

Medicare’s direction is clear. CMS continues to invest in longitudinal primary care, both by paying more accurately for complexity and by introducing options that bundle the work of “keeping a patient stable” into monthly payments.
One example is the expansion of HCPCS add-on code G2211 to additional E/M settings, which CMS describes as recognizing the inherent resources involved in longitudinal, relationship-based care. Another is the continued development of APCM services, which CMS frames as a monthly approach that removes some of the friction from time-based care management coding.
At the same time, oversight pressure is not easing. Even when a given OIG report is about a different category, the enforcement pattern is relevant to CCM and PCM: program integrity attention tends to cluster around non-face-to-face services where documentation can lag behind billing. For example, OIG’s recent reporting on remote patient monitoring highlights how Medicare oversight escalates when there are signals like weak patient relationships, thin documentation, or missing treatment management.
The practical implication for CCM and PCM in 2026 is that clinics should assume two things. First, payers will keep paying for coordinated, longitudinal care, but they will expect you to prove it. Second, the easiest way to stay out of trouble is to make your compliance process routine, not reactive
Clinical perspective: documenting the hidden work
Care coordination is reimbursement for real clinical work happening outside the visit, such as medication reconciliation and care plan updates.
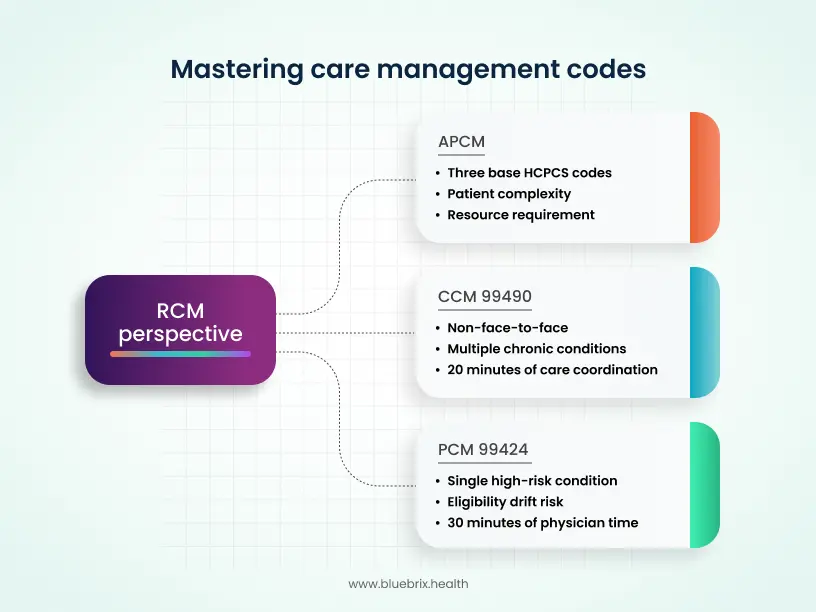
RCM perspective: mastering 99490, 99424, and the APCM monthly model
The RCM risk is rarely that the work wasn’t done; it’s that the proof is fragmented across EHR notes, call logs, and staff messages.
What does the new APCM monthly rate model mean operationally?
At a practical level, APCM shifts the focus away from tracking time and toward service eligibility and required care elements. Instead of asking “How many minutes were delivered?”, practices must ask “Are we meeting the conditions to bill?”
APCM is intended to cover advanced primary care infrastructure. CMS links eligibility to three core responsibilities: serving as the patient’s primary point of care, coordinating all needed health services, and obtaining documented patient consent. These become foundational requirements, not optional add-ons.
The new HCPCS codes we mentioned above align with existing behavioral health integration and collaborative care services and can be billed only when the APCM base code is reported by the same practitioner in the same month. This enables more integrated primary care and behavioral health models, but it also introduces additional billing dependencies.
For RCM leaders, the impact is twofold.
- Practices gain flexibility in how they design and deliver integrated care.
- Billing becomes more complex, increasing the need for precise documentation, clean workflows, and strong internal coordination.
A critical and often overlooked RCM risk here is overlapping billing exposure. The safest posture is to ensure the organization can clearly demonstrate that:
- The same work is not being billed under multiple codes or vendors, and
- Care management services are billed only when all required elements for each code family are met.
Maintaining clear directories of patient data, encounters, and care activities is essential. This is how practices avoid the two most common failure modes in APCM billing: unintentional duplication and missing audit-proof evidence.
The audit-proof strategy: using blueBriX to automate the audit trail
An audit-proof strategy is not “document more.” It is “document once, in the right places, with the right logic, and make it retrievable.”
Unified workflow matters because CCM and PCM evidence is naturally distributed. Consent might be captured in intake, time logs might live in a care management module, and care plan updates might be in a clinician note. When those artifacts are not linked, you get audit anxiety and revenue leakage at the same time.
A practical audit-proof approach has four layers.
- Structured onboarding aligns clinic values with billing protocols. That is not corporate fluff. It means clinicians and staff agree on what counts as care management work, how they document it, and what “complete” looks like before claims go out.
- Documentation templates are used sparingly and intelligently. The goal is not to force every patient into the same paragraph. The goal is to standardize the evidence points that audits look for: consent captured, care plan present and current, clinical rationale obvious, and tasks tied to patient goals.
- Time tracking is designed to be auditable. For time-based codes like 99490, the safest models capture timestamped activities, identify the staff member, and tie the activity to care plan goals. CMS’s CCM guidance makes clear that the service to-face and requires at least 20 minutes per month, so you want the record to show that threshold in a way a reviewer can follow.
- Proactively block overlap. This is where “audit-proof synergy” becomes real. If a platform can surface prior billed services for the month, highlight overlapping workflows, and reconcile encounter logs with claims, you avoid accidental double-billing and missed billing at the same time.
