

Working across Medicare, Medicaid, commercial plans, ACO contracts, and employer programs means your teams are not managing one definition of care coordination. They are managing several at the same time, each with its own expectations, file formats, timelines, and performance logic. Even when the patient and clinical workflow are the same, every payer slices the work differently.
Inside your day-to-day operations, this shows up as overlapping and competing requirements. A single patient may qualify for multiple programs, and each one asks for a different version of the same activity. One payer wants proof of outreach attempts. Another expects documentation of care transitions. Someone else requires detailed SDOH assessments, risk scoring, or chronic condition follow up. Your coordinators document an interaction once, but reporting teams must interpret it three different ways based on program rules.
These inconsistencies ripple into documentation standards, timelines, and submission rhythms. Some payers want monthly files, others quarterly or annual submissions, and many expect near real time updates. One portal is used for encounter data, another for assessments, and another for quality measures. Attribution rules rarely match, so your teams spend time verifying who belongs in each program before they can even start reporting on what happened.
The burden becomes heavier once you factor in mismatched definitions. What counts as timely engagement, what qualifies as a completed assessment, or even how an outreach attempt is logged varies from payer to payer. The work itself does not change, but the interpretation of that work does. As a result, coordinators and analysts shift between systems, reformat information, update templates, and reconcile data long after the care is delivered.
This is the part that rarely appears in dashboards but is felt everywhere across the organization. Small variations in requirements create large amounts of manual work. Authorization processes differ by payer, claim formats follow their own rules, and documentation expectations never align perfectly. Over time, this creates friction that drains staff energy and slows down both care delivery and reporting.
This is the operational reality of multi-program care. The challenge is not simply understanding multiple programs. The challenge is managing the collision points between them and translating the same care activity into several reporting languages without overwhelming your teams.
The eight challenges care teams run into every single day
Working with multiple payers and programs creates pressure that shows up in predictable ways. These challenges are not technical glitches. They are everyday barriers that slow teams down and make accurate reporting harder than it should be.
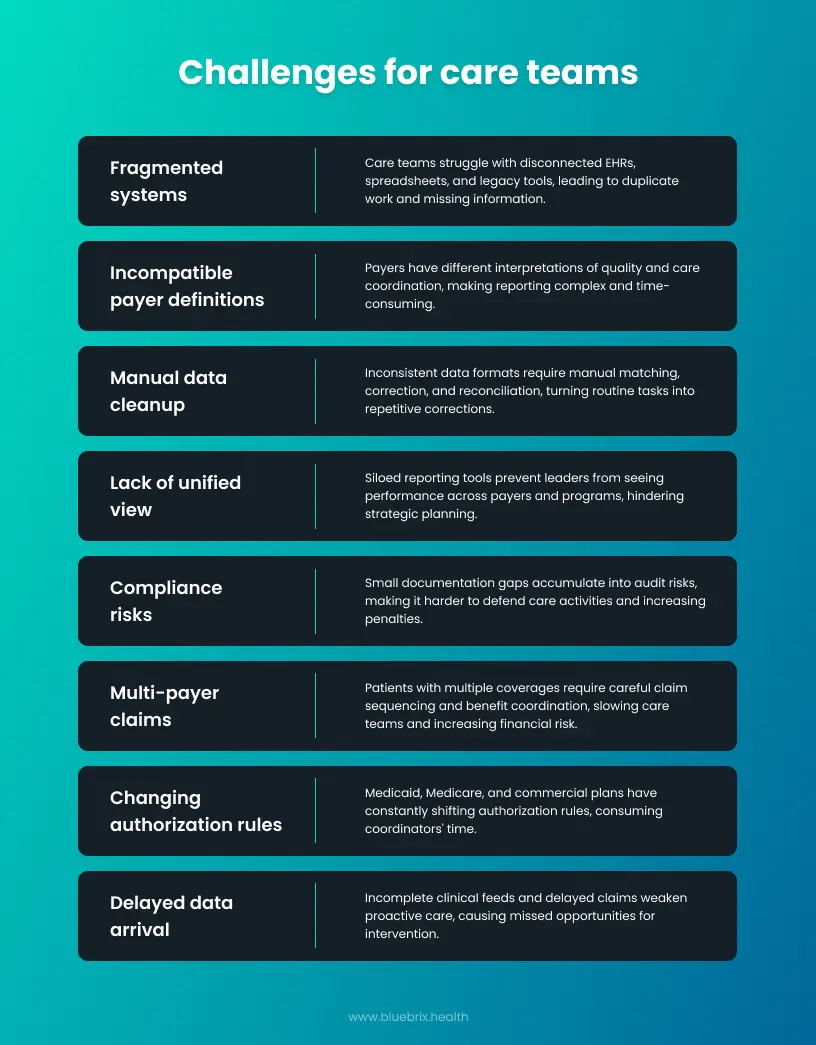
1. Fragmented systems create fragmented stories
Care teams move between several EHRs, spreadsheets, portals, and legacy tools that do not speak to each other. Each system captures data differently, which breaks the continuity of the patient record. The result is duplicate work, missing information, and delays that make reliable reporting difficult.
2. Payers define success in incompatible ways
Every payer brings a different interpretation of quality and care coordination. Some rely on HEDIS. Others follow state rules, eCQMs, MIPS logic, or proprietary definitions. When one patient population must be measured against several expectations, reporting logic becomes tangled and time consuming.
3. Manual cleanup becomes a full time responsibility
Data arrives in inconsistent formats and at different levels of completeness. Someone on the team ends up matching encounters, correcting codes, and reconciling claims. Work that should be routine becomes a cycle of spreadsheet corrections and repeat submissions.
4. No single view exists across programs
When reporting tools operate in silos, leaders cannot see performance across payers or compare how programs are functioning. Without a unified view, it is difficult to identify strengths, bottlenecks, or areas where resources need to shift. Strategic planning becomes guesswork.
5. Compliance risks accumulate quietly
Small gaps such as missing signatures, incomplete assessments, unclear timestamps, or coding inconsistencies become audit risks over time. If documentation does not align with each payer’s expectations, it becomes harder to defend care activities, which increases the likelihood of penalties or payment adjustments.
6. Multi-payer claims introduce extra layers of complexity
Patients who have more than one coverage require careful sequencing of claims, eligibility checks, and coordination of benefits. Each step comes with rules that differ across payers. When repeated at scale, this slows care teams and increases the financial risk for the organization.
7. Authorization rules change from payer to payer
Medicaid varies by state. Medicare behaves differently depending on traditional or Advantage coverage. Commercial plans follow their own structures. Forms, timelines, and medical necessity criteria shift constantly. Coordinators spend more time navigating authorization than helping patients.
8. Data rarely arrives when it is needed
Incomplete clinical feeds, delayed claims, and slow partner updates weaken proactive care. By the time teams receive the information required for intervention, the best moment to act may have already passed. This delays reporting and creates blind spots in care management.
How informatics actually fixes these challenges
Multi payer reporting becomes overwhelming not because teams lack skill but because the data that drives their work arrives from too many sources, follows different rules, and uses incompatible formats. Informatics serves as the structure that brings these pieces together. It standardizes clinical and administrative data, applies payer specific logic, and automates the steps that currently require hours of manual correction.
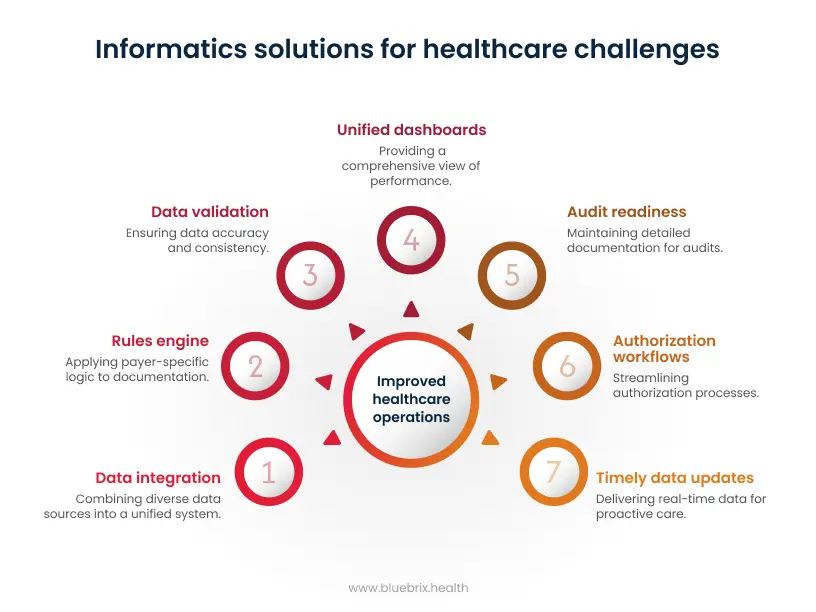
1. Creating one place for all data to live
The foundation of informatics is the ability to pull clinical, claims, social care, and operational data into a single environment. This usually involves integrations such as FHIR APIs for structured clinical data, HL7v2 feeds for hospital events, X12 transactions for claims, and SFTP transfers for payer rosters or eligibility files.
Once the data enters the system, automated pipelines remove duplicates, normalize formats, and map variation in fields such as encounter types, provider identifiers, or risk codes. This creates a consistent patient record that teams can rely on without spending hours fixing inputs from different systems.
2. Making conflicting rules work together
Different payers define measures and documentation requirements in their own ways. Informatics solves this by maintaining a separate rules engine for each program. Each engine stores logic for timelines, attribution, qualifying events, exclusions, and measure thresholds.
Once configured, the system automatically applies the correct logic to the same piece of documentation.
Example:
A coordinator records a single blood pressure reading. The informatics layer maps it to a HEDIS Controlling Blood Pressure measure for a commercial plan and simultaneously evaluates it against a Medicaid ACO’s custom eCQM requirements. The coordinator does not document the reading twice. The system interprets it for each program in the background.
3. Catching mistakes before they become problems
Manual reconciliation becomes lighter when the system performs validation at the moment data arrives. Informatics checks for missing fields, invalid codes, incorrect timestamps, and mismatches between clinical documentation and claims records.
Examples of automated validations include:
- Checking CPT and ICD code pairs against payer specific rules
- Ensuring that HIE notifications match internal EHR encounters
- Verifying that attribution rosters align with program eligibility periods
These validations prevent downstream denials, measure failures, or audit findings.
4. Giving teams a unified view across programs
With all data structured and all payer logic stored centrally, informatics generates dashboards that show performance across every contract. Leaders can compare care gaps, utilization trends, and measure status across Medicaid, Medicare, commercial plans, and specialty programs.
Because the system holds historical versions of measures, teams can also track the impact of rule changes over time without rewriting reports.
5. Keeping your organization audit ready
Audit readiness depends on having complete, consistent documentation trails. Informatics maintains timestamp level detail for every entry and stores the source and version of every data element.
This includes:
- Electronic signatures
- Assessment versions
- Changes to care plans
- Crosswalks that show how a single activity was interpreted for multiple payers
When a payer requests clarification, teams no longer scramble to piece together evidence. The system already holds an exact record of what happened.
6. Simplifying authorizations and utilization review
Authorization workflows vary by payer and program. Informatics orchestrates these steps by pre populating forms with clinical data pulled through FHIR or HL7, attaching necessary documentation, and tracking status updates in near real time.
Teams see what requests are pending, approved, or denied without checking multiple portals. This reduces delays and ensures that care is not stalled by administrative back and forth.
7. Bringing timely, complete data to your coordinators
Proactive care depends on timely updates. Informatics supports near real time data flows from hospital feeds, payer claims acknowledgments, community partner submissions, and internal care management tools.
This accelerates intervention windows and ensures reporting deadlines are met. When teams act on information sooner, both member outcomes and measure performance improve.
Implementing informatics in the real world
Once leaders understand what informatics can solve, the next question is how to put it into practice. Implementation sounds complex, but it becomes manageable when broken into predictable stages.
The first step is mapping the landscape. Every program, reporting requirement, and payer contract sits on top of specific data sources. Some systems support clinical workflows. Others handle documentation or payer files. Understanding where your data originates and how it moves highlights which integrations matter most.
The next step is building the connections that allow information to flow. This is where APIs, SFTP exchanges, HL7 feeds, FHIR endpoints, and eligibility files start moving data into one environment. These integrations give the informatics layer the raw material needed for accurate reporting and cleaner workflows.
Once data is flowing, organizations configure rules and logic. Medicare, Medicaid, commercial plans, value based programs, and state specific requirements are translated into system logic so they can be applied automatically. Teams document once, and the system interprets that work appropriately across programs.
Validation follows. Reporting teams run test submissions, compare outputs to existing processes, and confirm that payer definitions are applied correctly. This is where early adjustments are made so that go live is smooth.
Training and phased rollout come next. Coordinators learn how to document in one place. Reporting teams learn to use dashboards and alerts. Most organizations begin with two or three high impact programs and expand once the foundation is stable.
The goal of implementation is not to reinvent workflows. It is to connect them, automate payer rules, and give teams a single environment that reduces administrative pressure rather than adding to it.
Protecting data the right way in a multi payer world
Informatics is only effective if it protects the data it manages. Working with Medicare, Medicaid, commercial plans, and community partners requires consistent safeguards across every data movement. That includes encrypted storage, encrypted transmission, and role based access controls that limit what each user can view.
Security also depends on traceability. A strong informatics layer maintains audit trails for every update, signature, submission, or correction. This protects teams during reviews and reduces the friction of responding to payer questions. For sensitive behavioral health or social care data, information can be segmented so only the right roles have permission to view it.
When security is built into the workflow, staff do not need to worry about compliance on a daily basis. The platform handles the protections in the background, allowing teams to focus on coordinating care and producing accurate reports.
See how unified informatics simplifies multi-payer reporting
If you’re ready to see how it works, we can walk you through it step by step. Just reach out and we’ll set up a time that works for you.
Contact us

