1. The financial architecture of healthcare modernization
The contemporary healthcare landscape is defined by a transition toward value-based care (VBC), where the electronic health record (EHR) has evolved from a repository of data into the critical operational engine of the entire enterprise. For leadership, the core challenge is not simply software procurement, but the execution of a rollout that avoids exhausting years of capital reserves on a single deployment cycle.
From an executive perspective, the correct lens for evaluating a new system is not “How much does this EHR cost?” but “What is the total cost of ownership (TCO) for the operating model this EHR supports?” Configuration-first architectures shift cost control back to the organization by allowing technical leaders to assemble clinical modules without triggering the deep, bespoke engineering cycles typical of legacy systems. A major differentiator in reducing implementation of TCO is cognitive design. By aiming for a “low-click” environment, organizations can drastically reduce the training burden and the productivity dip that typically follows go-live.
The financial barrier to modernization remains significant. According to reports from the American Medical Association, large-scale hospital and health system EHR implementations routinely reach into the millions of dollars, with enterprise deployments exceeding $2 million depending on scope, customization requirements, infrastructure upgrades, training, and long-term support commitments. For enterprise health systems operating across multiple facilities, these costs often extend well beyond initial software procurement to include integration, data migration, workflow redesign, and ongoing optimization. However, for a healthcare Chief Technology Officer (CTO), the true cost is found in the long-term TCO, which encompasses four distinct layers of expenditure:
- Direct capital and subscription spend: These are the most visible costs, including licenses, cloud hosting, and required hardware upgrades.
- Professional services: These include the “below the waterline” costs for data migration, system integration, and the custom connectors often required for legacy compatibility.
- Operational impact: Revenue leakage from lost encounters and the “implementation-induced” spike in denial rates during the first 90 days of launch can be devastating to cash flow if not managed.
- Human capital: The “human tax” of clinician burnout and staff turnover that often occurs during high-friction rollouts. Training costs alone often range from $1,000 to $5,000 per staff member, but the hidden cost of lost productivity during the learning curve can be significantly higher.
2. The blueBriX way - structured implementation framework
One of the most effective ways to reduce cost is to compress the time from project kickoff to go-live. In healthcare IT, implementation is the bridge between software purchase and daily clinical utility; the longer that bridge, the more expensive every decision becomes. While traditional enterprise EHR implementations frequently run 6 to 18 months, the blueBriX modular, configuration-first architecture enables a disciplined 12-week cycle, provided governance and scope discipline are strictly enforced by the steering committee.
Implementation framework
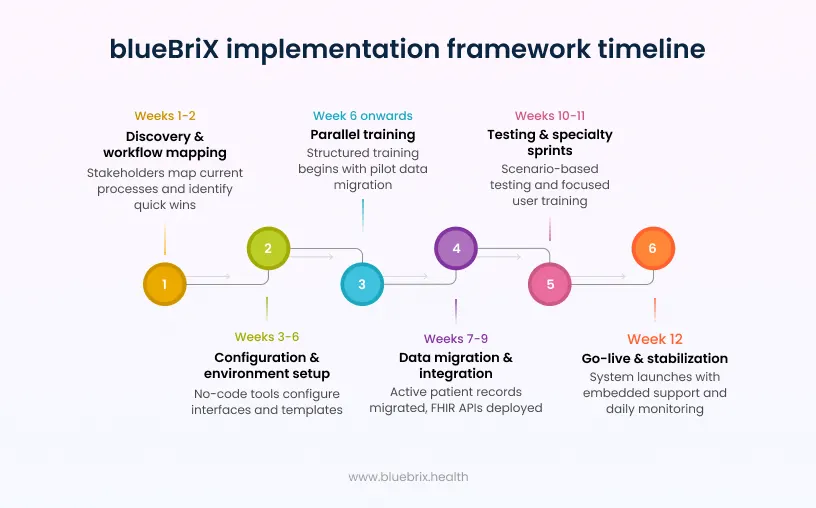
The blueBriX implementation framework prioritizes rapid configuration over custom development to achieve operational stability quickly and predictably:
- Weeks 1–2: discovery and workflow mapping:
blueBriX implementation leads work with technical, clinical, and RCM stakeholders to map current-state processes from intake to final claims. This phase identifies high-leverage “quick wins,” such as automated patient registration or eligibility checks, to demonstrate early value and secure stakeholder alignment. - Weeks 3–6: configuration and environment setup:
Using no-code configuration tools and pre-integrated modules within the platform, role-based interfaces and clinical templates are configured around real workflows. This approach minimizes reliance on expensive engineering cycles and accelerates time-to-value while preserving flexibility for future changes. - Week 6 onwards: training:
Training goes not wait for go-live. Once the environment is set up and a pilot set of data or representative sample records has been migrated into staging (from Week 6), a structured training program runs in parallel with the remaining configuration and migration work. - Weeks 7–9: data migration and integration:
The implementation team prioritizes migration of active patient records required for immediate continuity, while historical data is archived in a secure, searchable environment to reduce initial complexity and cost. Live interfaces for laboratories and pharmacies are deployed through FHIR-based APIs, reducing connector sprawl and long-term maintenance overhead. - Weeks 10–11: testing and specialty sprints:
Scenario-based testing is executed against real RCM workflows within the configured environment. Training is delivered through structured “Specialty Sprints,” a focused methodology that concentrates on the high-frequency tasks each user performs to minimize cognitive friction and accelerate productivity recovery. - Week 12: go-live and stabilization:
The system launches with embedded support from the blueBriX team. Daily operational huddles monitor throughput, user friction points, and denial backlogs, allowing rapid configuration refinement rather than triggering new development projects.
Case study: 30 clinics digitized in 15 days
The Sanford World Clinic deployment in Ghana provides a benchmark for rapid, large-scale implementation under real-world constraints. Partnering with blueBriX, SWC digitized 30 primary health centers serving more than 450,000 patients. While initial system configuration and customization required 60 days, the full rollout across all 30 heterogeneous sites was completed in just 15 days.
This acceleration was made possible by blueBriX’s configurable, modular platform architecture. Instead of deploying a monolithic system that required deep retraining, workflows were structured so that any given user could complete their responsibilities using just three role-specific screens. By limiting exposure to only the interfaces relevant to their tasks, more than 250 healthcare providers, many new to digital systems, were onboarded in a matter of hours, significantly reducing training overhead and accelerating adoption. Rather than taking years to stabilize, the modular architecture enabled rapid deployment, rapid adoption, and measurable operational gains within weeks.
3. The legacy system conundrum: breaking the technical debt cycle
The most expensive EHR is often the one already deployed. Across industries, research shows that roughly two-thirds of enterprise IT spending is allocated to maintaining existing systems rather than funding new initiatives, a dynamic that compounds technical debt through architectural rigidity, siloed integrations, and security vulnerabilities that demand costly, manual remediation. The financial stakes are high: a report found that the average healthcare data breach cost reached $10.93 million, underscoring how outdated infrastructure can materially increase financial risk.
Data migration: the hidden cost inside modernization
For organizations moving away from a legacy EHR, data migration is the most underestimated line item in the entire project budget. The risks are specific and serious: incomplete data extracts, inconsistent field formats, duplicate records, and missing transformation rules can corrupt clinical history, trigger compliance gaps, and delay go-live by weeks. blueBriX addresses this with a structured migration methodology, scoping volume and format requirements in the initial scope agreement, running data quality checks on client extracts before a single record is moved, validating all migrated data in the staging environment before any production run, and retaining a full source backup for a minimum of 90 days post go-live. For larger deployments, multiple migration dress rehearsals are run on staging to surface and resolve mapping issues well before go-live day.
Decoupling with FHIR and MCP
To exit this cycle, CTOs must migrate to open architectures built on Fast Healthcare Interoperability Resources (FHIR). Migrating to a standardized, API-driven architecture can reduce integration complexity and associated maintenance costs by a great percentage. FHIR provides the economic catalyst for this transition, using modern web standards to create a scalable foundation for data exchange.
A critical advancement for 2026 is the Model Context Protocol (MCP), an open standard that simplifies the “M x N” integration problem, where multiple legacy systems must connect to multiple different AI or analytics applications. Instead of building bespoke, point-to-point connectors for every new tool, MCP provides a standardized bridge. For a CTO, the FHIR MCP Server provides a consistent infrastructure for secure data access, allowing AI agents or decision support tools to query patient histories or lab results through a common interface. By decoupling the integration logic from the core system, MCP avoids the proliferation of expensive custom mappers and eliminates the technical debt associated with maintaining dozens of fragile connectors. This architectural simplification allows organizations to build clinical decision support systems in days instead of months.
4. Workflow-first design: resolving fragmentation and RCM challenges
A primary driver of EHR cost overruns is the “System-First” approach, where practices adapt their operations to fit a rigid software model. This misalignment leads to “shadow systems”, manual workarounds like paper notes or Excel trackers, that result in data entry errors, increased visit times, and higher denial rates. A workflow-first implementation inverts this sequence, beginning with a map of how care is truly delivered and revenue is truly collected before the system is configured.
The prior authorization “perfect storm” of 2026
Workflow-first design is especially critical for resolving the Revenue Cycle Management (RCM) challenges that often stall implementations. In 2026, the RCM landscape is defined by the CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F), which requires payers to provide near-instant responses to authorization requests, provided they are submitted through standardized, FHIR-based APIs.
Prior authorization represents one of healthcare’s most expensive administrative processes, costing the industry approximately $35 billion annually. Physicians spend an average of 16 hours per week on authorizations, with 94% reporting that these bottlenecks cause delays in patient care.
By treating clinical documentation and billing as a single continuum, automated prior authorization platforms with built-in alerts ensure that staff capture all required data during the encounter. In a complex case like cervical spine surgery, the system would prompt separate authorizations for the procedure, the implant, and post-op therapy before the service is rendered. This prevents the “prior auth predicament” where front-end errors sink back-end revenue, helping to stabilize cash flow from day one and recover the 5–15% of potential revenue typically lost to hidden leaks.
5. Modular deployment: scaling your tech stack, one "blue block" at a time
Executives should favor a modular deployment strategy over a traditional “rip and replace” model, which is often the riskiest and costliest way to modernize. The “Blue Block” strategy treats the EHR and its surrounding ecosystem as a set of interchangeable, pre-integrated components that can be introduced or retired incrementally.
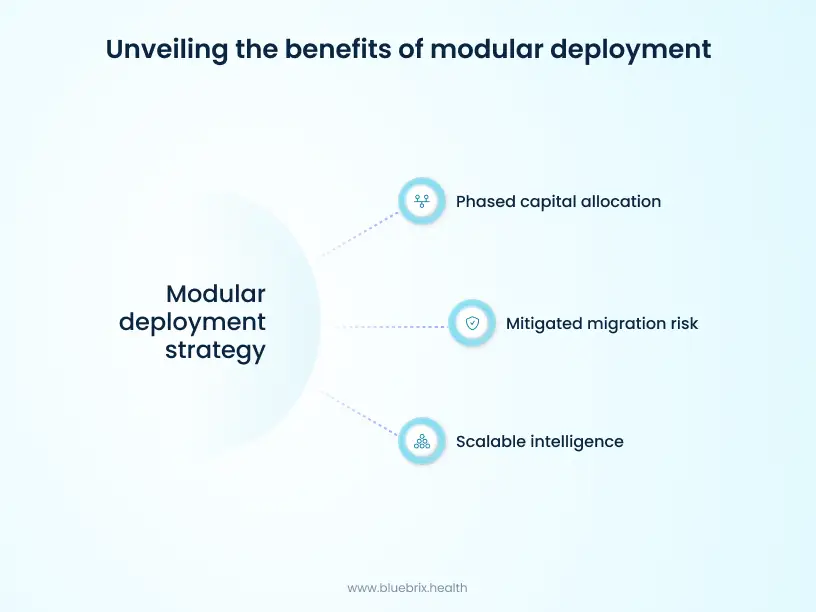
This approach offers three distinct financial advantages:
- Phased capital allocation: Organizations implement only the modules they need immediately, such as digital intake, RCM, or a specific chronic care program, and expand as execution and ROI are proven. This prevents the massive upfront investment in unused features common in monolithic systems.
- Mitigated migration risk: Teams can modernize peripheral workflows (like group therapy scheduling or population health analytics) first, allowing core legacy clinical documentation to remain stable while staff gain confidence in the new system.
- Scalable intelligence: Modular platforms utilize a dedicated intelligence engine to unify data from disparate legacy EHRs, lab systems, and wearables into a single patient profile without requiring an immediate, full-scale system replacement.
By starting with a “wedge” of high-impact functionality, executives can deliver immediate operational improvements while maintaining a manageable long-term capital trajectory and planning EHR migration steps over a longer horizon.
6. Extending value: the ROI of futureproofing with patient apps
Initial implementation costs often multiply when organizations try to add functionality like patient-facing tools after the initial go-live. A modern implementation must be built for extensions, treating extensibility as a core requirement from day one. Utilizing no-code builders allows internal teams to launch new patient experiences with minimal technical overhead and backend coding.
Case study: Vivos Therapeutics and the “extend” logic
The power of an outcome-driven platform is illustrated by Vivos Therapeutics, which acquired MyoSync, a specialist in Orofacial Myofunctional Therapy (OMT). Rather than purchasing disconnected therapy apps, Vivos utilized the blueBriX platform to develop the MyoSync App, a unified solution that connects directly to the AireO2 custom EHR.
This app is designed to help clinicians clearly track patient progress in terms of outcomes rather than just managing static records. It facilitates:
- Outcome-based progress tracking: Patients access guided therapy exercises and track their progress in real-time, providing clinicians with clear visibility into how the therapy is working.
- Therapy compliance monitoring: The app provides personalized digital tools and educational content that fosters accountability and improves adherence to OMT plans.
- Clinical oversight: Therapists use the integrated platform to monitor patient journeys throughout the treatment, ensuring that interventions are tailored to the patient’s objective progress.
From a cost perspective, the use of no-code/low-code platform allowed Vivos to launch this specialized experience with significantly reduced engineering overhead. By connecting the MyoSync therapy app directly to the existing cloud platform, Vivos optimized its capital outlay and avoided the expenses of high-cost, custom engineering while securing a foundation for scalable, outcome-driven digital health delivery.
7. Human capital: training for near-immediate productivity
Human capital costs are often the most underestimated component of EHR adoption. While training budgets may earmark a few days, the actual productivity dip can last months if the system is not designed with cognitive load in mind. blueBriX mitigates this “human tax” through a cognitive design philosophy, ensuring that approximately 90% of clinical tasks can be completed within just two screens.
Training should focus on “Specialty Sprints” – high-impact, role-specific sessions that focus on the 10–15 tasks a user performs most frequently. Anchor these sessions in real patient journeys that staff recognize, connecting system behavior to their actual responsibilities. In the SWC Ghana deployment, this simplicity allowed clinicians with minimal technical savvy to become productive with only a couple of hours of focused training. Minimizing the learning curve protects staff morale, reduces turnover risk, and preserves clinical revenue that would otherwise be lost to post-go-live friction.
8. The blueBriX implementation checklist
Technical leaders tasked with delivering a modernized EHR on time and under budget should prioritize the following tactical levers in their steering committee meetings and vendor evaluations:
- Prioritize configuration over customization: Insist that at least 80% of requirements are met via the configuration of existing “Blue Blocks” and no-code tools. Custom code should be reserved only for unique competitive differentiators.
- Architect for 2026 CMS mandates: Ensure the implementation plan includes FHIR R4 infrastructure and API gateways for the mandatory ePA and Provider Access APIs required by January 2026.
- Align RCM and clinical workflows: Build documentation templates and coding prompts as a unified continuum to prevent the first 90 days after go-live from becoming a denial spike.
- Optimize form management: Use no-code form builders to allow clinical teams to update their own forms in real-time, avoiding the thousands of dollars in vendor change fees associated with legacy systems.
- Stage risk with modular migration: Move active patient records first and archive historical data later to spread data migration costs over time and reduce go-live complexity.
- Design for low-click journeys: Enforce a “two-screen” standard for high-volume roles (like intake or triage) using journey walkthroughs and usability testing before the final cutover.
- Commit to role-based training: Budget for multiple waves of training: initial Specialty Sprints, reinforcement during stabilization, and targeted refreshers after major configuration changes.
- Scope and validate data migration before configuration begins: Agree migration volume and data format in the initial scope of agreement. Surprises at this stage are a leading cause of budget overruns. Request client data extracts at least two weeks before staging begins, and run data quality checks for completeness, format consistency, and duplicates before moving a single record. Document all field transformation rules and mappings and retain source data backups for a minimum of 90 days post go-live.
- Validate migrated data in staging before any production run: Client teams should formally sign off on data accuracy in the staging environment before the production migration run is executed. This single discipline eliminates the most common source of go-live day disruptions caused by corrupted or incomplete clinical records.
- Document and test a rollback plan before go-live: Every go-live should have a formally documented and tested rollback procedure. Knowing the exact steps to revert to the previous system state, with a clear authorization chain, transforms go-live from a high-risk event into a controlled, reversible transition. This is non-negotiable for enterprise deployments and best practice for all.
Keeping track of integrations, training, and change management
Three workstreams determine whether an implementation holds after go-live: integrations, training, and change management. In a blueBriX engagement, the Implementation Manager is the single point of contact across all three, with the PMO accountable from contract through closure.
Every integration is scoped before any build begins. A signed Integration Requirements Document defines the data flow, format, error handling, and fallback for each interface, and every integration must have a manual workaround in case it is unavailable on go-live day.
Training is a change management programme, not a one-off event. Super users are certified first and cascade to end users through role-based, scenario-based sessions. Sessions are recorded, one-page guides are provided for each role, and a sandbox environment remains available for practice after training ends.
Change management runs alongside. Staff are notified two weeks in advance, with a leadership message on what is changing and why. Change champions are identified in each department; a real-time issues channel opens on day one, and at-elbow support is on the floor for the first two days post go-live.