For the past two years, the Medicare Advantage had a cushion. CMS’s transition to the V28 risk adjustment model was phased in gradually, a blend of old and new designed to soften the financial impact while plans adjusted. That cushion is gone.
As of January 1, 2026, MA plans are operating under 100% V28. No blend. No buffer. The 2,000+ diagnosis codes that were deleted or downweighed, including widely used depression, vascular, and metabolic codes, are officially off the books. Whatever revenue assumptions were built around them, don’t hold anymore.
This is where it gets uncomfortable for a significant number of plans: if your risk adjustment strategy leaned heavily on retrospective coding, chart reviews, end-of-year coding sprints, vendor-driven HCC recapture, you’re likely staring at a 3 to 8% revenue cliff right now. Not because your teams did anything wrong. But because the codes you spent years chasing are codes CMS no longer values.
The model has moved. And in 2026, if the documentation isn’t specific, the payment isn’t coming.
This article unpacks why the old playbook is losing ground, what the plans holding their footing are doing differently, and what it actually takes to operate in a 100% V28 world.
Why is the 'capture model' rupturing?
The old model had a simple internal logic: more codes meant more revenue. Diagnosis capture became a production line. Find the code, document the code, and submit the code. The patient behind the code was often secondary to the process built around it.
That logic worked when CMS’s model rewarded volume. It doesn’t work when CMS’s model rewards specificity and clinical validity. The disconnect was always there. In 2026, it’s just expensive.
And “expensive” is putting it mildly.
Most plans understood that unsupported diagnoses carried some level of risk. A failed (Risk Adjustment Data Validation) RADV audit meant paying back money on the records that didn’t hold up. Manageable. Contained. Something the compliance team handled.
That math changed when CMS reinstated audit extrapolation. Under current RADV rules, CMS audits a sample of your member records, typically around 200 patients per contract. If they find errors in that sample, they no longer limit the clawback to just those records. They extrapolate the error rate across your entire membership.
The numbers get uncomfortable fast. A documentation gap in a 200-patient sample that looks like a minor compliance issue can translate into a $50 million-plus clawback at the contract level. One unverified code isn’t a miss anymore. It’s a liability with a multiplier attached to it.
This is the structural problem with the capture model that no amount of coding sprints can fix. It was built to maximize, not to verify. In a world where every unsubstantiated code carries extrapolated financial risk, the model doesn’t just underperform. It actively works against the plan.
The regulatory ground beneath MA plans just moved
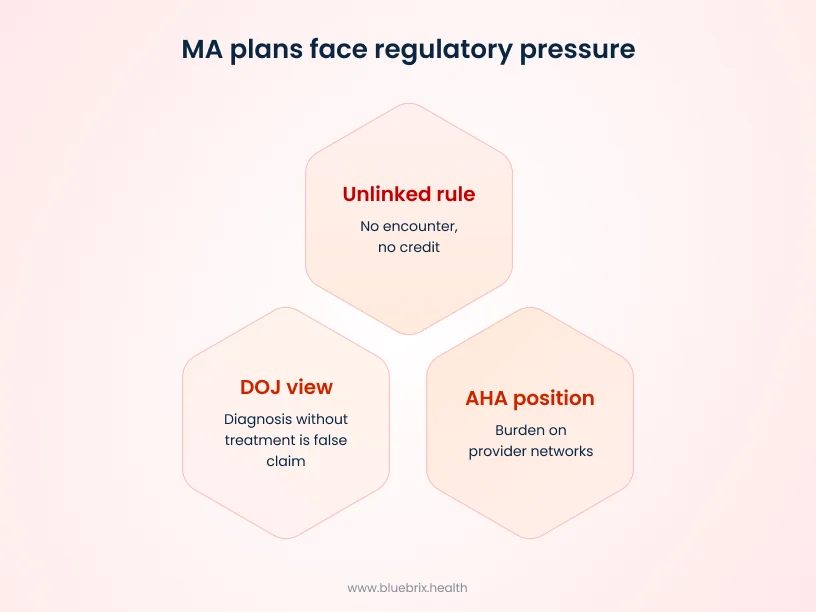
If the V28 revenue impact felt like a financial problem, what’s coming from the regulatory side makes it a legal one. The pressure on the capture model isn’t just coming from CMS’s payment formula. It’s coming from three directions simultaneously, and the timeline is tightening.
The 2027 “unlinked” rule
In the CY 2027 Advance Notice published January 26, 2026, CMS proposed something that should be getting more attention than it is. Any diagnosis code that isn’t tied to a specific, documented medical encounter, an actual doctor’s visit, won’t count for payment. No encounter, no credit. This isn’t a tweak. CMS projects the financial impact of this proposal at $7.1 billion industry-wide. That number is a signal, not a side note. CMS is explicitly drawing a line between finding codes and delivering care, and it’s pricing the difference.
The DOJ’s view on HRAs
Following the July 2025 National Health Care Fraud Takedown, the Department of Justice has been actively pursuing plans where Home Risk Assessments identified high-value diagnoses but the member never received any follow-up care. The DOJ’s position is straightforward and worth sitting with: a diagnosis without treatment isn’t a clinical finding. It’s a false Claim. Plans that used HRAs primarily as coding tools rather than care entry points are now finding themselves in the middle of that argument.
The AHA’s position
The American Hospital Association has been increasingly vocal about the administrative burden that MA plans place on provider networks, chart audits, retroactive documentation requests, and prior authorization friction. For MA plans, this matters beyond the policy debate. Providers have options. If your relationship with your network looks more like an auditor than a care partner, retention becomes a real operational risk. The plans that are building durable provider relationships in this environment are the ones showing up with data that helps providers, not requests that burden them.
Taken together, these three forces aren’t moving on separate tracks. They’re converging on the same conclusion: a business model built around capturing diagnoses without anchoring them in real care delivery has run out of runway, financially, legally, and operationally.
So what does the model that survives this environment actually look like? The MA plans holding their ground in 2026 have internalized something that sounds simple but operationally requires rewiring almost everything: a diagnosis is not the finish line. It’s the starting gun.
The pivot: 'better care' as survival
The plans that are winning in this environment aren’t just coding differently. They’ve restructured what success looks like operationally, shifting their performance measures, their care workflows, and their technology investments around one core principle: the value is in what happens after the diagnosis, not in the diagnosis itself. And the financial evidence is starting to back that up across Stars, MLR, and audit exposure simultaneously.
Stars and outcomes
Coding for hypertension gets you a RAF credit whereas controlling a member’s blood pressure gets you a Stars measure. CMS has been steadily increasing the weight of clinical outcome measures, and in 2026 that weight is impossible to ignore. MA plans that closed actual clinical gaps, not just documented them, are seeing it in their ratings and in the bonus payments tied to them.
The MLR math
The revenue lift from capturing ten minor chronic condition codes doesn’t come close to the cost of one avoidable hospitalization. Every unnecessary admission hits the MLR directly and with CMS tightening benchmark rates, MA plans don’t have the margin to absorb that. In a 100% V28 world where many of those codes no longer generate meaningful RAF credit anyway, the math decisively favors keeping members out of hospitals over chasing marginal diagnosis credits.
Cost reduction through preventive care
Closing a care gap for a diabetic member before they progress to a complication avoids downstream costs that dwarf the cost of the intervention itself. CDC-recognized diabetes prevention programs have demonstrated this concretely, cutting diabetes onset from 29% to 14% over three years, with an 88% probability of net savings per participant. MA plans with proactive chronic disease outreach are finding that prevention does double duty: improving member outcomes and reducing the high-cost utilization that erodes MLR at the same time.
Audit-proofing through care delivery
If you treat a member for the condition you coded, the treatment record is the proof. The visits, lab results, and care plan adjustments exist naturally because care happened. MA plans that treat what they code are building RADV-resilient records without a separate documentation strategy. The care itself becomes the compliance. That’s the design principle behind platforms like blueBriX.
The case for delivering better care is clear. But intention without the right infrastructure is just strategy on paper. For most MA plans, the bottleneck isn’t the will to change. It’s the technology stack that was never built for it.
The technology gap that's quietly costing MA plans
In 2026, the speed at which a MA plan can move from identifying a risk to acting on it is no longer an operational preference. It’s a competitive and compliance requirement.
The silo problem
Most MA plans are running two parallel worlds. There’s a coding tool in the back office identifying risk gaps and HCC opportunities. And there’s a care management tool that nurses and care coordinators use to manage member outreach and interventions. In most organizations, these two worlds don’t talk to each other.
That gap is more dangerous than it looks. When a coding tool flags a risk gap, but that flag never becomes a clinical task for a provider, nothing happens. The member doesn’t get the care. The condition doesn’t get managed. But the code gets submitted. To CMS and to the DOJ, that’s not a technology problem. That’s a paper trail of neglect. And in a RADV audit, it’s exactly the kind of disconnect they’re looking for.
The 72-hour test
Here’s a practical way to pressure-test your current setup: if your system identifies a high-risk member today, how long does it take for a provider to have an actionable clinical task in front of them? If the answer involves manual handoffs, spreadsheet exports, or a weekly review meeting, the answer is probably too long.
In 2026, the window between identifying a risk and acting on it has to shrink. A diagnosis that sits unaddressed for weeks isn’t just a care gap. It’s a liability gap. MA plans that are winning operationally have closed the distance between their risk identification workflows and their care delivery workflows, often down to hours rather than days. Platforms like blueBriX are built specifically around that gap.
Agility as the new infrastructure
Better care in 2026 doesn’t just require better intentions. It requires systems that can translate a clinical insight into a provider action in near real time. That means risk data and care management data living in the same environment, not syncing between two separate platforms on a weekly batch schedule. It means care coordinators seeing the same risk picture that the coding team sees. It means providers receiving clinically relevant, actionable information at the point of care, not three weeks after a chart review was completed.
The MA plans closing this gap aren’t necessarily the largest ones. They’re the ones that recognized the silo problem for what it is: not a workflow inconvenience, but the single biggest bottleneck between their current performance and where the market is heading.
That’s exactly the gap blueBriX is built to close. Here’s what that looks like in practice.
Beyond the capture model: Orchestrating agile care with blueBriX
Let’s see how blueBriX connects the dots between risk identification, care delivery, and audit readiness.
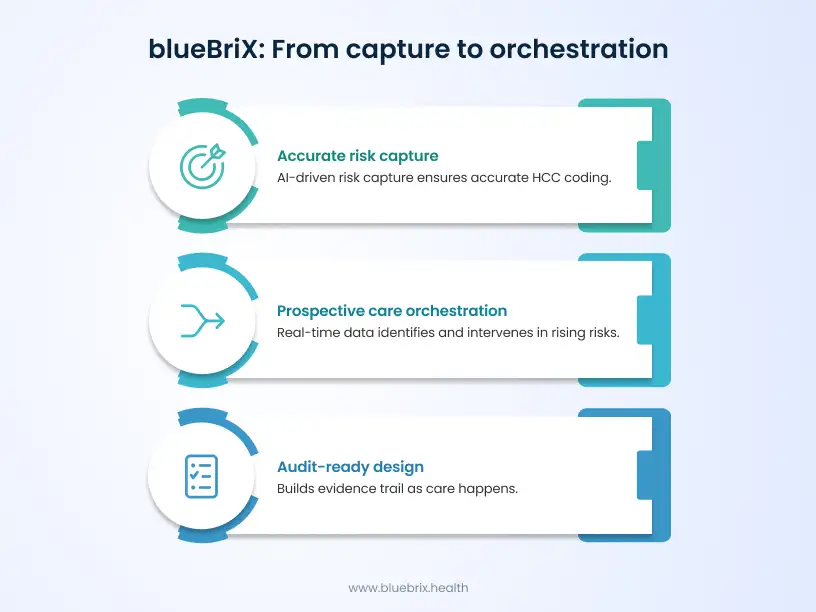
Accurate risk capture at the point of care
The most common revenue leak in MA isn’t fraud. It’s under-specificity. A condition gets coded, but not at the level of complexity the patient actually has. The RAF score falls short and the revenue that should have followed the patient’s true condition burden doesn’t show up.
blueBriX’s AI addresses this at the point of care. When a provider enters a clinical note, the AI surfaces relevant HCC codes, flags supporting codes that reflect the full complexity of the condition, and for high-weight diagnoses, prompts for the specific documentation needed to back them up. Everything is validated before submission.
Prospective care orchestration
The capture model was always looking backward. blueBriX shifts the timeline forward, orchestrating care as it happens.
blueBriX’s rule engine continuously ingests real-time data, pharmacy fills, lab results, and SDOH signals, to identify rising-risk members before they hit the ER. No waiting for a claim. No retrospective chart pull.
When a risk shift is detected, the rule engine instantly alerts the care team to intervene before the condition escalates. Every alert and intervention is documented in real time, so every reported condition has a clinical action behind it. No unanswered diagnoses. No compliance risk.
When a provider opens blueBriX, they see a unified task list: “Verify this V28 HCC, perform this A1c check, and schedule the pharmacist follow-up.” The risk, the quality gap, and the care need to be resolved in a single visit.
Audit-ready by design
In the age of RADV extrapolation, assembling documentation after an audit notice arrives is too late.
blueBriX builds the evidence trail as care happens. Every clinical action, from a telehealth check-in to a medication adjustment, is automatically logged and linked to the relevant diagnosis in real time. Nothing is chased down after the fact.
When auditors arrive, there is no scramble. Every submitted diagnosis has a corresponding clinical action behind it, timestamped, linked, and ready. That’s what happens when you treat the patient you coded for.
In a world where a single documentation gap can trigger a multimillion-dollar claw back, the live evidence trail isn’t a nice-to-have. It’s your strongest defense.
Don’t let V28 impact your revenue — get your personalized impact assessment
2026 is already costing plans that haven’t made the shift. The window to course-correct is open. Request your personalized V28 impact assessment and see how blueBriX orchestrates the care that protects your revenue.
Connect with our team today