

The EHR decision that's keeping health system leaders up at night
There’s a question that lands in the inbox of almost every CMO, clinical operations leader, or health IT director at some point: “Are we on the right EHR?”
It sounds deceptively simple. But if you’ve ever sat through a vendor demo marathon, navigated a multi-year contract renewal, or tried to reconcile what your billing team needs against what your clinical teams will actually adopt, you know it’s anything but.
The stakes have gotten considerably higher, too. With value-based care now the dominant financial framework driving CMS programs, Medicaid managed care, ACO contracts, and commercial payers, your EHR is no longer just a place to store patient records. It’s the operational backbone of how your organization proves it’s delivering quality outcomes and gets paid for it.
This guide is built for enterprise healthcare organizations evaluating EHR platforms, scaling across sites and specialties, or simply asking hard questions about whether their current system can carry them into a value-based future. We’ll cover what features actually matter at scale, how to think about pricing beyond the sticker, and why your practice size and care model should drive the decision.
Why most EHRs are still failing clinicians and what that costs you
EHRs have a reputation problem, and not without reason.
A systematic review published in JMIR Medical Informatics analyzing over 66,000 health professionals found that 40.4% reported burnout with a significantly higher likelihood among those who spent more time on EHR-related tasks outside of work hours. A separate study tracking physician faculty at a major New York academic health system found that daily clerical and after-hours EHR time actually increased between 2018 and 2022, not decreased.
The Commonwealth Fund is blunt about the cause: primary care physicians face growing administrative burden from “complex insurance rules, implementation of value-based payment, poor usability of EHR systems, and an overload of care quality measures.”
When nearly 70% of primary care physicians feel that most EHR clerical tasks they perform don’t require a trained physician, something is structurally broken in how these platforms are designed and deployed. And the costs, apart from clinician morale, are productivity, retention, and the quality of care that gets compressed when providers are focused on their screen instead of their patient.
The good news is that purpose-built, workflow-intelligent EHR platforms are closing this gap. But only if you know what to look for and what questions to ask.
What shifting EHR standards mean for your organization in 2026
If you’re a clinical or operational leader, the EHR landscape in 2026 isn’t presenting you with new opportunities so much as raising the floor on what you’re expected to deliver and the gap between where most organizations are and where payers and regulators want them to be is wider than many realize.
Here’s what actually matters for your organization right now.
The bar for interoperability has been raised and regulators are watching. The 21st Century Cures Act’s information blocking provisions are no longer just a compliance checkbox. CMS and the ONC are actively enforcing the expectation that patient data flows freely across care settings. If your EHR creates data silos whether by design or because your vendor charges to activate a standard API that’s both a regulatory exposure and a care quality problem. In 2023, only 70% of hospitals were fully participating in all four domains of interoperability, sending, receiving, finding, and integrating patient data. In a value-based care environment, that remaining 30% isn’t just technically behind. It’s financially behind, because incomplete data means incomplete quality scores, and incomplete quality scores mean leaving reimbursement on the table.
If you’re still on an on-premise EHR, your operational risk profile is growing. Cloud-based systems now account for over 84% of the ambulatory EHR market not because cloud is a trend, but because it’s the only architecture that realistically keeps pace with continuous regulatory updates, interoperability mandates, and the integration demands of value-based contracts. On-premise systems can be made to work, but the cost and effort of keeping them current compounds every year. For multi-site organizations managing multiple payer relationships, that compounding cost eventually becomes a strategic liability.
What your EHR can do should make more sense than just having an EHR. Near-universal adoption means your competitors have an EHR too. The organizations pulling ahead in value-based care contracts are the ones whose platforms actively support care gap identification, population health management, and automated quality reporting — not the ones whose EHR simply documents what already happened. The question your leadership team should be asking isn’t “Do we have an EHR?” It’s “Is our EHR generating the clinical and financial intelligence our contracts now require?”
What "enterprise" actually means in healthcare EHR terms
Enterprise doesn’t just mean large. It means operationally complex. And that complexity looks different depending on your care model, but the common threads are recognizable across specialties and settings:
- Multiple sites — sometimes across counties, states, or care models
- Mixed provider types and clinical disciplines sharing patient data
- A diverse payer mix spanning Medicare, Medicaid, commercial insurance, and self-pay
- Regulatory layers that vary by specialty, location, and program type
- Value-based care contracts that require population-level quality reporting, outcome tracking, and care coordination across the continuum
A generic, one-size-fits-all EHR rarely handles this well. And when your IT team is being charged $25,000 just to “turn on” a standard API feed — a scenario that’s far more common than it should be — you’re not working with a modern enterprise platform. You’re working with a system designed to profit from complexity rather than reduce it.
The 6 EHR features that define enterprise performance in value-based care
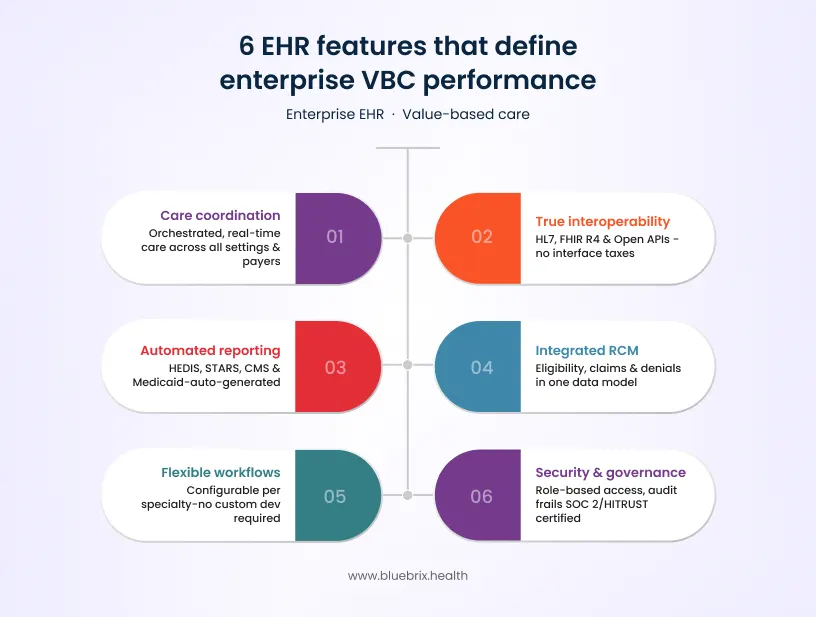
1. Care coordination that goes beyond referral management
In value-based care, completing a referral is the minimum. What your EHR needs to support is orchestrated care across disciplines, care settings, payers, and community resources — in real time.
That means multi-provider collaboration embedded in the workflow, not layered on top of it. It means a primary care physician, a specialist, a care manager, and a community health worker can all see what’s happening with a shared patient without switching platforms or relying on faxed summaries. It means care gaps get flagged before they become quality failures, not after.
Look for: centralized care coordination dashboards, referral tracking with closed-loop confirmation, cross-provider documentation visibility, patient risk stratification, and the ability to surface social determinants of health (SDoH) data alongside clinical information.
2. True interoperability: HL7, FHIR R4, and open APIs
HL7 and FHIR aren’t just acronyms — they’re the plumbing of modern healthcare data exchange. Your enterprise EHR must connect bidirectionally with Health Information Exchanges (HIEs), external EHRs across care settings, lab and imaging systems, pharmacy networks, payer portals, and state and federal reporting systems.
FHIR R4-compliant open APIs are now effectively the baseline for any serious enterprise platform. Without them, you’re building walls between your data and the clinical decisions that depend on it — and creating integration costs that compound every year.
The right question to ask any vendor: “Show me a live data exchange between your platform and an external HIE. How long does it take? Who maintains the connection when it breaks? And what does it cost to add a new integration?”
3. Automated compliance and quality reporting for VBC contracts
If your quality team is still manually pulling data from multiple systems to generate HEDIS reports, STARS measures, or payer-required quality metrics, you’re losing time and introducing the kind of human error that shows up in your quality scores and your reimbursement.
Enterprise EHRs in 2026 should include pre-built and configurable report templates for CMS quality programs, Medicaid reporting requirements, ACO performance metrics, and payer-specific contract requirements — generated automatically from clinical documentation, not manually assembled after the fact.
The goal is compliance and reporting that runs in the background, not a team of analysts scrambling at reporting deadlines.
4. Integrated revenue cycle management across payers and specialties
Billing in a multi-specialty, multi-payer enterprise environment is genuinely complex. CPT codes vary by specialty, modality, and payer contract. Prior authorization requirements differ across insurers. Telehealth billing has its own distinct coding landscape. And in value-based contracts, accurate claims aren’t just about revenue — they’re part of your quality evidence.
Your EHR and your RCM engine cannot operate as separate systems with a manual handoff between them. Look for platforms offering real-time eligibility verification, ERA/X12 claims processing, automated coding suggestions grounded in clinical documentation, denial management workflows, multi-payer contract support, and telehealth billing built natively — not added as a module.
When documentation, billing, and quality reporting run through a single data model, claims are cleaner, denials are fewer, and your financial performance reflects the care you’re actually delivering.
5. Specialty-flexible, configurable clinical workflows
One of the most common — and costly — EHR failures at enterprise scale is deploying a platform that works well for one specialty and forces every other specialty to adapt to it. Cardiologists, primary care physicians, behavioral health clinicians, surgeons, and chronic disease specialists don’t document, order, or coordinate care the same way.
An enterprise EHR worth its price should offer configurable clinical templates, documentation workflows, order sets, and care pathways that can be tailored to each specialty — without requiring extensive custom development or a dedicated IT team to maintain each configuration.
Ask for a live demo of how the platform handles two very different specialties simultaneously. The answer will tell you a lot about how “flexible” actually translates in practice.
6. Enterprise security, role-based access, and data governance
Enterprise healthcare organizations are among the most frequently targeted by ransomware and data breach attempts in any sector. HIPAA compliance is a regulatory floor — not an enterprise security strategy.
Look for granular role-based access controls so that each user sees only what they need to see, data segmentation by program, location, or care type, full audit trails for compliance and legal defensibility, and independent security certifications like SOC 2 Type II or HITRUST. Vague answers to security questions during vendor evaluation are not just red flags — they’re deal-breakers at enterprise scale.
EHR by practice size: matching platform depth to organizational reality
Small practices (1–10 providers)
The priority here is simplicity, speed, and low administrative lift. You need smart scheduling, purpose-built clinical templates, automated patient reminders that reduce no-shows, one-click billing, and built-in telehealth — without an IT team to manage any of it.
The biggest risk for small practices is choosing a platform that’s either too stripped-down (forcing workarounds that eat clinical time) or too complex (creating adoption failure before you ever see ROI). The right system should feel like it was built for your size, not scaled down from a hospital implementation.
Mid-size organizations (10–50 providers, multiple locations)
This is where interoperability stops being optional. With multiple providers coordinating care across locations, multiple payer relationships to manage, and reporting requirements from Medicaid or value-based contracts, you need a system that centralizes data without requiring manual reconciliation to hold it together.
Multi-site management, open API integrations with labs and referral networks, multi-provider workflow coordination, and automated quality reporting move from “nice to have” to operationally essential. Scalability matters too — a platform that performs well for 20 providers but breaks under the demands of 45 is a liability, not a solution.
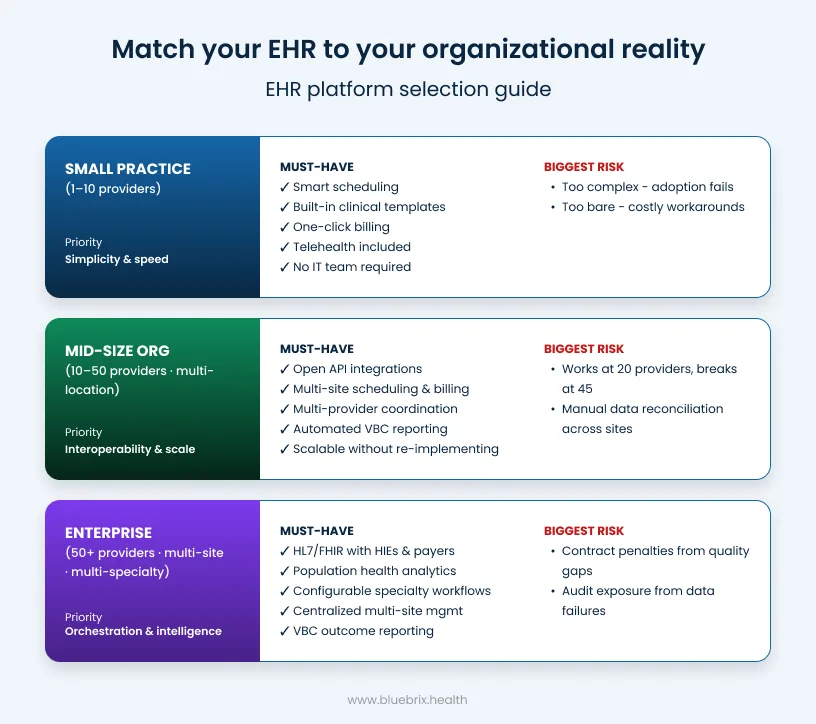
Enterprise organizations (50+ providers, multi-site, multi-specialty)
At enterprise scale, the EHR functions as a care coordination orchestration platform. It connects clinical workflows to financial performance, population health management to individual care delivery, and quality reporting to payer reimbursement — across every site, specialty, and provider type in your organization.
Requirements include HL7/FHIR interoperability with HIEs, payers, and external systems; configurable specialty workflows across multiple clinical disciplines; enterprise-grade role-based access and data governance; population health analytics and risk stratification; and outcome reporting tied directly to VBC contract performance metrics. The cost of getting this wrong at enterprise scale isn’t just operational friction — it’s contract penalties, audit exposure, and care gaps that register in your quality scores and your balance sheet.
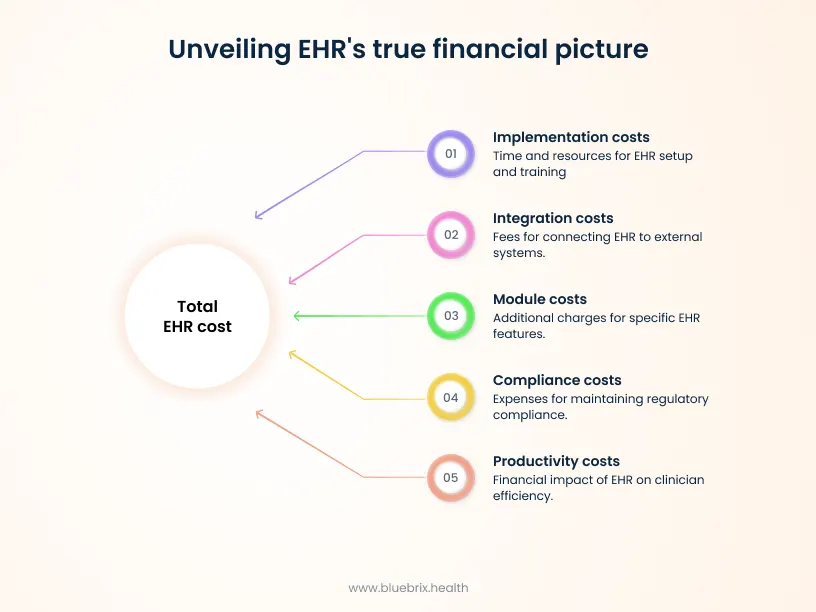
How to think about EHR pricing: total cost of ownership (TCO) over 5 years
EHR pricing is notoriously opaque, and the headline per-user monthly cost rarely reflects what organizations actually spend. Here’s how to build a more honest picture:
Implementation and onboarding: Enterprise EHR deployments can take 6–18 months and demand significant internal staff time alongside vendor support. Ask precisely what’s included in implementation, what’s billed separately, and what a realistic go-live timeline looks like for your configuration.
Integration costs: Some vendors charge substantial fees to activate standard API connections to external systems — what the industry sometimes calls “interface taxes.” At enterprise scale, these costs accumulate quickly. Platforms built on open standards with native integrations are generally far more cost-effective over a multi-year contract.
Module and feature pricing: Many EHR vendors sell a base platform and gate telehealth, ePrescribing, advanced analytics, patient engagement, and compliance reporting behind separate modules. What looks affordable at signing can expand significantly once you activate the features you actually need to operate.
Compliance and regulatory maintenance: Healthcare regulations change constantly. Who absorbs the cost of keeping your system current? Cloud-based SaaS platforms typically build this into their model. On-premise and legacy architectures often don’t — and the bill comes at the worst possible time.
Hidden productivity costs: If your providers are spending multiple hours each week on documentation tasks that a better-designed system would automate or streamline, that’s a real cost — it just doesn’t show up on the vendor invoice. The research is clear: EHR-related burnout is directly linked to clinician departure. Replacing a departing specialist can cost anywhere from $30,000 to well over $100,000 in recruiting, credentialing, and onboarding alone.
The right pricing question isn’t “what does it cost per seat?” It’s “what is the all-in cost of this platform over five years — including what we lose or gain in productivity, compliance, and care quality?”
The value-based care imperative: your EHR needs to be ready for this
CMS is expanding value-based programs across Medicare Advantage, ACOs, and specialty care. State Medicaid agencies are building performance metrics into managed care contracts across primary care, behavioral health, and specialty settings. Commercial payers are increasingly tying reimbursement to measurable outcomes rather than volume.
In this environment, an EHR that simply records what happened in a clinical encounter is not enough. Your platform needs to track population-level outcomes — not just individual encounters — flag care gaps before they become quality failures, generate payer-required performance reports automatically, and connect clinical activity to financial results within a single data model.
This is the difference between a documentation system and a care coordination orchestration platform. The former records. The latter manages, connects, and performs. In value-based care, organizations that bridge that gap will have a structural advantage. Those that don’t will feel it in their contracts.
How blueBriX approaches enterprise EHR and care coordination
blueBriX is a purpose-built integrated EHR and care coordination orchestration platform designed for healthcare organizations operating in — or transitioning toward — value-based care. It was built to be specialty-flexible from the ground up, serving primary care, multi-specialty groups, behavioral health, chronic disease management, community health, and more within a single unified architecture.
The platform brings clinical documentation, care coordination, revenue cycle management, telehealth, ePrescribing, compliance reporting, and patient engagement together into one integrated system — eliminating the fragmentation that drives up costs, creates care gaps, and burns out clinical teams.
At enterprise scale, blueBriX delivers HL7/FHIR interoperability connecting to external EHRs, HIEs, labs, PDMPs, and payer systems — without the interface taxes that drain IT budgets. Centralized scheduling, documentation, and billing across all sites and provider types operate through a single operational lens, giving leadership real visibility into performance across the entire organization.
For organizations managing value-based contracts, the platform’s care coordination orchestration capabilities mean care gaps are identified and acted on in real time, quality metrics are tracked continuously rather than assembled at reporting deadlines, and payer performance data flows from clinical documentation automatically — not from a separate analytics tool that’s always slightly out of sync.
For clinical teams, blueBriX is built around configurable, specialty-aware workflows. Whether your providers are documenting a primary care visit, a chronic care management encounter, a psychiatric evaluation, or a complex care coordination session, the system adapts to how they work — rather than forcing them to adapt to how the system was designed.
Transparent, all-inclusive pricing means the features your organization needs to operate are not hidden behind module upgrades.
10 questions to ask any enterprise EHR vendor before you sign
- How does your platform support value-based care quality reporting — natively, or through a separate reporting module?
- Can you demonstrate live, bidirectional data exchange with an HIE or external EHR system?
- What is your realistic implementation timeline for an organization of our size and complexity, and what’s included?
- How are integration costs structured? Is there a fee to connect each new external system, lab, or payer?
- How configurable are clinical workflows across different specialties or care models — and who manages that configuration?
- What does full-feature pricing look like with telehealth, ePrescribing, analytics, and compliance reporting all active?
- What security certifications do you hold — SOC 2 Type II, HITRUST, or equivalent?
- What is your roadmap for AI-assisted documentation, clinical decision support, and population health analytics?
- What does your SLA look like for uptime, and how are incidents handled during active clinical hours?
- How does your platform scale when we add providers, locations, or new specialty lines and what does that cost?


