The 2026 VBC landscape: New models, tighter rules, higher stakes
The value-based care ecosystem is entering a pivotal transformation phase in 2026. CMS has fundamentally restructured the risk and reward equation for healthcare organizations, making the difference between scalable and non-scalable workflows a matter of organizational survival.
The model proliferation challenge
CMS has launched three significant new VBC models for 2026, each with distinct operational requirements. The ACCESS model introduces outcome-aligned payments that reward clinical improvements across multiple chronic conditions, requiring real-time tracking of patient health trajectories. LEAD, launching in January 2027 with 2026 prep requirements, establishes 10-year benchmark commitments that demand unprecedented longitudinal care coordination. BALANCE focuses on behavioral health integration, adding mental health workflows to already complex care coordination processes. TEAM (Transforming Episode Accountability Model) shifts episode-based payments to team-based care coordination, requiring workflow integration across multiple provider types. MAHA ELEVATE expands Medicare Advantage value-based arrangements with enhanced quality measures and utilization management requirements.
For organizations managing multiple contracts, this means your workflow infrastructure must simultaneously support fundamentally different payment methodologies, quality measures, and reporting cadences. A workflow model designed for traditional MSSP operations simply cannot flex to accommodate these new requirements without significant re-architecture.
The downside risk acceleration
Perhaps more significant than new model launches is CMS’s acceleration of downside risk requirements in the MSSP program. Starting in 2026, ACOs can remain in upside-only tracks for a maximum of five years before mandatory transition to two-sided risk arrangements. This compressed timeline means organizations that previously had breathing room to build capability must now scale their care management infrastructure rapidly while simultaneously preparing for financial risk exposure.
This policy shift changes the scalability equation entirely. You’re no longer scaling just for efficiency—you’re scaling to protect against millions in potential losses. Every care gap, every missed intervention, every delayed quality measure closure now carries direct financial consequences. Your workflow model must identify risks proactively, not reactively.
ACO REACH recalibration
For organizations in the ACO REACH program, 2026 brings stricter risk score caps and revised benchmark adjustment methodologies. These changes directly impact how care management workflows must prioritize patients and allocate resources. The new risk score caps mean organizations can no longer rely solely on comprehensive coding capture; instead, workflows must balance documentation accuracy with actual care delivery improvements that demonstrate value.
The benchmark adjustments create regional variation in performance expectations, requiring workflow models that can adapt stratification and intervention thresholds based on local market dynamics rather than applying one-size-fits-all approaches.
The scalability imperative crystalized
These simultaneous policy changes create an environment where workflow scalability isn’t a competitive advantage, it’s table stakes. Organizations must now operate multiple VBC models concurrently, manage accelerated risk timelines, and adapt to evolving benchmarks and caps, all while maintaining operational efficiency, provider satisfaction, patient satisfaction, and clinical outcomes.
The question is no longer “Should we invest in scalable workflows?” but rather “How quickly can we implement workflows that scale across this new complexity before it overwhelms our operations?”
The scalability imperative in VBC workflows
Understanding what workflow scalability truly means is the first step toward evaluating your current infrastructure. It’s not simply about handling more patients—it’s about managing multiple dimensions of growth simultaneously.
Dimension one: Volume scalability
Volume scalability seems straightforward—your workflows should handle 50,000 attributed lives as efficiently as 5,000. But volume introduces non-linear complexity. At 5,000 lives, a care coordinator can manually review high-risk patient lists daily. At 50,000 lives, that same process requires intelligence and automation to surface the right patients at the right time.
More critically, volume scalability affects intervention effectiveness. A manual outreach process that achieves 40% contact rates at small scale often degrades to 15% at high volume because staff cannot maintain the same level of personalized engagement. Scalable workflows compensate through intelligent segmentation, automated prioritization, and timing optimization that maintains effectiveness even as volume grows.
Dimension two: Complexity scalability
Complexity scalability addresses your ability to manage increasingly sophisticated care scenarios without proportional increases in administrative overhead. Consider the trajectory of a typical VBC organization: you start with basic diabetes care management, add hypertension protocols, layer in behavioral health screening, integrate social determinants assessments, and eventually manage patients with 5+ chronic conditions requiring coordinated interventions across multiple specialists.
Each added layer of clinical complexity multiplies workflow complexity. A non-scalable workflow requires building separate processes for each clinical scenario. A scalable workflow uses configurable logic that applies consistent care orchestration principles regardless of clinical complexity, adapting intervention intensity and coordination requirements based on patient-specific factors.
Dimension three: Variability scalability
Variability scalability—often overlooked—determines whether you can operate multiple distinct VBC models simultaneously within a unified workflow infrastructure. This becomes critical in 2026 as organizations manage MSSP contracts alongside REACH agreements, Medicare Advantage plans, and potentially ACCESS or LEAD participation.
Each model has different attribution methodologies, quality measure sets, benchmark calculations, and reporting requirements. Non-scalable workflows require separate systems or extensive customization for each model, creating data silos and duplicating administrative effort. Scalable workflows abstract common care management functions while accommodating model-specific requirements through configuration rather than custom development.
Dimension four: Security and compliance scalability
Security and compliance represent the often-invisible fourth dimension of scalability. As your VBC operations grow, you’re not just managing more patients—you’re managing more PHI touchpoints, more user access requirements, more third-party data sharing agreements, and more regulatory reporting obligations.
A workflow that manually tracks business associate agreements and consent preferences might suffice when you’re working with three partner organizations. At scale, when you’re coordinating care across 50+ provider practices, 20+ specialist groups, and 10+ community service organizations, manual compliance management becomes impossible. Security incidents increase, audit findings multiply, and you’re constantly at risk of regulatory penalties.
Scalable workflows embed security and compliance controls directly into the process flow. Role-based access happens automatically based on care team assignments. Data sharing follows predefined governance rules. Audit logs capture complete workflow lineage without requiring additional staff effort.
Understanding these dimensions is essential, but how do you actually distinguish a scalable workflow from a rigid one? Six architectural differences reveal the answer.
What truly sets apart scalable workflows from rigid workflows in VBC
Now that we’ve established what scalability means across multiple dimensions, let’s examine the specific architectural differences that separate workflows capable of adapting to 2026’s demands from those that will struggle under the weight of new requirements.
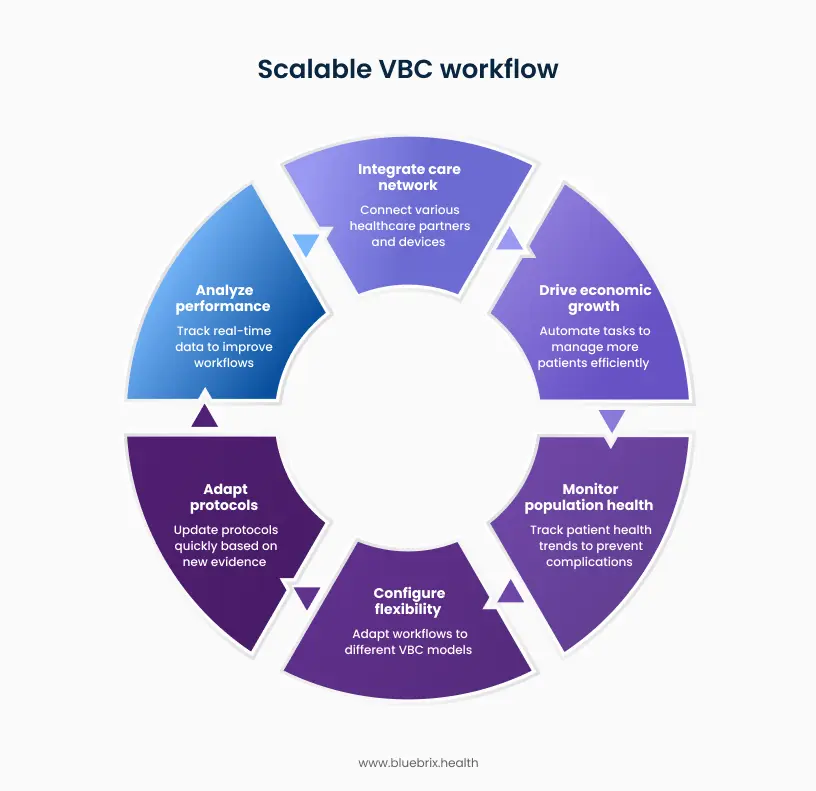
Seamless care network integration
VBC success depends on coordinating care across specialist partnerships, remote patient monitoring programs, health information exchanges, community-based organizations, and social service providers. Scalable workflows are built on API-first architecture using standardized data exchange protocols (FHIR, HL7). New care partners, monitoring devices, and information sources integrate through configuration rather than custom development. Clinical data flows bidirectionally: specialist findings update care plans automatically, RPM alerts trigger care coordinator interventions, social service referrals close the loop on outcomes.
Without this foundation, each new integration requires custom interface development, creating data silos where critical patient information doesn’t flow between systems. Specialist visit outcomes remain invisible to primary care teams. RPM data sits isolated in vendor platforms.
Economic volume growth
Growth is necessary for VBC sustainability, but only if margins remain viable. Scalable workflows use intelligent automation to handle routine processes: prior authorization submissions, appointment reminders, care gap notifications, quality measure tracking, and standard patient outreach. The same care management team effectively manages 3-5x more patients by focusing human effort on complex cases requiring clinical judgment while automation handles high-volume routine tasks.
When workflows can’t automate, administrative overhead scales linearly with patient volume. Double your attributed lives, double your care coordination staff. Growth erodes margins rather than enhancing them.
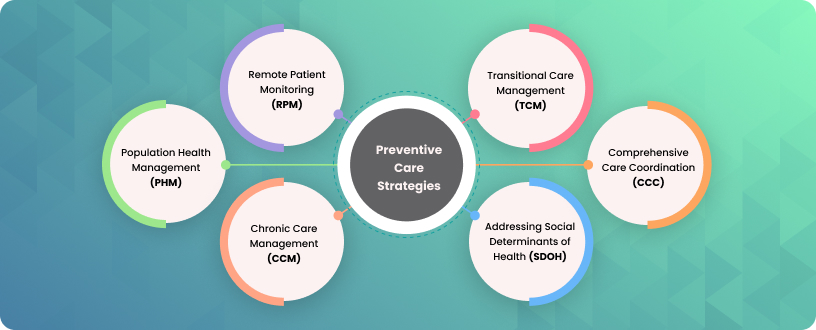
Proactive population health surveillance
VBC payment models reward preventing complications rather than treating them. Scalable workflows monitor patients between encounters and trigger interventions when patterns indicate emerging risk. Diabetic patient shows declining glucose control trends, outreach happens before hyperglycemic crisis. CHF patient’s home scale readings indicate fluid retention, intervention occurs before ER visit. The workflow starting point shifts from the examination room to the patient’s daily life.
Traditional encounter-based workflows initiate only when patients present for care: office visits, emergency department encounters, hospital admissions. Care coordination happens after clinical events occur, missing prevention opportunities.
Multi-model configuration flexibility
Organizations manage MSSP contracts alongside ACO REACH agreements, Medicare Advantage plans, and emerging models like ACCESS or LEAD simultaneously. Scalable workflows use modular architecture where core care management functions (risk stratification, care planning, intervention delivery, outcome tracking) are model-agnostic and reusable. Model-specific parameters are configurable rather than hard-coded. The same patient attributed to multiple models receives coordinated interventions addressing all applicable requirements without duplicate outreach.
Without this modularity, organizations either build separate systems for each VBC model (creating data fragmentation and reconciliation nightmares) or force a single workflow across all models (serving none optimally).
Rapid protocol adaptation
CMS updates quality measure specifications annually. New clinical evidence modifies treatment protocols. Organizational priorities shift based on performance data. Scalable workflows separate business rules from technical implementation. Operations teams modify intervention protocols, care gap definitions, stratification thresholds, task routing, and escalation logic through administrative interfaces without coding. Changes deploy within days. New protocols pilot with patient subsets before organization-wide rollout.
When business logic is embedded in application code, every modification requires IT work orders, development sprints, quality assurance testing, and staged deployment—8-12 weeks from request to production. Organizations accumulate change backlogs, operating with outdated protocols.
Real-time performance intelligence
VBC success requires understanding what’s working and replicating it immediately. Scalable workflows embed real-time performance analytics throughout execution. Continuous tracking of intervention effectiveness, care coordinator productivity, patient engagement patterns, and clinical outcome trends. A/B testing capabilities allow controlled comparison of workflow variations. Successful approaches replicate across teams immediately. Performance degradation triggers alerts while there’s still time for corrective action.
Periodic retrospective reporting shows where you’ve been, not where you’re heading. By the time underperformance appears in monthly or quarterly reports, you’ve already missed the measurement period.
These architectural differences define what separates theory from practice. Now let’s examine how blueBriX delivers these capabilities in a platform built specifically for VBC operations.
blueBriX: The practical engine for scalable care
To move from a rigid workflow to a scalable one, you need a platform that doesn’t require you to “rip and replace” your existing systems. blueBriX acts as a modular overlay that simplifies complex care delivery.
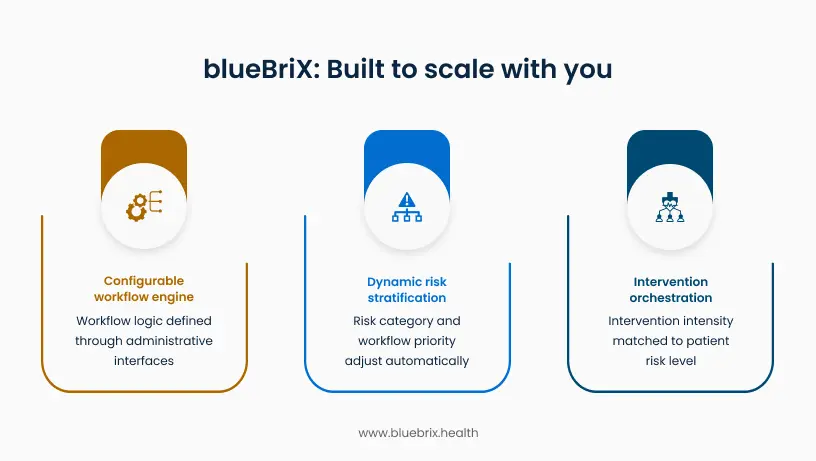
Configurable workflow logic: Adapting without development cycles
blueBriX’s configuration-based workflow engine separates business rules from technical code. Clinical operations teams define care logic through administrative interfaces without writing code. When a new VBC contract requires SDOH screening for specific patient populations, you configure the screening requirement, define which patient cohorts it applies to, set the completion timeline, and specify what happens if the screening isn’t completed. The workflow activates immediately.
Practical Impact: Organizations managing multiple payer contracts with different requirements run distinct workflow logic for each contract within a single platform. A patient attributed to MSSP follows one set of quality measure protocols. The same patient enrolled in an ACCESS pilot follows additional outcome tracking protocols. Care coordinators see both requirements in one interface without experiencing the underlying complexity.
Dynamic risk stratification: Continuous priority adjustment
Risk stratification processes data in real-time rather than in periodic batches. When a patient’s status changes (hospital admission, missed appointment, concerning lab result), their risk category and workflow priority adjust automatically. The platform supports multiple risk scoring methodologies simultaneously. Organizations using HCC-based risk adjustment for Medicare patients, ACG scores for commercial populations, and custom internal models for specific programs can run all three concurrently. Each methodology informs different workflow decisions without requiring manual reconciliation.
Practical Impact: Care coordinators don’t spend time manually reviewing patient lists and deciding who needs attention today. The system surfaces the right patients at the right time based on current data. A patient discharged from the hospital this morning appears at the top of the priority list this afternoon, not in next month’s report. This automated prioritization allows care managers to focus entirely on patient interaction rather than administrative triage.
Intervention orchestration: Matching intensity to need
The platform matches intervention intensity to patient risk level and engagement patterns, orchestrating the next appropriate action based on multiple factors: clinical urgency, quality measure deadlines, prior response history, and available resources. For a low-risk patient with good engagement history, the system might trigger automated appointment reminders via their preferred channel (text message). For a high-risk patient recently discharged from the hospital, it initiates care coordinator outreach within 24 hours, schedules a follow-up visit, and monitors whether the patient fills discharge medications. If automated outreach fails repeatedly, the workflow escalates to more intensive intervention methods.
Practical Impact: Care teams allocate human effort where it creates the most value. Nurses and care coordinators focus on complex, high-risk patients requiring clinical judgment and relationship-based support. Automated workflows handle routine reminders, appointment confirmations, and standard educational outreach. This resource optimization allows the same clinical team to effectively manage patient panels 3-5x larger than traditional manual coordination models support.
Enterprise technology foundation
Intelligent workflows need solid infrastructure underneath. blueBriX operates as a cloud-agnostic layer that connects your existing systems without replacing them.
Interoperability that actually works
Your EHR stays. We just make it talk to everything else. Native FHIR and HL7 support means data flows both ways. Close a care gap in blueBriX, and the update syncs back to your EHR automatically. One source of truth, no duplicate entry.
Security that scales with you
Zero Trust architecture with SOC 2 Type II and HIPAA compliance built into the platform. When you expand to new states or add new care models, the security foundation is already in place. No additional audits or compliance hurdles.
Uptime you can depend on
When your system goes down, care stops. That’s not acceptable when you’re coordinating care for thousands of patients across multiple locations. blueBriX is built for reliability, delivering 99.9% platform uptime, so clinicians and patients have consistent, predictable access when it matters most.
15+ years of proven healthcare expertise
Technology alone doesn’t create successful VBC programs. Experience does. blueBriX’s 15+ years of evolution alongside the healthcare industry’s most significant transformations provides the institutional knowledge that makes implementation successful rather than just technically functional.
blueBriX has matured alongside the industry’s most significant shifts, evolving from early digitization efforts to today’s complex Value-Based Care and Medicare Advantage models. This history is embedded in the platform’s architecture, providing a foundation that naturally understands the nuances of modern clinical and reimbursement workflows.
Expertise across versatile healthcare settings
Our long journey across the US healthcare landscape has defined the blueBriX DNA, refining the platform within demanding environments like pediatric behavioral health, specialty sleep medicine, and global insurance networks. This experience has produced a library of pre-built “clinical bricks” designed to navigate the specific regulatory and operational complexities of any care model, ensuring the technology adapts seamlessly to the clinical setting.
Technological leverage and quantifiable outcomes
Our clients across the US have leveraged these workflows to achieve sustainable growth without proportional increases in overhead. By automating high-value decisions, specialty clinics have realized a 52% revenue increase with 23% fewer encounters, while behavioral health providers successfully scaled their user base by 175% through 83% faster claim processing. This transition allows clinical teams to reduce time spent navigating data by 45–60%, redirecting those critical hours back into direct patient care.
Unmatched global scale and speed
blueBriX has proven that enterprise-level transformation does not have to take years. In one large-scale international deployment, we digitized 30 primary health centers in just 15 days, cutting patient history access time by 80%. Today, blueBriX supports over 2 million patients across 350+ clinics globally, utilizing a modular architecture that delivers measurable ROI in weeks rather than months.
“The global nature of our work necessitated we look for a malleable solution that will adapt to the needs and regulations of various countries, We can now build clinical workflows to fit our exact needs, no matter the specialty of care or the language requirement.”
– Jim Slack
Vice President, Sanford Health
If you'd like to explore how blueBriX fits your specific environment,
We’re here to have that conversation. Connect with our team today!
Connect with our team today