

EMR and EHR are often used interchangeably, largely because both systems handle digital patient records and support everyday clinical tasks like documentation and scheduling. Vendor marketing has further blurred the line, turning “EHR” into a catch-all label even when a system still behaves like a traditional EMR.
This overlap makes the difference feel minor. But it is not. An EMR typically keeps patient data inside one organization, while an EHR is designed to share information across providers and support coordinated care. When leaders assume every “EHR” is interoperable, they risk selecting systems that limit scalability, reinforce data silos, and fall short of today’s care delivery and reporting expectations.
A simple way to cut through the jargon is to focus on behavior, not labels: can the system exchange structured data with hospitals, labs, and specialists without custom work? If not, it effectively functions as an EMR.
Let us start with understanding what an EHR actually is.
What is an EHR? (Electronic health record explained simply)
An EHR is a digital version of a patient’s entire health history that is designed to move with them across doctors, hospitals, labs, pharmacies, and care settings. Like an EMR, it stores diagnoses, medications, allergies, lab results, imaging, immunizations, and visit notes. The difference is intent. An EHR is built to be shared securely among multiple providers and organizations, so every authorized clinician can see the same up-to-date picture of the patient at the point of care. In short, an EHR is a patient-centric, shareable digital health record meant to support coordinated, longitudinal care across the care continuum.
What an EHR is?
Think of an EHR as a connected record rather than a clinic-bound chart. It pulls together information from primary care, specialists, hospitals, labs, and pharmacies into one continuously updated timeline. The goal is to give clinicians a complete view of the patient’s history, not just what happened during the most recent visit. This allows care teams to make decisions using a broader context, instead of relying on fragmented snapshots from separate systems.
How an EHR differs from an EMR?
A helpful way to think about it: An EMR is a digital chart for one practice. And an EHR is that chart plus the ability to exchange data across the care continuum. In practice, the term “EHR” is often used to describe systems that support interoperability, population health tools, and patient access portals, not just internal documentation. That interoperability is what transforms isolated records into a shared source of truth.
How EHRs support longitudinal and patient-centered care?
Because EHRs aggregate data from many encounters over time, they enable care models that go beyond single visits.
- Longitudinal view of the patient: EHRs collect information from multiple providers into a single, chronologically ordered record. Clinicians can see trends in vitals, labs, medications, and diagnoses over years, not just days or weeks. This makes it easier to spot patterns like gradually rising blood pressure or repeated emergency visits and intervene earlier, rather than reacting only to isolated episodes.
- Patient-centered decision-making: Many EHRs include patient goals, preferences, and social determinants of health, helping clinicians tailor care plans to real-life circumstances. Patient portals also give individuals access to their records, test results, and messages, supporting shared decision-making and self-management of chronic conditions.
- Coordinated care across settings: Because EHRs are designed to share structured data across organizations, discharge summaries, specialist notes, and test results can flow directly into the primary-care record. This reduces information gaps during transitions of care. Care-management tools help teams track referrals, follow-ups, and preventive services, keeping treatment plans consistent as patients move between providers.
- Data-driven prevention and risk stratification: Longitudinal EHR data feeds predictive models that flag high-risk patients for proactive outreach. Clinicians can monitor adherence, complications, and outcomes over time, adjusting care plans based on evolving needs instead of single encounters.
Together, these capabilities turn fragmented visits into a continuous health narrative. EHR platforms like blueBriX are designed around this longitudinal model. By unifying clinical documentation, care plans, referrals, and outcomes in one system, they reduce fragmentation and support sustained engagement across physical and behavioral health settings.
Built-in data exchange: how EHRs connect providers?
A defining feature of EHRs is their ability to automatically share and receive patient information without relying on printing, faxing, or manual re-entry.
This typically happens through:
- Standards-based interfaces, such as HL7 and FHIR, which allow one system’s lab result, medication list, or discharge summary to be understood by another system.
- Health information exchanges (HIEs) and national networks, which act as a switchboard so hospitals, clinics, and labs can exchange data without building one-off connections with every partner.
Modern EHR platforms designed for multi-site and behavioral health integration, such as blueBriX, build these standards into their core architecture rather than treating interoperability as an add-on. This allows organizations to exchange discharge summaries, lab data, and referral information in near real time without relying on custom interface projects.
What usually moves through these connections includes:
- Clinical documents like discharge summaries and referral notes
- Lab results, imaging reports, and real-time event alerts such as admissions or ED visits
For providers, this means fewer information gaps and less administrative work. Instead of chasing records, clinicians can pull in data directly from connected partners and focus on care. Built-in exchange turns an EHR from a single-site chart into a connected node in a broader healthcare network.
Real-world example: coordinated primary and behavioral healthcare
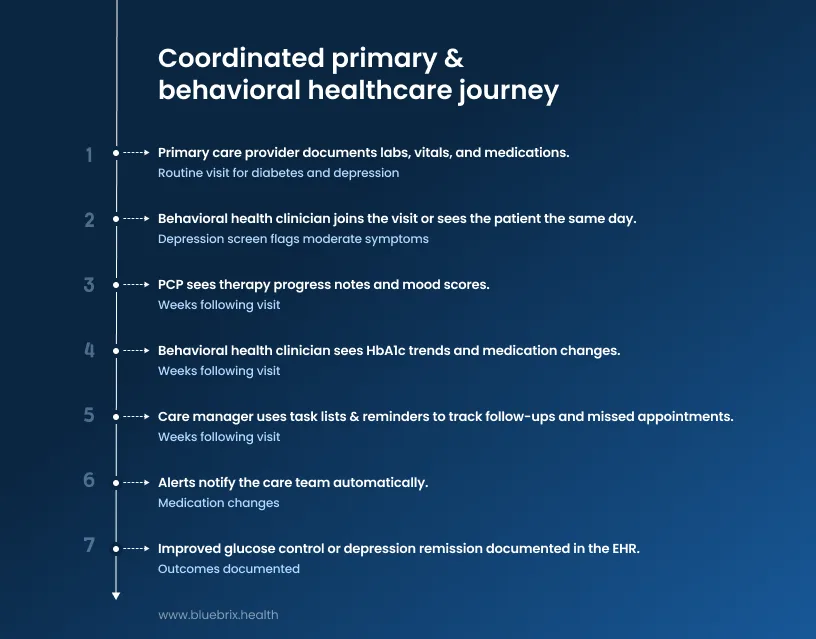
Imagine a primary care clinic that shares an EHR with an embedded behavioral-health team. A patient with diabetes and depression comes in for a routine visit. The primary-care provider documents labs, vitals, and medications in the EHR. Because both teams use the same system, the behavioral-health clinician immediately sees the updated record without waiting for a fax or separate note.
During the visit, a depression screen flags moderate symptoms. The behavioral-health clinician joins the visit or sees the patient the same day. Together, they create a shared treatment plan directly in the EHR.
Over the following weeks:
- The PCP sees therapy progress notes and mood scores.
- The behavioral-health clinician sees HbA1c trends and medication changes.
- A care manager uses task lists and reminders to track follow-ups and missed appointments.
If medications change, alerts notify the care team automatically. Outcomes like improved glucose control or depression remission are documented in one place that everyone can access.
In this setup, the shared EHR turns multiple clinicians into a single, coordinated care unit, reducing repetition, reconciling medications automatically, and keeping everyone aligned around the same plan.
Next, let us see what an EMR actually is, how it works, and where its limitations begin.
What is an EMR? (Electronic medical record explained simply)
At its simplest, an EMR is the digital version of a patient’s paper chart inside one doctor’s office or hospital. It contains the same information you would traditionally find in a physical folder: diagnoses, medications, allergies, lab results, vitals, and visit notes. The difference is that everything lives on a computer instead of in filing cabinets.
The key point is scope. An EMR is mainly designed for use within a single practice or facility. It helps clinicians in that organization document care, manage workflows, and run day-to-day operations. It is not inherently built to follow the patient across multiple providers. In short, an EMR is a digital chart for one organization, focused on documenting and managing care inside that setting.
What an EMR is?
Think of an EMR as your practice’s internal system of record. It allows clinicians to:
- Record structured and free-text clinical notes
- Maintain problem lists, diagnoses, and treatment plans
- Store medications, allergies, immunizations, and vital signs
- View lab and imaging results
- Track visit histories over time
All of this lives in one centralized system so staff can quickly pull up a patient record during appointments. For most clinics, the EMR becomes the place where “everything happens” from a clinical documentation standpoint.
What an EMR is not?
An EMR is not automatically shared with outside organizations. Unlike an EHR, it typically does not move with the patient across hospitals, specialists, labs, or community providers. The data usually stays inside the walls of that one practice unless teams manually export, fax, or build custom interfaces. This is one of the most important distinctions to understand early: EMRs are designed around internal workflows, not network-wide care.
Typical EMR features
Modern EMRs usually bundle several core functions into one practice-level system.
- Clinical notes and patient records: EMRs support both structured templates and free-text notes for visits, procedures, and progress tracking. They maintain problem lists, diagnoses, treatment plans, medications, allergies, immunizations, and vitals in a single patient profile. Many also allow clinicians to view lab and imaging results through connected systems.
- Scheduling and workflow: Most EMRs include appointment calendars, check-in and check-out workflows, and task lists for staff. Front-desk teams can book visits, send reminders, and link appointments directly to patient charts so clinicians see the right record as soon as a patient arrives.
- Internal billing and revenue support: EMRs often capture diagnoses and procedures during documentation, which feeds into coding and charge capture. Many support basic billing workflows such as claim creation and edits, sometimes integrated with or connected to a separate practice management system.
- Additional common capabilities: These typically include e-prescribing, basic clinical decision support like drug interaction alerts, and reporting tools for productivity and quality metrics.
Taken together, a typical EMR combines clinical notes, scheduling, and internal billing workflows into one system focused on what happens inside a single organization.
Real-world example: a small clinic moving from paper to EMR
Imagine a single-provider family medicine clinic that once relied on paper charts, handwritten appointment books, and separate billing forms.
Before adopting an EMR:
- Patient records lived in filing cabinets
- Scheduling happened in paper calendars
- Billing required manual re-entry into separate systems
- Sharing information with labs or specialists meant faxing or mailing copies
After implementing an EMR, that same clinic operates very differently:
- The provider documents visits directly in the patient’s digital chart using templates
- Staff schedule appointments in real time and send automated reminders
- Diagnoses and procedures flow into internal billing workflows without duplicate data entry
- Medication lists and allergies are always visible during visits
For the clinic, the EMR becomes a single digital hub. Providers spend less time searching for charts, staff workflows are more streamlined, and patient information is easier to access.
But even in this improved setup, most data still stays inside the clinic.
Key limitations of EMRs in connected-care environments
EMRs work well for documenting care inside one organization. Problems arise when care needs to extend beyond that boundary.
- Poor interoperability and data silos: Many EMRs do not reliably exchange structured data with hospitals, specialists, labs, or community providers. This creates gaps during transitions of care, such as after hospital discharge, when information often arrives late or incomplete.
- Weak support for longitudinal and chronic care: EMRs are built around individual encounters. They are not designed for continuous monitoring or between-visit engagement, which means patient-generated data like home vitals or wearable metrics often lives in separate systems.
- Limited care coordination: EMRs record what happened during a visit but typically do not manage referrals, assign care-management tasks, or track accountability across organizations. Teams end up relying on emails, spreadsheets, and phone calls to coordinate care.
- Information overload and clinician burden: Long problem lists, duplicated notes, and alert fatigue can make it harder to quickly understand a patient’s situation, especially when external records do not integrate cleanly. This contributes to documentation burden and burnout.
- Vendor lock-in and integration constraints: Many EMRs offer limited APIs or closed ecosystems, making it difficult to add best-of-breed tools for analytics, care management, or patient engagement. This restricts innovation and often forces organizations into costly system replacements later.
In short, EMRs are necessary for internal documentation, but they are not sufficient for connected care. They capture data well within one setting, yet struggle with interoperability, longitudinal care, coordination workflows, and integration.
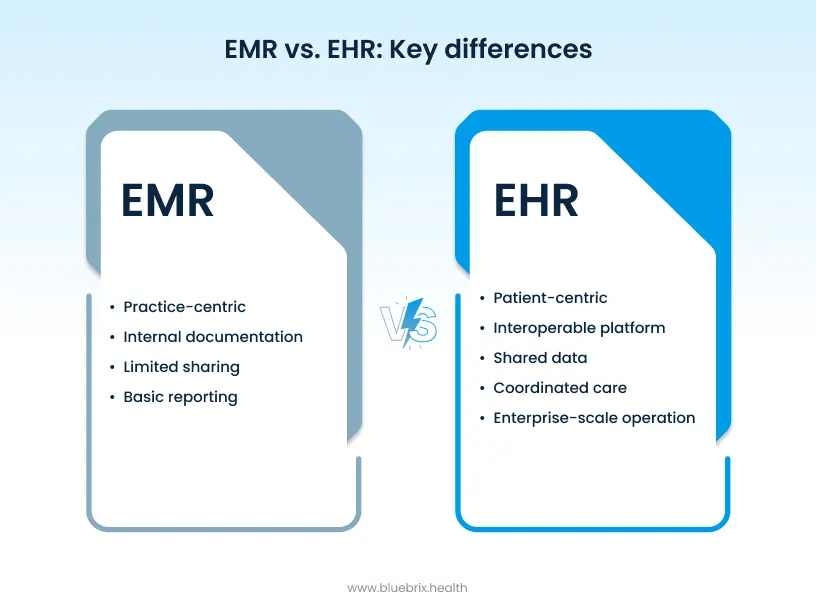
EMR vs EHR: key differences at a glance
EMRs and EHRs often look similar on the surface. Both store patient data. Both support documentation. Both help clinics run day-to-day operations. But once you look at how they handle scope, data sharing, care coordination, reporting, and growth, the differences become much clearer. Let’s break it down.
Scope of use
EMR: practice-centric records
An EMR is essentially the digital version of a paper chart inside one practice or facility. It is built around diagnosis, treatment, and internal workflows for that single organization. Think of a small primary care clinic or a standalone specialty office. The record usually does not move easily outside that setting unless someone manually exports or prints it. In other words, the EMR is centered on the practice.
EHR: patient-centric health histories
An EHR is designed to capture a longitudinal, cross-setting view of a patient’s health. It brings together information from multiple providers, hospitals, labs, and specialists. Instead of staying locked inside one clinic, the record follows the patient across time and organizations. That makes the EHR fundamentally patient-centric, not practice-centric.
Data sharing and interoperability
EMR: internal storage
EMRs are optimized for in-house use: clinical documentation, scheduling, and internal billing. Sharing data with outside entities is often manual or limited. Records may be faxed, emailed as PDFs, or printed. Most EMRs are not built around external interoperability, which makes cross-organization data exchange slow and inconsistent.
EHR: connected care networks
EHRs are designed to exchange structured data across organizations using standards such as HL7 and FHIR. These standards define how medications, labs, allergies, and diagnoses are formatted so one system can send information and another system can understand it correctly.
How HL7 and FHIR enable secure data exchange: HL7 is an older messaging standard commonly used to send clinical data like lab results between systems. FHIR is a newer, API-based standard that allows applications to query and update patient data in near real time, such as pulling the latest lab result from a hospital EHR into a specialist’s system. Both support authentication, encryption, and audit trails, so data moves securely between authorized providers instead of traveling as unsecured faxes or static PDFs.
This is what turns an EHR into part of a connected care network rather than just a digital chart.
Data ownership and patient access
EMR: provider-controlled records
In an EMR-centered model, the practice or hospital controls the record. Patients usually access their information through manual processes like requesting printed summaries or scanned documents. These records are not always current and are harder to share with other providers.
EHR: shared health information
EHRs treat the record as shared health information that multiple authorized providers can access and update. Most EHRs also offer patient portals, allowing patients to view labs, medications, visit notes, and summaries online. Many portals also support secure messaging, appointment scheduling, and bill payment. This shifts access from manual requests to ongoing digital availability.
Care coordination
EMR: standalone documentation
An EMR mainly supports documentation and workflows inside one organization. Coordination across settings (for example, primary care to specialist to hospital) is often handled through phone calls, paper referrals, and faxes. This manual approach increases the risk of delays and information gaps.
EHR: collaborative care planning
EHRs support team-based, longitudinal care by:
- Letting multiple providers view the same patient record
- Offering shared care plans, task lists, and referral tracking
- Sending alerts when key events happen, such as emergency visits or hospital discharges
This makes it easier to manage chronic conditions, handle transitions of care, and support value-based models that depend on consistent follow-up.
Reporting and compliance readiness
EMR: basic clinical tracking
EMRs typically support internal reporting like visit counts, simple quality measures, and basic dashboards. They usually lack tools for network-level analytics, risk adjustment, or value-based performance tracking across multiple providers.
EHR: quality reporting and value-based care support
EHRs are built to support regulatory and payer reporting. They aggregate data across sites and organizations, enabling:
- Population health analytics
- Risk stratification and proactive outreach
- Performance dashboards for value-based contracts
This broader reporting capability is essential for organizations participating in outcome-driven care models.
Scalability
EMR: small-practice tools
EMRs work well for single-site practices with limited interoperability needs. But they often become technical debt as organizations grow, add locations, or join larger networks, because they are not designed for multi-provider ecosystems.
EHR: enterprise-ready platforms
EHRs are designed to scale across multi-site systems and integrated delivery organizations.
They typically support:
- Multiple clinics or hospitals on one platform
- Integration with labs, imaging, payers, and health information exchanges
- Centralized governance, security, and analytics
This makes EHRs better suited for organizations planning expansion or participating in network-based care.
For healthcare leaders, the real question is not simply EMR vs EHR. It is whether the system can move data securely across providers, support coordinated care, and scale alongside the organization’s clinical network and payment-model goals. Up next, we will look at why these differences matter today, especially as healthcare shifts toward integrated care and value-based models.
Why the EMR vs EHR difference matters today
The difference between EMR and EHR matters more today than it did a decade ago because healthcare itself has changed. The industry is moving away from isolated, fee-for-service practices toward networked, value-based, and patient-centric care. In this environment, the choice between an EMR-like system and a true EHR-class platform directly affects an organization’s financial health, clinical operations, and ability to scale. What once felt like a technical nuance is now a strategic decision. Here’s why.
Value-based care and risk-sharing contracts
Payers increasingly reward outcomes, risk adjustment, and care coordination, not just volume of visits. EMR-centric systems are built around encounter-based documentation and billing. They typically lack the longitudinal, cross-provider data needed to track episodes of care, manage risk, or demonstrate performance across populations.
True EHRs are designed to aggregate data from multiple providers and settings. This enables population health analytics, risk stratification, and quality reporting, all of which are foundational for value-based contracts. When organizations confuse “EHR” with any digital chart, they risk choosing systems that look modern but cannot support shared savings, ACO-style arrangements, or risk-based reimbursement. That leaves them financially exposed as payment models evolve.
Interoperability and connected-care expectations
Patients now move fluidly between primary care, specialists, hospitals, telehealth, and community providers. Records are expected to follow the person, not stay trapped in one system. EMRs often treat data as an internal asset. Sharing still relies heavily on faxes, PDFs, or manual exports, which creates delays and information gaps during transitions of care. EHRs, by contrast, are built around standards-based interoperability (such as HL7 and FHIR) and connections to health information exchanges and national networks. Lab results, discharge summaries, and specialist notes can flow automatically into the patient record.
In today’s regulatory climate, driven by initiatives from Centers for Medicare & Medicaid Services and Office of the National Coordinator for Health IT, expectations around data sharing are tightening. Information-blocking rules, TEFCA, and patient-access mandates mean organizations relying on EMR-style silos face growing compliance risk, potential penalties, and reputational damage.
Patient expectations and digital engagement
Patients increasingly expect real-time access to their records, secure messaging, and digital tools to manage appointments, medications, and chronic conditions. EMR-centric systems usually treat patient engagement as an add-on, offering limited or bolt-on portals while keeping the core system provider-focused. Modern EHRs embed patient-facing capabilities directly into the platform, including portals, messaging, apps, and telehealth integrations. They treat patients as active participants in care, not just charts in a system. Choosing the wrong platform today can put organizations behind on patient satisfaction and retention, especially as consumers compare experiences across healthcare providers.
Workforce burnout and clinical efficiency
Clinician burnout is at crisis levels, driven in large part by fragmented workflows, manual data entry, and the constant hunt for information across disconnected systems. EMRs often require staff to re-enter data, chase faxes, and manually reconcile external records. That adds cognitive load and administrative work to already stretched care teams. Interoperable EHRs reduce this burden by automatically pulling in external results, providing unified dashboards and alerts, and supporting team-based workflows with built-in care-management tools. In the labor-constrained market, an EMR-like system that increases friction can push clinicians away. An EHR-class platform that streamlines work can help retain talent.
Scalability and network strategy
Healthcare organizations are consolidating into larger networks, ACOs, and clinically integrated systems. Technology needs to scale across sites, specialties, and care models. EMRs are often designed for single locations or single specialties. Extending them across a network usually requires expensive interfaces, workarounds, or eventual replacement. EHRs are built as enterprise-ready platforms. They support multi-site deployments, centralized governance, consistent data models, and integration with external partners. When leaders confuse EMR and EHR, they may buy a system that works for a small practice today but becomes technical debt as the organization grows.
Regulatory and policy momentum
Recent policies explicitly push healthcare toward seamless data exchange and patient-controlled records. Requirements tied to the 21st Century Cures Act, TEFCA, and information-blocking rules penalize systems that hinder data sharing. At the same time, value-based payment programs and quality measurement frameworks require structured, longitudinal data that EMR-centric systems often cannot provide. Choosing an EMR-like system under the label “EHR” can expose organizations to regulatory gaps, audit risk, and missed incentive payments.
In short, the EMR vs EHR difference matters today because modern healthcare is defined by interoperability, value-based payment, patient-centricity, and networked care. Understanding EMR as a practice-centric digital chart, and EHR as a patient-centric, interoperable platform, helps leaders choose systems that align with where healthcare is going, not where it was ten years ago.
What to look for when choosing between EMR and EHR systems
When you choose between EMR and EHR, you are really choosing between a practice-centric digital chart and a patient-centric, interoperable platform. That decision directly affects your ability to coordinate care, participate in value-based models, and scale. Here’s what matters most.
Scope of use and future strategy
Start with your growth plans.
- If you are a single-site, single-provider practice, an EMR can work for internal documentation, scheduling, and basic billing. It is usually faster to implement and cheaper upfront.
- If you plan to expand, add specialties, or connect with hospitals and referral partners, prioritize an EHR that supports longitudinal records and multi-site growth from day one.
Rule: buy for where you are going, not just where you are today.
Data sharing and interoperability
This is the biggest differentiator.
- EMR-style systems usually keep data inside one facility. Sharing often relies on faxes, PDFs, or manual exports.
- EHR-class systems are built for structured exchange using HL7 and FHIR, with connections to labs, hospitals, telehealth platforms, and health information exchanges.
Look for proof of:
- Real-time or near-real-time data flow (labs, ED alerts, discharge summaries).
- ONC-certified interoperability and TEFCA readiness, guided by expectations set by Office of the National Coordinator for Health IT.
If the vendor cannot show live exchange in reference sites, assume interoperability is limited.
Care coordination and team-based workflows
Modern care is delivered by teams.
- EMRs work well for small, single-office workflows but offer limited shared care plans or referral tracking across organizations.
- EHRs support shared care plans, task lists, alerts, and referral dashboards so PCPs, specialists, and care managers can work from the same record.
Ask vendors:
- Can multiple organizations update the same care plan?
- How are admissions, discharges, and referrals handled?
Patient engagement and access
Patients now expect digital-first experiences.
- EMRs often treat portals as add-ons.
- EHRs typically include native patient portals with access to notes, labs, medications, messaging, scheduling, and billing, plus telehealth integrations.
Look for strong patient portal adoption and clear consent management.
Reporting, compliance, and value-based readiness
Payment increasingly depends on outcomes, not visits.
- EMRs support basic practice-level reports.
- EHRs support population health, risk stratification, and quality reporting (MIPS, HEDIS), aligned with requirements from Centers for Medicare & Medicaid Services.
Ask:
- Can quality data be submitted automatically?
- Does the system support episode-based and risk-adjusted reporting?
Scalability and total cost of ownership
Think 3 to 5 years ahead.
- EMRs are cheaper initially but often become technical debt as you add locations or join networks.
- EHRs cost more upfront but are designed for multi-site operations, centralized governance, and consistent data models.
Review the vendor’s roadmap for cloud architecture, automation, and AI, and confirm they support large-system deployments.
Usability and clinician experience
Burnout matters.
- EMRs can feel simple at first but become rigid as complexity grows.
- Leading EHRs offer customizable workflows, specialty templates, and tools like ambient documentation and voice-to-text.
Ask about:
- Average time per note in real practices.
- Training and ongoing support.
Practical rule of thumb for 2026
- Choose an EMR only if you are a single-location practice with no plans to coordinate externally or grow.
- Choose an EHR if you need interoperability, patient-facing tools, value-based readiness, or scalability, which describes most organizations today.
Bottom line: anchor your decision in your network strategy, not just your current size. If you expect to share data, join an ACO, or move toward risk-based care, an EHR-class system is almost always the safer long-term choice.
Even with clear criteria, many organizations still end up with systems that don’t match their strategy. That usually isn’t because leaders ignore these factors, it’s because common pitfalls creep into the decision process. Next, let’s look at the most frequent mistakes practices make when choosing between EMR and EHR platforms, and how to avoid them.
Common mistakes practices make when selecting clinical systems
Even with clear criteria, many practices still end up with systems that look good in demos but create long-term operational pain. The same mistakes show up again and again. Here are the most common ones.
- Skipping a clear needs assessment: Many teams jump straight into vendor demos without first mapping their own workflows or future goals. They don’t document how check-in, documentation, coding, and referrals work today, or how things may change with value-based contracts, telehealth, or multi-site growth. The result is often a system that is either over-engineered and expensive, or under-powered and missing critical capabilities.
Do this instead: Define must-have features upfront and rank them before speaking to vendors.
- Choosing based on price alone: It’s common to select the “cheapest” option without looking at total cost of ownership. Hidden costs include implementation, training, interfaces, per-user fees, upgrades, and productivity loss during go-live. Low-cost systems often lack interoperability or scalability, leading to costly replacements later.
Do this instead: Build a 3 to 5 year TCO model and compare vendors on long-term value, not just sticker price.
- Treating interoperability as optional: Many practices see interoperability as a nice-to-have. They choose EMR-like systems that cannot share structured data with hospitals, labs, or specialists, creating fax-driven workflows and information gaps. This becomes a serious problem when joining ACOs, HIEs, or value-based programs.
Do this instead: Ask for real-world proof of HL7/FHIR connectivity and live data exchange with external partners.
- Underestimating usability and clinician experience: Decisions are often driven by administrators or IT teams, not frontline clinicians. Poor templates, excessive clicks, and weak specialty support lead to burnout and resistance, which hurts adoption and productivity.
Do this instead: Involve physicians, nurses, and MAs in demos. Measure time per note and workflow fit, not just feature lists.
- Ignoring patient engagement: Many practices focus only on documentation and billing. They overlook patient portals, telehealth integration, reminders, and self-scheduling, even though patients increasingly expect digital access. This impacts satisfaction and retention.
Do this instead: Treat patient engagement as a core requirement. Ask vendors for real adoption metrics from reference sites.
- Overlooking scalability: Teams often buy systems that fit today’s size but not tomorrow’s strategy. A solution that works for one location may struggle with multiple sites, new specialties, or enterprise reporting, forcing expensive migrations later.
Do this instead: Map a 3 to 5 year growth plan and confirm the platform can support it.
- Underestimating implementation and training: Many assume cloud systems are easy to roll out. They cut training, skip workflow redesign, and expect staff to learn on the job. The result is errors, delays, and months of reduced productivity.
Do this instead: Plan role-based training, assign super-users, and ask vendors about average time-to-stability.
- Ignoring security, compliance, and vendor stability: Some practices focus only on features. They overlook HIPAA-grade security, audit trails, regulatory readiness, and vendor financial health, increasing long-term risk.
Do this instead: Review security documentation, support SLAs, uptime history, and customer references.
- Treating EMR or EHR as a one-time purchase: Many organizations view system selection as a project, not a platform strategy. They fail to plan for ongoing optimization, AI upgrades, or integration with analytics and care-management tools, leaving them stuck with outdated workflows.
Do this instead: Treat your clinical system as a long-term digital backbone, with a roadmap for continuous improvement.
Final thoughts: choosing a system that supports long-term growth
At this point, one thing should be clear: modern healthcare organizations need far more than digital records. Documentation alone does not support coordinated care. A standalone chart does not enable value-based performance. And a practice-centric system cannot carry an organization through network expansion, behavioral health integration, or outcome-driven reimbursement. What today’s providers actually need is a connected foundation that brings clinical care, operations, and financial workflows into one coherent environment.
A simple checkpoint for healthcare leaders
If you are evaluating your current system, ask yourself:
- Can we exchange structured data easily with external providers?
- Do behavioral health and medical teams work from the same longitudinal record?
- Can we support quality reporting and value-based programs without manual workarounds?
- Will this platform scale as we add locations, services, or care models?
If the answer to any of these is no, you may be operating on an EMR-like foundation, even if your system is labeled an EHR.
Bottom line: the EMR vs EHR decision is no longer about features. It is about whether your technology supports connected care, operational efficiency, and long-term growth. Organizations that adopt EHR-first thinking position themselves for interoperability, behavioral health integration, meaningful reporting, and scalable care delivery. Those that do not often find themselves constrained by data silos and short-term system choices.