If you’re a clinical leader, operations manager, or practice administrator who’s ever waited on IT just to update an assessment form, this blog is for you. Maybe your patient intake process needs a small tweak. Maybe your behavioral health program added a new screening question. Or maybe your documentation workflows are evolving faster than your systems can keep up. If any of that sounds familiar, you’re not alone. This piece is for healthcare teams who want more control over their clinical workflows without adding technical complexity, and who believe clinicians should be able to adapt assessment forms as care models change.
Why clinicians still depend on IT to change assessment forms?
- In most EHR systems, assessment forms are treated as part of the core infrastructure rather than everyday clinical tools. As a result, clinicians typically cannot edit them directly, even for small changes. This is by design. EHR platforms limit who can modify forms to protect patient data, maintain reporting accuracy, and prevent changes that could disrupt connected workflows. Any update usually goes through IT-led processes that include security reviews, approvals, and testing before it reaches production.
- Many form updates also involve more than simply adding a question. They often touch structured data fields, scoring logic, reporting templates, and system integrations. Most clinicians are not trained in these technical layers, which naturally places IT in the role of gatekeeper. In addition, many vendors lock templates after implementation to avoid breaking integrations or compliance reporting, meaning even basic adjustments require technical involvement.
- Workflow governance adds another layer. Changes typically need care coordination across clinical leadership, operations, compliance, and training teams to ensure consistency and regulatory alignment, making centralized IT oversight the default approach.
In short, clinicians depend on IT not because they lack insight into what needs to change, but because traditional EHR systems are built around technical control rather than clinician-led configuration.
The hidden operational cost of delayed form updates
Delayed form updates do more than slow down workflows. They quietly drain productivity, revenue, and morale.
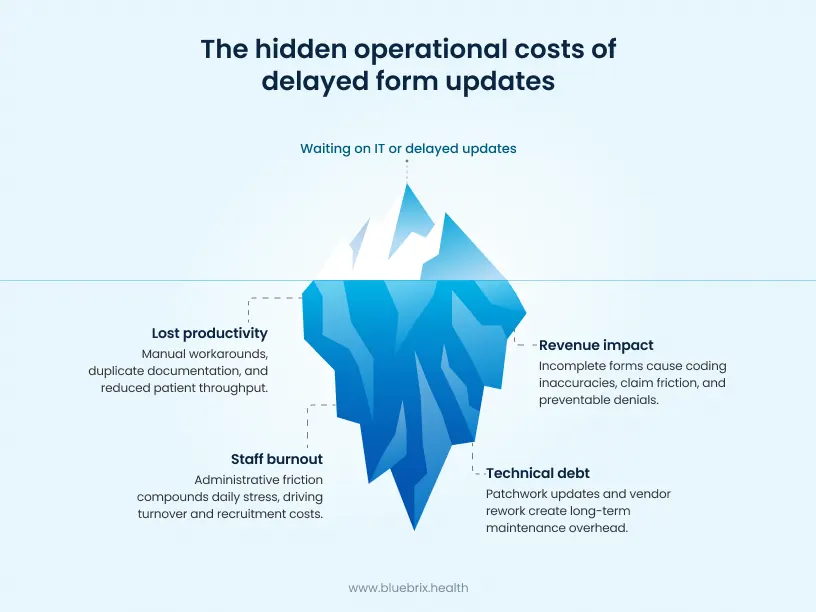
- Lost productivity: When clinicians rely on outdated forms, they compensate with manual workarounds, duplicate documentation, or follow-up clarification. That time comes directly out of billable hours and patient throughput. Even small inefficiencies compound across teams, reducing overall capacity and slowing onboarding for new staff who must learn imperfect workflows.
- Revenue impact: Incomplete or misaligned assessment forms affect coding accuracy and documentation quality. In behavioral health and other high-volume settings, this increases claim friction, reimbursement delays, and preventable denials. Inefficient intake and screening processes can also contribute to missed appointments or early patient drop-off, directly affecting revenue stability.
- Staff burnout and retention costs: Repeated dependence on IT for routine updates adds to clinician frustration. Over time, administrative friction becomes part of daily stress. In an environment already facing workforce shortages, even minor workflow barriers can contribute to dissatisfaction, turnover, and higher recruitment and training costs.
- Maintenance and rework overhead: When updates are delayed or implemented in patches, organizations accumulate technical and operational debt. Vendor-supported revisions, rework, and repeated configuration adjustments add to long-term maintenance expenses. Instead of making incremental improvements, practices may eventually face larger, more disruptive system overhauls.
These costs rarely appear on a single report. But collectively, they shape productivity, revenue performance, staff stability, compliance readiness, and long-term operational health. When policy or regulatory changes introduce new data requirements, outdated forms often force teams to manually add those data points later in reports, creating additional administrative overhead.
What no-code really means in a clinical environment?
In a clinical setting, no-code does not mean removing structure or technical safeguards. It means giving authorized clinical and administrative users the ability to configure assessment forms and workflows through visual tools, without writing software code. Instead of submitting requests to IT for every change, clinicians or designated admins can use built-in configuration interfaces to:
- Add or remove form fields
- Update assessment questions
- Adjust scoring logic
- Apply conditional rules
- Manage versions of clinical forms
- Create new assessment forms for new departments, individual providers, care programs, or policy mandates
These changes happen within the EHR platform itself, using predefined components that preserve data structure, reporting integrity, and interoperability requirements. Importantly, no-code in healthcare is not about unrestricted editing. It operates within controlled boundaries. Access is role-based, changes are tracked, and updates follow governed workflows designed to maintain consistency across clinical, operational, and reporting systems.
At its core, no-code shifts form configuration from a technical task to a clinical or administration one. It allows care teams to adapt assessment tools directly, while the underlying platform continues to enforce standards for data quality, security, and compliance.
How can providers modify assessment forms without writing code?
In no-code clinical platforms, form updates happen through built-in configuration tools designed for non-technical users. Instead of submitting IT tickets, authorized clinicians or administrators work directly inside the EHR using visual editors.
Typically, the process looks like this:
Clinicians start by opening an assessment builder or form editor within the system. From there, they can select existing templates or create new ones using predefined components such as text fields, checkboxes, dropdowns, and scoring elements.
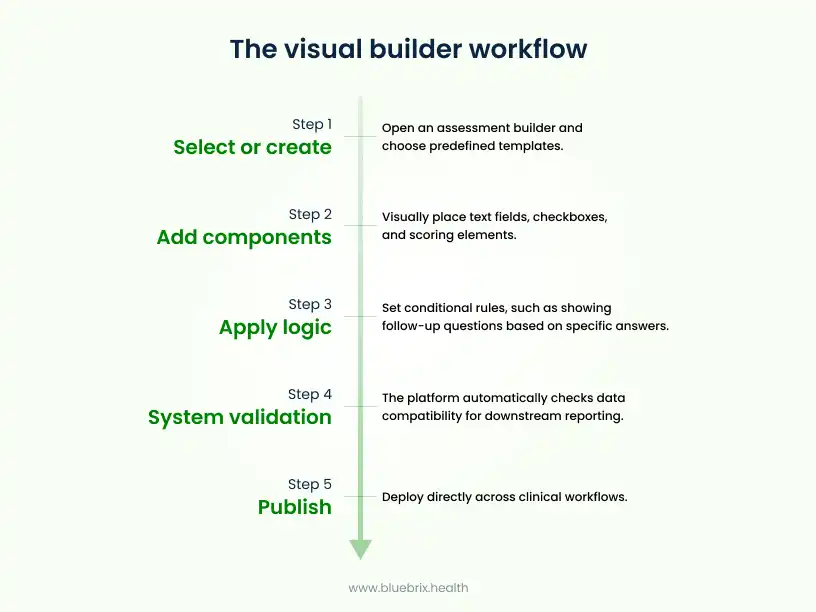
All of this is done through guided interfaces rather than code.
Once changes are made, the platform applies built-in validation to ensure data remains structured and compatible with reporting and downstream workflows. Updates can be saved as new versions, reviewed if required, and published across clinical workflows directly.
Behind the scenes, the system continues to enforce role-based access, version control, and audit tracking. This means clinicians can make meaningful updates to assessments while the platform maintains consistency, data integrity, and governance standards.
In simple terms, no-code shifts form modification from a technical task to a clinical configuration activity, allowing care teams to adapt assessment tools using familiar, visual controls instead of software development.
A real-world example of no-code form customization in action
A multi-location behavioral health organization serving veterans and first responders was struggling with fragmented assessment workflows. Standard PTSD templates captured core symptoms, but they failed to account for layered clinical realities such as moral injury, traumatic brain injury overlap, substance use comorbidities, and suicide risk escalation patterns.
Clinicians were documenting critical nuances in free text, which limited structured reporting, risk tracking, and longitudinal outcome analysis.
Using the no-code configuration capabilities the organization redesigned its assessment architecture from the ground up, without involving external developers.
Instead of creating a single static form, they engineered a modular, rules-driven assessment framework that included:
- Multi-branch conditional logic that dynamically adjusted question sets based on combat exposure type, symptom severity, and prior hospitalization history
- Embedded risk stratification algorithms that calculated composite risk scores in real time and triggered automated clinical alerts for high-risk thresholds
- Cross-form data inheritance, allowing prior assessment data to pre-populate follow-up evaluations while preserving version history
- Structured comorbidity mapping that linked trauma indicators to addiction screening modules and medication management workflows
- Built-in outcome tracking tied to DBT and trauma-focused therapy milestones
Assessment outputs were not isolated documents. They fed directly into:
- Auto-generated care plans with pre-configured intervention pathways
- Population health dashboards for program-level trend monitoring
- Payer-aligned documentation templates for value-based reporting
- Group therapy assignment logic based on risk and symptom clustering
Because the system was configured through no-code tools, clinical leads iterated on the design after a 60-day pilot. They refined moral injury scoring weights, introduced military sexual trauma branching logic, and adjusted suicide risk triggers, all without IT tickets or vendor development cycles.
Over time, the organization moved from static documentation to a living assessment ecosystem. Risk detection became proactive rather than reactive. Clinical pathways adapted to real patient data patterns. Leadership gained structured visibility into symptom trends across locations.
This is what advanced clinician-led configuration looks like: not just editing forms, but designing adaptive clinical intelligence systems that evolve alongside care models.

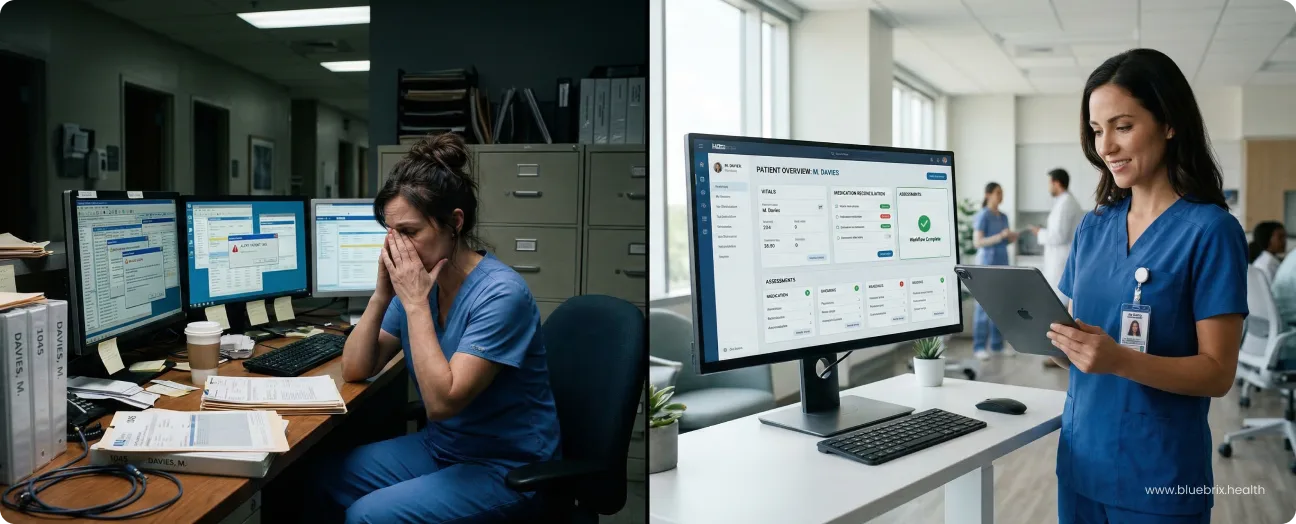
What changes when clinicians control their own workflows?
When clinicians can directly update assessment forms and workflows, the shift is immediate and practical.
- First, changes happen closer to care delivery. Instead of translating clinical needs into technical requests, teams make updates themselves at the point of insight. Assessment tools evolve alongside care protocols, not weeks later.
- Second, workflows become more consistent. Intake, documentation, and care planning stay aligned because form updates propagate across connected processes. Clinicians spend less time working around system limitations and more time using standardized, up-to-date tools.
- Third, teams gain agility. New programs, regulatory adjustments, or specialty requirements no longer require long implementation cycles. Authorized users can refine assessments as needs emerge, supporting faster iteration and smoother operational transitions.
- There’s also a noticeable impact on collaboration. Clinical, operations, and administrative teams work from the same configured workflows, reducing back-and-forth and minimizing interpretation gaps between care delivery and documentation.
Most importantly, ownership shifts back to clinical teams. Assessment forms stop feeling like fixed system artifacts and start functioning as living tools that reflect real-world practice. Clinicians regain control over how information is captured, structured, and used, without sacrificing governance or data integrity. In short, clinician-led configuration turns workflows from static processes into adaptable clinical assets.
How do clinicians make sure that changes are made without breaking workflows?
No-code in healthcare is built around controlled flexibility. While clinicians can update assessment forms themselves, those changes happen within structured boundaries designed to protect clinical workflows and data integrity.
Access is role-based, meaning only authorized users can make edits. Every change is tracked through version history, making it easy to review updates or revert if needed. This creates transparency and accountability without slowing teams down.
Form builders use predefined components that preserve structured data, ensuring updates remain compatible with reporting, billing, and downstream clinical processes. Built-in validation checks help prevent incomplete or misconfigured forms from being published.
Many platforms also support review or approval steps for sensitive changes, allowing clinical leadership or operations teams to oversee updates before they go live. This keeps documentation consistent across providers and locations while still enabling clinician-led configuration.
In short, clinicians are empowered to adapt workflows, but the system continues to enforce standards behind the scenes. Flexibility comes with guardrails, so improvements happen safely and consistently across the organization.
Who benefits most from no-code capabilities?
No-code assessment tools are especially valuable for healthcare teams that need to adapt quickly without adding technical overhead. Certain groups benefit more directly than others.

- Clinicians and frontline providers: Behavioral health clinicians often manage complex, evolving cases such as PTSD, trauma, and co-occurring conditions. No-code capabilities allow them to tailor assessments to reflect real patient realities rather than relying on rigid, generic templates. They can adjust screening logic, refine symptom tracking, and align forms with specific therapeutic models without waiting on IT. This agility reduces administrative friction, lowers burnout tied to workflow limitations, and improves productivity by keeping documentation aligned with care delivery.
- Smaller and resource-limited practices: Independent clinics and smaller behavioral health organizations often lack dedicated IT teams or development budgets. For them, no-code configuration removes the need for expensive customization projects or repeated vendor requests. Practices can deploy tailored workflows quickly, avoid long configuration cycles, and maintain interoperability without deep technical expertise. This flexibility helps them compete with larger health systems while strengthening patient throughput and revenue cycle stability in multi-payer environments.
- Care coordination and integrated care teams: In integrated behavioral health and value-based models, assessments must align with care plans, reporting requirements, and payer expectations. No-code tools support rapid adaptation to regulatory updates and evolving program requirements, allowing teams to adjust screening and documentation structures without disrupting care continuity.
- Patients, indirectly but meaningfully: When clinicians can refine assessments quickly, patient engagement improves. Intake feels smoother, documentation reflects individual needs more accurately, and care plans are built on structured, up-to-date information. Real-time insights enable more personalized treatment pathways, which can reduce early drop-offs and support better long-term outcomes.
In short, organizations that operate in fast-changing clinical environments, especially behavioral health settings and smaller practices, stand to gain the most from no-code assessment capabilities.
Why no-code form configuration matters when choosing an EHR?
When evaluating an EHR, most buyers focus on core features like documentation, scheduling, billing, and reporting. But how easily your team can adapt assessment forms over time often determines whether the system supports growth or becomes another operational bottleneck. Care models change. Regulatory requirements evolve. Programs expand. New patient populations bring new documentation needs. An EHR that requires IT tickets or vendor requests for every form update slows all of that down.
No-code form configuration shifts this dynamic. Instead of treating assessments as fixed system components, no-code EHRs allow authorized users to treat them as configurable clinical tools. This means practices can respond to change in real time, whether that’s refining intake workflows, adding specialty-specific screening questions, or adjusting documentation to meet payer or compliance needs.
From a buyer perspective, this matters because it directly affects:
- Speed to adapt: Practices can update forms as care protocols evolve, without long implementation cycles.
- Operational resilience: Teams stay productive even as workflows change, instead of waiting on external support.
- Scalability: Multi-location growth and new service lines become easier when assessments can be standardized centrally and customized locally.
- Long-term cost control: Fewer vendor dependencies and configuration projects reduce ongoing maintenance and rework.
Just as importantly, no-code capabilities signal how future-ready a platform really is. An EHR that empowers clinicians to configure assessments safely is better equipped to support value-based care, integrated behavioral health, and outcome-driven models.
Platforms like blueBriX approach this by embedding no-code configuration directly into clinical workflows, so form customization is not a separate technical process but part of everyday operations.
In short, choosing an EHR with no-code form configuration is not just about convenience. It’s about selecting a system that can evolve alongside your organization, without forcing clinical teams to slow down every time something changes.