

Quick answers: behavioral health EHR evaluation in 2026
If you’re short on time, the four questions below cover what most behavioral health leaders are actually trying to figure out before they buy. Each links into the deeper section of the guide where the topic is fully unpacked.
What is the best EHR for behavioral health in 2026?
There’s no single best EHR for behavioral health. The right answer depends on your size, payer mix, CCBHC or CMHC status, ACO participation, and whether your quality team is currently abstracting measures by hand. What separates the strong behavioral health EHR vendors from the rest is whether eCQM measure logic, MSSP APP Plus reporting, FHIR R4 interoperability, and integrated RCM live natively on the platform or whether they’re bolted on through third-party integrations. The seven capabilities in this guide are the practical evaluation criteria. For a side-by-side comparison of the top platforms, see top 8 Behavioral Health EHRs to Consider for Practices.
What does behavioral health EHR software need to do for eCQM reporting?
An EHR for behavioral health that genuinely supports eCQM reporting needs four things working together: native measure logic for the 2026 specifications (not third-party integrations), automated denominator and numerator capture during routine documentation, FHIR R4 architecture with QRDA-III and FHIR JSON submission support, and structured data capture for screening tools and SDOH that flows into measure calculations without manual abstraction. If any of those are missing, your quality team is doing the work the platform should be doing, which is where the $250,000 to $400,000 annual abstraction cost comes from. We’ll break down each capability with vendor evaluation questions.
Is blueBriX a value-based care platform built for behavioral health?
Yes. blueBriX is a value-based care platform purpose-built for behavioral health organizations participating in CCBHC certification, Medicaid Core Set reporting, MSSP APP Plus, and ACO LEAD. The value-based care solutions on the platform with eCQM automation, FHIR R4 interoperability, integrated RCM, SDOH capture, and care coordination across Medicare and Medicaid lines of business, are the same workflows that produce your quality reporting submissions. In this guide, we’ll walk you through the specific capabilities and a 13-week implementation timeline.
How does behavioral health practice management connect to quality reporting?
Quality reporting is a downstream output of how your practice runs day to day. When behavioral health practice management with scheduling, documentation, billing, and outcomes tracking, lives on the same platform as eCQM measure logic, screening tools, and care coordination, your quality measures populate as a byproduct of routine clinical and operational work. When practice management runs on a separate system from your EHR, the data has to be reconciled, and that reconciliation is where measure denominators get incomplete and numerators get missed. We also cover how blueBriX consolidates these workflows on a single platform.
Introduction: the audit that changes everything
Picture a Monday morning at a mid-size CCBHC.
The state sends notification of a quality data audit — 48 hours to produce documentation proving the clinic met depression screening and follow-up targets for 2,500 Medicaid patients in the previous measurement period.
The quality team immediately opens three separate systems. Someone pulls charts. Someone else cross-references claims data. A third person is manually building a spreadsheet. By late evening, the numbers don’t match. Two hundred records are either incomplete, duplicated across systems, or missing follow-up documentation entirely.
The organization misses the audit window. A quality bonus payment worth $80,000 is delayed pending review. The clinical director spends the next six weeks in remediation mode instead of running quality improvement initiatives.
This isn’t a hypothetical. Variations of this scenario play out across behavioral health organizations every reporting period. And in 2026, with Medicaid Core Set reporting already mandatory, CMS actively transitioning all quality measures to digital quality measures (dQMs), and value-based care contracts controlling an ever-larger share of reimbursement, the organizations still running quality reporting on manual abstraction and spreadsheets are accumulating risk they haven’t fully priced.
The solution isn’t working harder on the spreadsheets. It’s buying the right platform.
This guide is for every decision-maker involved in a behavioral health EHR evaluation whether you’re the CEO calculating ROI, the Clinical Director evaluating workflow impact, the IT Director assessing technical requirements, or the Quality Manager who has been quietly absorbing the manual abstraction burden for years. We’ll cover what genuine eCQM readiness looks like in a platform, which questions expose the difference between real capability and marketing language, and what you should see in a demo before you sign anything.
Why this behavioral health EHR evaluation is different from your last one
The behavioral health EHR market in 2026 looks fundamentally different from even three years ago. Platforms have matured, but so have the compliance requirements they’re supposed to handle. The gap between a platform that can store clinical data and one that automates quality compliance has never been wider and that gap is now a direct financial variable.
What changed in 2026
Several 2026-specific factors make this evaluation more urgent than previous cycles:
Mandatory Medicaid Core Set reporting is already live.
Mandatory reporting of Medicaid Core Set behavioral health measures began in 2024 under 42 CFR Parts 433, 437, and 457. If your organization participates in Medicaid, your behavioral health quality data is no longer optional to collect and submit accurately. The 2026 reporting period (covering services provided primarily in 2025) runs Fall 2026 and the window to fix infrastructure gaps is now.
CMS is transitioning all quality measures to digital quality measures.
This is the stated CMS strategic roadmap. Digital quality measures use standardized digital data from multiple sources via interoperable FHIR API-based systems. Organizations without FHIR R4-native EHR infrastructure are increasingly locked out of the most advanced quality reporting programs — limiting access to higher-value VBC contracts.
2026 eCQM specifications are updated and in effect.
CMS published updated eCQM specifications for the 2026 reporting/performance period in May 2025 (eCQI Resource Center). Annual specification updates affect measure logic, value set definitions, and code system mappings. If your EHR vendor hasn’t pushed those updates to your instance, you may be calculating quality scores against outdated measure definitions right now.
FHIR R4 compliance is mandatory for certified health IT.
The ONC 21st Century Cures Act HTI-1 Final Rule requires FHIR R4 support as of January 2025 and mandates USCDIv3 data elements via FHIR APIs. This is the current baseline. Vendors who still treat FHIR as an optional add-on are not compliant with current certified health IT standards.
Telehealth quality reporting requirements have expanded.
With behavioral health organizations having significantly expanded virtual care delivery, CMS updated telehealth guidance for eCQMs for the 2026 performance period. If your telehealth visits run through a platform that isn’t natively integrated with your quality reporting infrastructure, those clinical encounters may not be populating your quality measure denominators and numerators correctly.
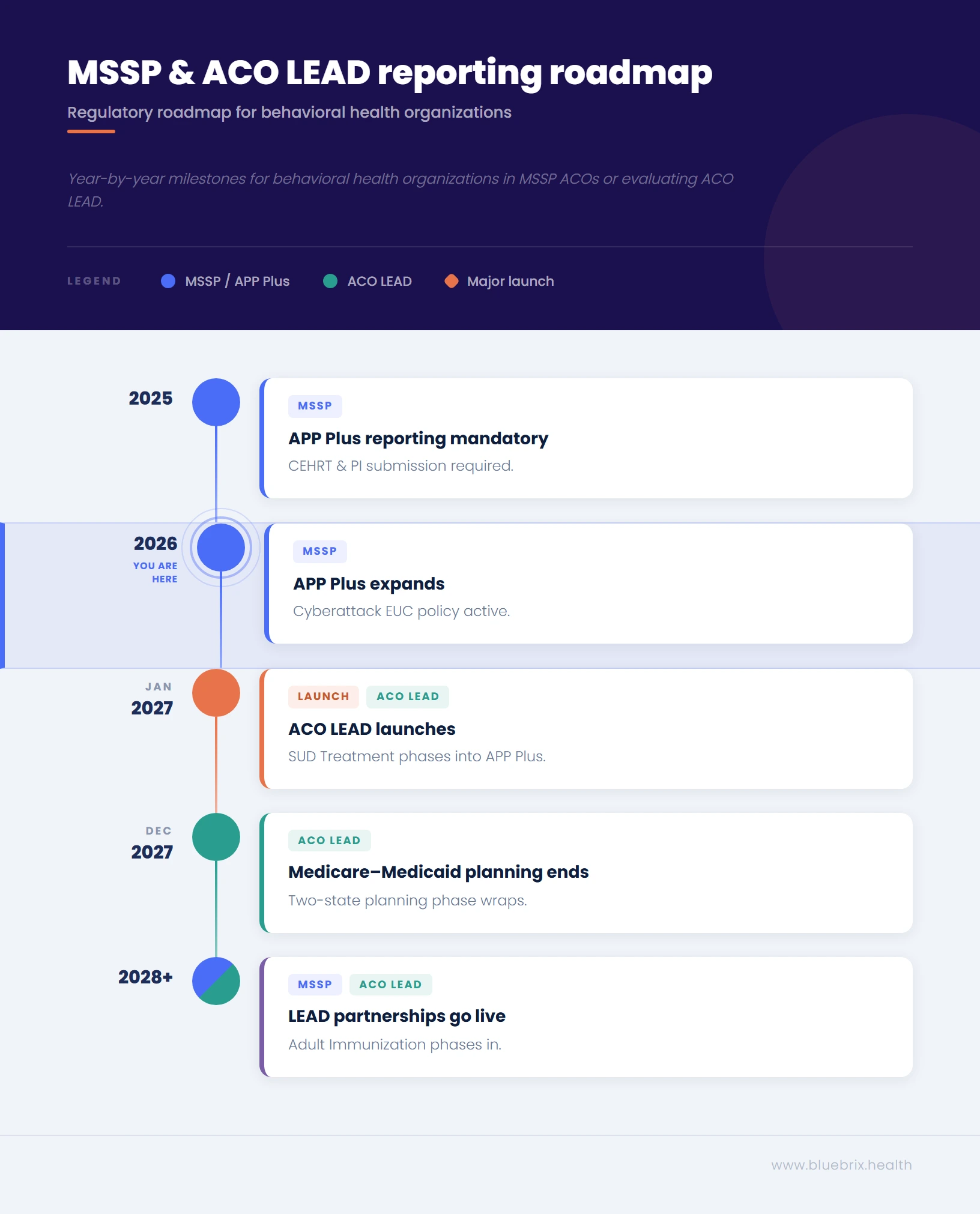
If you’re in an MSSP ACO, your reporting obligations are expanding and ACO LEAD launches January 2027.
The CMS Web Interface sunset after 2024 reporting. If your ACO participates in the Medicare Shared Savings Program, you’re now reporting the APP Plus quality measure set via eCQMs, MIPS CQMs, or Medicare CQMs and that set is evolving. The APP Plus set finalized in the CY 2026 Physician Fee Schedule Final Rule includes Diabetes Glycemic Status (#001), Depression Screening and Follow-up Plan (#134), Controlling High Blood Pressure (#236), Breast Cancer Screening (#112), Colorectal Cancer Screening (#113, phasing in PY 2026), Risk-Standardized Hospital Admission Rates (#484, PY 2026), Initiation and Engagement of Substance Use Disorder Treatment (#305, phasing in PY 2027), and Adult Immunization Status (#493, PY 2028 or one year after the eCQM specification becomes available, whichever is later), plus CAHPS for MIPS (#321) and the Hospital-Wide Readmission rate (#479).
Two of those measures — Quality ID #134 Depression Screening and Quality ID #305 SUD Treatment — run almost entirely through your behavioral health workflows. (Note: CMS finalized the removal of Quality ID #487 Screening for Social Drivers of Health from APP Plus in the CY 2026 Final Rule, reversing the proposed phase-in.)
Separately, CMS announced in December 2025 that ACO REACH will be replaced on January 1, 2027 by the Long-term Enhanced ACO Design (LEAD) Model: a 10-year voluntary model focused on dually eligible Medicare and Medicaid beneficiaries and other high-needs populations, with a quality measure set that includes two eCQMs phased in over time (CMS Innovation Center). If you serve dually eligible beneficiaries, this is the model you’ll want to evaluate.
Manual quality abstraction costs close to half a million
Before evaluating any platform, every stakeholder in your organization needs to understand what manual quality abstraction is actually costing. The costs are distributed, which makes them easy to underestimate individually and shocking when added up.

The revenue math
- Direct labor: A mid-size CCBHC or CMHC with 20–50 providers typically requires 1–2 FTE positions dedicated primarily to quality data abstraction and reporting preparation. At fully-loaded salary costs of $55,000–$70,000 per FTE, that’s $110,000–$140,000 annually in labor dedicated to a process that a properly configured platform handles continuously in the background.
- Missed VBC bonuses: Quality bonuses and shared savings distributions in value-based contracts are gated on performance scores. Organizations with incomplete or late quality data submissions routinely miss the performance thresholds needed to qualify. A single missed quality bonus cycle at a mid-size behavioral health organization can represent $50,000–$200,000+ in foregone revenue, depending on contract structure.
- Month-end close delays: When quality data and financial data live in separate systems, month-end reconciliation requires manual consolidation of EHR clinical data, clearinghouse claims data, and bank deposit data — a process that routinely takes 10–15 days to finalize. The C-suite is flying blind on actual financial performance for two weeks of every month.
- Audit exposure: Poor communication and data gaps contribute to more than $11 billion in avoidable healthcare costs annually in the U.S. (Journal of Patient Safety). Manual abstraction introduces human error into the data that quality audits are based on — and incorrect measure denominator inclusions, missed exclusions, or documentation gaps don’t just affect scores, they create regulatory risk.
The fully-loaded cost of manual quality reporting at a mid-size behavioral health organization often exceeds $250,000–$400,000 annually when labor, missed bonuses, and operational drag are combined.
The operational drain
Quality teams at mid-to-large behavioral health organizations report being “burdened by existing quality oversight requirements” with limited remaining capacity for actual quality improvement initiatives (NCQA Behavioral Health Quality Framework, 2021). More than 40% of healthcare organizations spend 10–20+ hours per week troubleshooting data issues caused by fragmented systems (Rhapsody 2025 State of Interoperability Report).
Manual chart abstraction, the practice of having quality staff pull individual records to determine whether patients meet measure inclusion criteria and received appropriate interventions, is not just time-consuming. Research characterizes it as “labor-intensive and unreliable” with questionable validity across fragmented care settings (Journal of Patient Safety). When the same patient’s data lives in your EHR, a separate crisis intervention system, a hospital’s EHR following an inpatient stay, and a clearinghouse, systems that don’t talk to each other, manual abstraction produces quality measure calculations that are incomplete by design.
The integration tax
IT teams at behavioral health organizations face a specific version of this problem. Many EHR vendors handle quality reporting through third-party point solutions: a separate quality analytics vendor connects to your EHR via integration, applies their own measure logic, and submits on your behalf. The operational risk in this configuration is significant. Data accuracy and integrity are at higher risk when a vendor other than your core platform aggregates and prepares quality reporting submission (Koan Health, 2024). When data discrepancies occur, accountability diffuses across vendors and identifying where the breakdown happened takes weeks.
55% of healthcare IT leaders cite legacy infrastructure as their biggest barrier to interoperability (Rhapsody 2025 State of Interoperability Report). In behavioral health specifically, most EHR vendors are not yet fully FHIR-compliant, creating fragmented data that directly affects both integrated care delivery and quality reporting accuracy. Adding integration connections to address this fragmentation comes at significant cost and the “interface tax” can run $25,000+ per connection.
The workflow burden
Every hour a clinical staff member spends doing retrospective chart review for quality measure validation is an hour not spent on care coordination, patient follow-up, or closing actual care gaps. The irony of manual quality abstraction is that the effort required to prove care quality is being delivered comes at the direct expense of the time and attention that would improve care quality.
Documentation burden is the top driver of clinician burnout in behavioral health settings. An EHR that automates quality data capture at the point of care — so that a completed PHQ-9 screening simultaneously satisfies the depression screening quality measure without any additional staff action — doesn’t just save operational cost. It returns clinical bandwidth to clinical work.
What eCQM-ready actually means: a technical buyer's checklist
Every platform claims to be eCQM-ready. Here’s what it actually means in practice, and the questions that separate real capability from checkbox compliance.
Capability 1: native eCQM measure logic
What it means: The EHR contains the quality measure specifications, value set mappings, and CQL (Clinical Quality Language) logic natively, meaning quality measure calculations run inside the platform against your clinical data, not in a third-party system connected via integration.
Why it matters: Native measure logic is the difference between real-time quality performance visibility and monthly batch reports from a vendor who may or may not be calculating against current specifications.
Check with your vendors:
- Where does your eCQM calculation engine live — natively in the EHR, or in a connected third-party system?
- Can you show me a live quality performance dashboard calculated against actual patient data, not sample data?
- How do you handle payer-specific measure definition differences between CMS and commercial payers?
Capability 2: Automatic VSAC Value Set Updates
What it means: CMS releases updated value sets through the Value Set Authority Center (VSAC) quarterly. An eCQM-ready platform applies these updates automatically — your IT team doesn’t download files and your quality team doesn’t re-map measure logic.
Why it matters: Value set changes affect which patient encounters and clinical events count toward quality measure numerators and denominators. Calculating quality scores against outdated value sets produces incorrect performance data. If your scores are wrong, your VBC performance calculations are wrong.
Questions to ask vendors:
- How are VSAC value set updates applied to your platform, and who is responsible for applying them?
- What is your update timeline from CMS publication to deployment in our instance?
- Is annual measure specification maintenance included in our subscription, or is it a professional services engagement?
Capability 3: FHIR R4 Native Architecture
What it means: The platform is built on FHIR R4 as a foundational data model — not a FHIR API bolted onto a legacy architecture as a compliance workaround.
Why it matters: CMS’s transition to digital quality measures requires FHIR-based data exchange across multiple sources. Organizations on legacy EHR architectures will face increasing friction as dQM requirements expand. FHIR R4 native also enables the interoperability required to aggregate data from external sources — hospital systems, crisis intervention providers, HIEs, PDMPs — into unified quality calculations.
Questions to ask vendors:
- Is FHIR R4 your native data model, or is it an API layer added to a legacy architecture?
- Are you ONC-certified under the HTI-1 Final Rule requirements for FHIR R4 and USCDIv3?
- How do you handle data aggregation from clinical encounters that occur outside your platform — hospitalizations, crisis services, external specialists?
Capability 4: CCBHC and CMHC Measure Pre-Configuration
What it means: The platform arrives pre-configured for CCBHC-specific quality metrics and CMHC state reporting requirements — including both clinic-collected and state-collected measures — rather than requiring your IT team to build these configurations from scratch.
Why it matters: CCBHCs must report measures across 8 required service types under the Section 223 Demonstration Program, including CMS Medicaid Adult/Child Core Set measures like Screening for Depression and Follow-Up Plan (CDF-AD, CDF-CH) and Use of Pharmacotherapy for Opioid Use Disorder (OUD-AD). Quality Bonus Payments under CCBHC certification are tied to these measure performance scores. A platform that doesn’t arrive pre-configured for these measures requires significant implementation investment and ongoing maintenance.
Questions to ask vendors:
- Which CCBHC quality measures are pre-configured in your platform out of the box?
- How do you handle the distinction between clinic-collected and state-collected measures?
- When SAMHSA updates the CCBHC Quality Measures Technical Specifications Manual, how are those changes reflected in your platform?
Capability 5: Real-Time Quality Performance Dashboards
What it means: Leadership and quality teams can see quality measure performance scores in real time — against current measure targets, with drill-down to individual patient-level gaps — before reporting deadlines, not after.
Why it matters: A reactive quality reporting posture — discovering performance gaps at submission time — is how organizations miss bonuses and fail audits. Real-time dashboards enable proactive care gap closure during the measurement period, when intervention can still affect outcomes.
Questions to ask vendors:
- Can you show me a live quality dashboard with current performance data against 2026 measure targets?
- Can staff drill down from measure-level scores to patient-level care gaps?
- How does the dashboard handle multi-location reporting — can we see performance aggregated at the network level and broken down by site?
Capability 6: Integrated Revenue Cycle Management
What it means: Clinical quality performance data and revenue cycle data live in the same platform — so quality scores, claims status, and financial performance are visible together, without requiring a separate data consolidation process.
Why it matters: In value-based care contracts, quality performance is a direct financial variable. When quality and RCM live in separate systems, the C-suite cannot see how quality performance is affecting reimbursement in real time. Separate systems also create the month-end reconciliation burden that delays financial reporting by 10–15 days.
Questions to ask vendors:
- Is RCM a native component of your platform, or a separate product with a data integration?
- Can your CFO-level dashboards show quality performance scores alongside reimbursement impact from the same interface?
- How does your platform handle multi-payer behavioral health billing — Medicaid, Medicare, commercial payers, and grants — in a single system?
Capability 7: SDOH Data Capture and Closed-Loop Tracking
What it means: The platform supports standardized SDOH screening tools (PRAPARE, AHC-HRSN), community resource referral directories, and closed-loop tracking that confirms whether patients accessed referred services — with SDOH data flowing into quality measure calculations and Z-code documentation automatically.
Why it matters: A growing number of quality measures now incorporate SDOH elements, and value-based care contracts increasingly require Z-code documentation, community health worker intervention tracking, and social needs outcome reporting. Organizations treating SDOH as a separate workflow from quality reporting are doing double the work for half the credit.
Questions to ask vendors:
- Which SDOH screening tools are built into your platform natively?
- How does SDOH data flow into quality measure calculations and ICD-10 Z-code capture?
- Does your platform support community resource referral with closed-loop tracking — can we confirm whether a patient accessed a referred service?

What your behavioral health EHR needs to do if you’re in an MSSP ACO or evaluating ACO LEAD
If you’re already participating in an MSSP ACO whether as a behavioral health partner inside a primary care–led ACO, a contracted specialty provider, or part of a CCBHC- or CMHC-anchored arrangement, your data is no longer just your data. The ACO’s shared-savings calculation now runs partly through your EHR. The same is true if you’re evaluating ACO LEAD for a January 2027 start: a model designed around dually eligible Medicare and Medicaid beneficiaries places your behavioral health workflows squarely in the middle of every meaningful quality measure.
A peer-reviewed 2022 study of MSSP ACOs found that just 9% of ACOs use a single EHR system, while 77% use six or more (Perloff & Sobul, American Journal of Managed Care, January 2022). Your ACO is almost certainly aggregating data across a CCBHC, a CMHC, primary care groups, and an FQHC and accurate APP Plus reporting depends on every one of those systems producing comparable, all-payer/all-patient eCQM data. The cleaner your data flows out of your EHR, the more leverage you have inside the ACO.
The APP Plus measures you’re directly responsible for
Per the CY 2026 Physician Fee Schedule Final Rule, your ACO reports the APP Plus measure set on an all-patient, all-payer basis — the population covered by every participating provider, not just Medicare FFS beneficiaries (when reporting via eCQMs/MIPS CQMs). Several APP Plus measures sit inside your clinical workflow:
- Quality ID #134 — Preventive Care and Screening: Screening for Depression and Follow-Up Plan: Patients age 12 and older screened with a standardized tool, with a documented follow-up plan if positive. CMS specifically refined this measure’s guidance and numerator specifications in the CY 2026 Final Rule. The follow-up plan is where most ACOs lose performance points — and that follow-up almost always lives in your workflow, not your primary care partner’s.
- Quality ID #305 — Initiation and Engagement of Substance Use Disorder Treatment (phasing in for PY 2027): CMS confirmed this measure for APP Plus inclusion in PY 2027. If you run SUD service lines, what was previously a grant-funded compliance exercise becomes a Medicare shared-savings input the moment that measure goes live.
- Screening for Social Drivers of Health removed from APP Plus: CMS finalized removal of Quality ID #487 Screening for Social Drivers of Health from the APP Plus measure set in the CY 2026 Final Rule.SDOH screening still matters for your CCBHC certification, Medicaid Core Set reporting, and several other VBC contracts,but it’s no longer driving your ACO’s APP Plus quality score. The capability you build for SDOH (Capability 7 above) is still strategic; it just isn’t the APP Plus pressure point we previously expected it to be.
- Quality ID #484 — Clinician and Clinician Group Risk-Standardized Hospital Admission Rates (administrative claims, PY 2026): A claims-based measure, but your follow-up after psychiatric hospitalization, medication management, and crisis intervention drive readmission rates more than almost anything else in the ACO and that flows straight into the composite score.
Why ACO LEAD changes the calculus for your organization
The Long-term Enhanced ACO Design (LEAD) Model launches January 1, 2027 as the formal successor to ACO REACH (CMS Innovation Center). Three of its design features matter directly to you:
- Dually eligible and high-needs focus: CMS designed LEAD specifically around dually eligible Medicare and Medicaid beneficiaries and high-needs patients, including those who are homebound or home-limited (CMS LEAD Model). That population has substantially higher behavioral health and SUD prevalence than the general Medicare population — which is why a LEAD ACO without you in it can’t meaningfully manage its assigned beneficiaries.
- Medicare–Medicaid integration component: CMS plans to select two states for an initial planning phase running through December 2027 to develop a framework for ACO–Medicaid partnership arrangements (CMS LEAD Model; Center for Health Care Strategies, 2026). If you already operate across both Medicaid and Medicare lines of business, this is the first federal model that aligns those two funding streams within a single accountable care arrangement. The data infrastructure you need to operate inside it has to span both, and your EHR has to handle that without forcing dual workflows.
- An entry path designed for smaller, independent, and rural participants. Unlike earlier ACO models, LEAD is built to draw in smaller, independent, and rural participants including those new to ACOs with full historical experience as the benchmark plus an add-on (CMS; AMA, December 2025). If you’re a rural CMHC or a small CCBHC that previously had no realistic ACO entry path, you do now, provided your EHR can produce ACO-grade quality data.
LEAD’s quality framework uses point-based scoring with a 3% quality withhold tied to performance, and eCQMs are phased in over time, starting as reporting-driven measures with bonus opportunities and evolving into core performance measures (CMS LEAD Model RFA; MD interactive analysis, April 2026). You’ll also need to implement a prevention and quality plan tailored to your population, which for a high-BH-prevalence dually eligible population means BH-specific clinical workflows and data capture have to be ready out of the box.
What this means for your EHR evaluation
If you’re currently in an MSSP ACO or expect to be in one, or are evaluating ACO LEAD, four EHR capabilities move from “nice to have” to “disqualifying if missing”:
- Certified EHR Technology and Promoting Interoperability submission. Beginning in PY 2025, ACO participants, providers, and professionals who are MIPS-eligible clinicians, Qualifying APM Participants, or Partial QPs must be on Certified EHR Technology (CEHRT) and submit Promoting Interoperability data, regardless of MSSP track (CMS CY 2024 Final Rule, in effect for PY 2025). The rule allows specific exclusions for small practices, non-patient-facing clinicians, hospital-based clinicians, and ASC-based clinicians, plus hardship exceptions. But for most outpatient BH organizations participating in MSSP ACOs, a non-CEHRT EHR is a participation barrier that your ACO won’t want to absorb at scale.
- QRDA-III and FHIR JSON submission support. APP Plus eCQM submissions to CMS happen via QRDA-III XML or FHIR JSON formats. If your EHR can’t produce these natively, your ACO is paying a third-party aggregator to do it — and the data accuracy risk noted earlier in this guide multiplies every time your data has to round-trip through a separate vendor.
- All-payer/all-patient eCQM data on a single platform. APP Plus eCQM/MIPS CQM reporting requires data on every patient your providers see, not just Medicare beneficiaries. If your EHR segregates Medicare, Medicaid, and commercial workflows, your ACO inherits a reconciliation problem the ACO won’t want to solve twice.
- Cyberattack EUC readiness. CMS expanded MSSP Extreme and Uncontrollable Circumstances (EUC) policies in the CY 2026 Final Rule to include cyberattacks — ransomware and malware affecting an ACO at the legal entity level. Your EHR’s security posture is now part of your ACO’s risk profile, not just yours. Your ACO will ask about it; you’ll want a confident answer.
Questions to ask vendors:
- Are you currently submitting APP Plus eCQM data on behalf of any MSSP ACO clients today, and can you walk us through that submission workflow end to end?
- When our patients also see ACO participants on a different EHR, do we hand our ACO a clean QRDA file, or does the ACO have to reconcile our data downstream?
- For ACO LEAD specifically: how does your platform support care coordination across Medicare and Medicaid lines of business for our dually eligible beneficiaries, and how does that data flow into APP Plus and LEAD measure calculations?
What a genuine behavioral health EHR platform demo should show you
A behavioral health EHR demo is a sales presentation until you ask the right questions. Here’s what each decision-maker in your evaluation should specifically request to see.
What the c-suite should see
Ask to see a financial impact dashboard that shows quality performance scores alongside VBC revenue projections in the same view. Ask the vendor to walk you through what happens when a quality bonus threshold is missed — how does the platform surface that risk before reporting season ends, and what does the intervention workflow look like? Ask specifically about the total cost of ownership: what’s included in the subscription versus what triggers a professional services engagement or add-on fee?
Red flags: Vague answers about “additional modules” for quality reporting, inability to show integrated financial and quality data in a single view, or pricing structures that charge per-quality-measure or per-integration.
What clinical directors and quality managers should see
Ask to see a live quality measure performance report calculated against real clinical data — not a sample environment. Request a demonstration of how a completed PHQ-9 screening flows from clinical documentation into a depression screening quality measure, with no additional staff action. Ask specifically how the platform handles payer-specific measure definition differences for the same clinical measure across different contracts.
Red flags: Quality dashboards that require a manual data export step, measure calculations that run on a batch schedule rather than in real time, or inability to distinguish between CMS and commercial payer measure definitions within the same interface.
What IT directors should see
Ask for the platform’s ONC certification documentation and FHIR R4 compliance evidence. Request a technical architecture overview that distinguishes between native FHIR implementation and FHIR API wrapper over a legacy system. Ask specifically how the platform handles data aggregation from clinical encounters outside the EHR — hospitals, external crisis providers, HIEs — and what the integration architecture looks like for each external connection.
Red flags: FHIR described as a future roadmap item, integration costs quoted on a per-connection basis, or quality reporting handled by a third-party vendor not present in the demo.
What care coordinators and clinical staff should see
Ask to walk through a complete clinical encounter from documentation to quality measure capture — specifically, how does completing a required assessment or intervention satisfy a quality measure without any separate data entry step? Ask how the platform handles care coordination across providers and settings, including external referrals and community partner follow-up. Ask what the documentation burden looks like at point of care compared to your current system.
Red flags: Quality measure documentation that requires a separate workflow from regular clinical documentation, care coordination features that don’t surface patient-level quality gaps during encounters, or SDOH referral tracking that exists in a separate module disconnected from quality reporting.
Why blueBriX is purpose-built for behavioral health eCQM compliance
Most behavioral health EHR platforms were built for a healthcare environment that preceded mandatory eCQM reporting, FHIR R4 requirements, and value-based reimbursement as a dominant revenue model. They’ve been patched toward compliance rather than designed for it.
blueBriX was built from the ground up for the behavioral health organizations for whom eCQM compliance, CCBHC certification, Medicaid Core Set reporting, and value-based care performance aren’t optional features, they’re the operational core.
Here’s how blueBriX meets the buyer’s guide criteria above:
Automated eCQM data capture at the point of care.
In blueBriX, clinical documentation and quality measure capture are the same action, not sequential actions. When a clinician completes a PHQ-9 and documents the result, that data simultaneously satisfies the depression screening quality measure. No retrospective chart review. No quality team abstraction step. No manual data entry into a separate reporting system.
Annual eCQM specification updates included in your subscription — deployed within 30 days of CMS publication.
When CMS publishes annual eCQM specification changes (typically each May), blueBriX updates measure logic within 30 days. VSAC value sets update automatically quarterly. Your IT team doesn’t download files. Your quality team doesn’t re-map logic. Your vendor doesn’t invoice you for professional services. This is operational continuity, included.
FHIR R4 native architecture, ONC-certified.
blueBriX is built on FHIR R4 as a native data model — not as an API wrapper over legacy infrastructure. This enables the FHIR-based data exchange that CMS’s dQM transition requires, supports integration with state HIEs and external data sources without the interface tax, and satisfies the ONC HTI-1 Final Rule requirements for certified health IT.
CCBHC and CMHC pre-configured out of the box.
blueBriX arrives pre-configured for CCBHC quality metrics across all 8 required service types, including both clinic-collected and state-collected measures and pre-built reporting for Medicaid Core Set, grant funding, and state-specific compliance frameworks. When SAMHSA updates CCBHC specifications, blueBriX updates measure configuration to match.
Real-time quality performance dashboards with patient-level care gap visibility.
blueBriX provides leadership and quality teams with real-time measure performance scores against current targets, with drill-down capability to individual patient-level gaps so care coordination teams can close gaps during the measurement period — not after reporting deadlines have passed.
Integrated RCM — one platform for clinical and financial operations.
blueBriX combines EHR functionality with Revenue Cycle Management services in a single platform. Your CFO can see quality performance scores and reimbursement impact together. Month-end reconciliation doesn’t require consolidating three separate data sources. VBC bonus eligibility is visible in real time, not reconstructed weeks after the performance period ends.
Closed-loop SDOH tracking integrated with quality reporting.
blueBriX supports standardized SDOH screening tools, community resource referral directories, and closed-loop tracking from referral made through service confirmed. SDOH data flows automatically into Z-code documentation and quality measure calculations — transforming SDOH from a checkbox compliance exercise into a care coordination tool that simultaneously satisfies quality reporting requirements.
Built for the way you participate in MSSP ACOs and ACO LEAD.
blueBriX is built on Certified EHR Technology with native FHIR R4, captures APP Plus eCQM data on an all-payer/all-patient basis, and produces submission-ready files in the formats your ACO needs. That means your depression screening (Quality ID #134), follow-up after psychiatric hospitalization, and the SUD treatment measure (Quality ID #305) phasing in for PY 2027 are populated as a byproduct of the documentation your clinicians are already doing — not a separate abstraction project that lands on your quality team. If you’re evaluating ACO LEAD for January 2027, blueBriX’s integrated RCM, dual-eligibility-aware billing, and care coordination across Medicare and Medicaid lines of business support the Medicare–Medicaid integration component that makes LEAD distinct from earlier ACO models.
Implementation timeline: 13 weeks from contract to go-live.
For a mid-size CCBHC (20–50 providers, 3–5 locations): Weeks 1–4 for data migration and system configuration; Weeks 5–8 for quality measure specification and workflow customization; Weeks 9–12 for staff training and parallel testing; Week 13 for go-live with automated quality reporting fully operational.
Choosing a behavioral health EHR vendor: how to compare your shortlist
By the time you reach a final shortlist, most behavioral health EHR vendors will tell you a similar story: certified, FHIR-ready, eCQM-capable, scalable. The work of evaluating an EHR for behavioral health is separating what’s genuinely operational from what’s on a roadmap slide. The seven capabilities, the four MSSP/LEAD-specific items, and the demo asks mentioned above are designed to do that separation for you.
A few framing principles to bring into the conversation with each vendor on your shortlist:
Treat “EHR” and “value-based care solutions” as the same purchase, not two.
Behavioral health EHR software that can’t produce APP Plus eCQMs, support all-payer/all-patient reporting, and feed quality data into your ACO’s submission workflow isn’t actually a VBC platform — even if the website says it is. Test for the workflow, not the marketing.
Compare BH-specific vendors against horizontal vendors with a BH module.
A horizontal EHR with a behavioral health add-on and a purpose-built behavioral health EHR platform will demo similarly for thirty minutes. The difference shows up at quarter-end, when the BH-specific platform reports CCBHC and APP Plus measures without manual abstraction and the horizontal platform’s “BH module” turns out to be a notes template. Ask each vendor to produce a sample QRDA-III file from their behavioral health workflow, with real measure logic.
If you’re still building your shortlist, our side-by-side comparisons of the top behavioral health EHR platforms and top mental health EHR platforms in 2026 are a useful starting point. If billing is the dominant pain point in your evaluation, see also our breakdown of the features every behavioral health EHR billing system needs in 2026 .
The questions most organizations don’t ask until it’s too late
These are the questions that separate a good evaluation from a regrettable contract.
“What is your update process when CMS changes eCQM specifications, and what does it cost?” The right answer: Automatic, included in subscription, deployed within 30 days. The wrong answer: Professional services engagement, or “we’ll send you the updated specification files to configure.”
“Is your quality reporting capability native to the EHR, or does it require a third-party integration?” The right answer: Native, with measure logic residing in the core platform. The wrong answer: A third-party quality analytics vendor connected via integration — even if it’s described as “seamless.”
“Can I see the FHIR R4 ONC certification documentation?” The right answer: Immediate provision of ONC certification. The wrong answer: “We’re in the process of certification” or “We support FHIR through our API layer.”
“How does your platform handle multi-location quality reporting for an organization with 5–10 sites?” The right answer: Centralized quality dashboards with site-level drill-down, unified measure calculations across locations, single submission workflow. The wrong answer: Per-site configurations that require separate management, or quality reporting aggregated manually from site-level exports.
“What happens to our quality data if we decide to leave your platform?” The right answer: Full data portability in standard formats, no exit barriers. The wrong answer: Data export fees, proprietary formats, or vague answers about data ownership.
“Show me a quality measure that failed — how does the platform surface that failure and what does the intervention workflow look like?” The right answer: A live demonstration of a care gap surfaced in the dashboard, with click-through to the patient-level record and a clear workflow for care coordinator follow-up. The wrong answer: Inability to demonstrate this in the live environment, or redirection to a sample data environment.
Bring this guide's framework to a working demo with blueBriX
If you’re in an MSSP ACO or evaluating ACO LEAD for January 2027, the next step should be a working session where the framework in this guide becomes the agenda. Book a 45-minute demo with our team. We’ll walk through the seven capabilities, the MSSP/LEAD-specific items, and the six demo asks detailed above on a live environment. Bring your evaluation checklist, your shortlist context, and the questions your quality and finance teams want answered. You’ll leave with a clearer view of whether blueBriX fits and a sharper checklist either way.
Schedule a demo