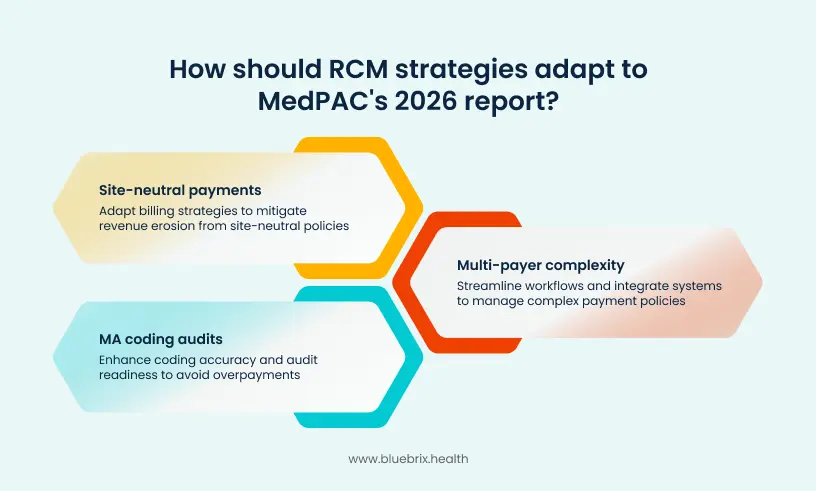
MedPAC is pushing hard for site-neutral payment policies, aligning Medicare rates for the same services regardless of whether they’re delivered in a hospital outpatient department, an ambulatory surgical center, or a physician’s office. In 2024, existing site-neutral policies reduced payments by $1.2 billion. CMS expanded these policies in 2026 for an additional $290 million in reductions, and MedPAC is recommending further expansion. For RCM teams at hospital-affiliated behavioral health departments or integrated health systems, this is an active revenue erosion risk that requires billing strategy adaptation, not just awareness.
MA coding audits are coming
The report’s detailed analysis of MA coding intensity — including technical appendices on how to measure and address overpayment — is a preview of the policy direction. As CMS tightens MA coding standards, payer audit frequency and intensity will increase. RCM teams need to move from reactive denial management to proactive coding accuracy and audit readiness. That means systematic pre-submission claim scrubbing, real-time eligibility verification across MA payers, and documentation standards robust enough to withstand retrospective review.
The multi-payer complexity problem gets harder
One of the report’s less-discussed but consequential findings is how Medicare’s payment policy decisions ripple through the broader payer landscape. Medicare rates are widely used as benchmarks by Medicaid programs and private insurers. As Medicare tightens certain payment categories and expands quality requirements, expect commercial payers to follow. RCM teams managing multi-payer environments — which is nearly every BH organization — will face an increasingly complex and rule-laden claims environment. Manual workflows and siloed billing systems will struggle to keep pace.
Care coordination: from clinical program to financial linchpin
The MedPAC report reinforces a shift that has been building for several years: care coordination is directly tied to financial performance in Medicare’s evolving payment models.
Post-acute care efficiency is under the microscope
MedPAC’s chapter on post-acute care highlights what it calls “high FFS Medicare payments, FFS incentives, and Medicare benefits” that may be encouraging inefficient care — including overuse of SNF and home health services when less intensive settings could achieve equivalent outcomes. This is a signal that care coordinators in transitional care roles will face increasing payer scrutiny around discharge disposition decisions and post-acute utilization patterns. An integrated EHR software that supports documenting the clinical rationale for care setting choices will matter more in audit and appeals contexts.
Alternative payment models reward coordination done right
The report explicitly notes that alternative payment models — ACOs, bundled payments, shared savings arrangements — create strong incentives to reduce post-acute care utilization through better coordination. For care teams managing high-risk populations across settings, this translates to a concrete financial case for investments in risk stratification, care gap tracking, and real-time patient status visibility. The organizations that can demonstrate reduced avoidable readmissions and post-acute utilization will capture meaningful shared savings.
Dual-eligible patients is a coordination complexity that pays
MedPAC’s mandated chapter on Dual-Eligible Special-Needs Plans (D-SNPs) is particularly relevant for care coordinators. Nearly half of dually eligible Medicare/Medicaid beneficiaries are now enrolled in D-SNPs, and the report notes that available data “provide limited insight” into relative performance. This is both a challenge and an opportunity: organizations with strong coordination infrastructure and measurable outcomes data are positioned to differentiate in a market where most players can’t demonstrate their value clearly.
SDOH documentation goes from nice-to-have to revenue driver
As VBC models and quality metrics tighten, Social Determinants of Health (SDOH) documentation is becoming directly tied to risk scores and quality bonuses. The care coordinator who tracks whether a patient actually accessed the food pantry referral and closes the loop in an EHR that’s purpose-built for VBC, is now contributing to HCC coding accuracy and quality measure performance. Closed-loop SDOH tracking isn’t just good clinical practice. It’s becoming a financial function.
Value-based care: the report as a strategic roadmap
For VBC executives and program leaders, the MedPAC 2026 report reads less like a policy document and more like a strategic roadmap. The trajectory it describes — away from FFS volume, toward quality-linked payments, integrated care models, and fiscal accountability — is one that VBC leaders have been navigating for years. But several specific findings are worth translating into strategy.
The Medicare safety-net index: a new targeting framework
MedPAC’s recommendation to replace the existing Disproportionate Share Hospital (DSH) metric with a new Medicare Safety-Net Index (MSNI) is a significant technical change with real strategic implications. The MSNI would better target resources toward hospitals that serve high proportions of low-income Medicare beneficiaries. For VBC leaders at safety-net organizations, this is a potential revenue enhancement — but capturing it requires the population health data and low-income patient tracking that most organizations still manage inconsistently.
Quality metrics are hardening across every setting
Across every provider type analyzed in the report, MedPAC’s payment-adequacy framework increasingly depends on quality performance — readmission rates, ambulatory care-sensitive hospitalizations, patient experience scores, and outcomes measures. For VBC leaders, the strategic implication is clear: quality data infrastructure is a financial asset. Organizations that can pull real-time quality metrics across their patient population, identify gaps before the payer does, and demonstrate performance improvement trajectories will have stronger VBC contract negotiation positions and better audit outcomes.
The fiscal pressure is permanent, build for it
Perhaps the most important strategic signal in the report is structural. Medicare spending is growing faster than the economy, faster than tax revenues, and faster than beneficiaries can absorb through premiums and cost sharing. This isn’t a short-term cycle — it’s a structural imbalance that ensures continued policy pressure on payment rates, quality requirements, and care efficiency standards for the foreseeable future. VBC models are the policy response to this imbalance. Organizations that build for a VBC environment aren’t just chasing a trend — they’re adapting to the permanent direction of Medicare policy.
What this means by role
- BH Clinical Leader – Prioritize HCC coding accuracy for comorbidities, invest in SDOH closed-loop tracking, and prepare documentation for tighter MA coding scrutiny.
- RCM / Finance Lead – Model site-neutral payment risk, build proactive MA audit readiness, and automate multi-payer eligibility and prior-auth workflows before complexity increases further.
- Care Coordinator – Document SDOH interventions and care setting rationale meticulously. Your coordination data is becoming directly tied to quality scores and shared savings calculations.
- VBC / Strategy Executive – Use the fiscal trajectory in this report as a board-level case for VBC investment. The payment environment described here is permanent, not cyclical.
- Compliance Officer – Prepare for intensified MA coding audits and new site-neutral billing requirements. Audit-ready documentation infrastructure is a priority now, not a future project.
- Post-Acute Operator – Payment reductions for SNFs, home health, and IRFs are recommended. Accelerate margin protection strategies through quality reporting, staff retention, and efficient care coordination.
How blueBriX helps you navigate this environment
The payment shifts described in the MedPAC report don’t require you to predict the future — they require you to build the operational infrastructure that performs well across a range of policy outcomes. At blueBriX, our platform is purpose-built for exactly this environment: where quality metrics determine revenue, where multi-payer complexity is constant, and where administrative inefficiency is an existential threat to already-thin margins.
- VBC analytics & quality tracking— Real-time dashboards for HEDIS, STARS, and payer-specific quality measures. Know your gaps before your payer does.
- HCC coding support— Automated prompts and documentation workflows that capture patient complexity accurately, reducing missed coding and improving risk scores.
- Automated RCM & claims optimization— ERA/X12 processing, real-time eligibility checks, and multi-payer rules automation across Medicaid, Medicare, and MA plans.
- Care coordination workflows— Closed-loop referral management, SDOH tracking, and risk stratification tools that turn coordination into measurable quality performance.
- Compliance-ready documentation— Pre-built templates for CCBHC, Medicaid, and MA audit requirements, reducing audit risk and accelerating month-end close.
- HL7/FHIR interoperability— Open API integration with HIEs, PDMPs, and payer systems — essential as MA plan data exchange requirements tighten.
- Telehealth & virtual care— HIPAA-compliant, built-in telehealth with integrated documentation and billing supporting access while reducing per-visit administrative cost.
- Workforce automation— Automated scheduling, prior auth workflows, and SMS/email patient engagement protecting your clinical staff time as workforce shortages intensify.
Conclusion: the prepared organization wins
The MedPAC March 2026 report is, at its core, a description of a system under financial pressure finding ways to pay for quality rather than volume. For providers across behavioral health, post-acute care, RCM, care coordination, and value-based programs, the message is consistent: the organizations that invest in the infrastructure to demonstrate quality, document complexity accurately, and operate efficiently will capture the upside of payment policy shifts. Those that don’t will find the cuts land harder and the bonuses remain out of reach.
This is a reason for preparation. The payment environment described in this report is the continuation of a trajectory that has been building for a decade. MedPAC 2026 accelerates the urgency for organizations that have been delaying investment in VBC readiness, RCM modernization, and care coordination infrastructure.
The question is whether your platform, your workflows, and your data will be ready when 2027 arrives.