
The cloud EHR inflection point: why this conversation matters now
Healthcare organizations moved to the cloud to gain speed, scale, and flexibility—but many leaders are discovering that daily operations still feel just as heavy. Across care models and markets, the pattern is consistent: cloud adoption solved infrastructure problems, but left core operational constraints largely unchanged.
At the same time, healthcare itself has changed. Payment models reward outcomes, care extends beyond clinical settings, and margins leave little room for inefficiency. Cloud EHRs emerged as the logical response, but hosting alone was never enough to meet these new demands.
But here is the paradox many leaders now face: the infrastructure problem has largely been solved, yet the operational problem persists.
Care teams still rely on manual coordination. Leaders still struggle to adapt workflows quickly. Data still moves slower than care demands. The disappointment is rarely voiced publicly, but it is widely felt privately.
Treating cloud EHR as a hosting decision instead of a foundational operating choice – that’s the problem.
Why cloud EHRs often disappoint after go-live
From a technical standpoint, cloud EHR migrations often succeed. Systems are stable. Access improves. IT teams spend less time managing hardware. Yet operational leaders frequently ask a troubling question months after go-live:
Why does it still feel so hard to get things done?
The answer lies in design heritage. Many cloud EHRs were originally built as monolithic systems optimized for documentation, billing, and compliance. When moved to the cloud, their core assumptions remained unchanged. Workflows stayed tightly coupled. Customization remained code-heavy. Change cycles stayed slow.
The result is what some leaders quietly call “cloud fatigue”, a sense that despite significant investment, day-to-day operations feel no more flexible than before. This explains why optimization roadmaps stretch indefinitely, why innovation feels incremental, and why transformation initiatives keep circling back to workarounds rather than breakthroughs.
At this point, most organizations reach for tactical fixes such as more training, more governance, more optimization cycles. But these efforts rarely address the real issue. The problem is not how well the system was implemented, but what the system was fundamentally designed to do.
Until leaders examine that design intent, cloud EHR disappointment tends to repeat itself, no matter how many upgrades, vendors, or cloud migrations follow.
Systems of record vs systems of action: a critical distinction
If cloud EHRs feel underwhelming after go-live, the root cause is rarely execution. It is almost always a mismatch between what leaders expect the system to do and what it was actually designed to be.
Once the system is live, this mismatch becomes visible. Leaders expect adaptability, responsiveness, and support for modern care models only to discover that cloud hosting has not changed the system’s underlying purpose.
This gap between expectation and design intent is what separates incremental improvement from real transformation. To move forward, leaders must understand the difference between systems of record and systems of action.
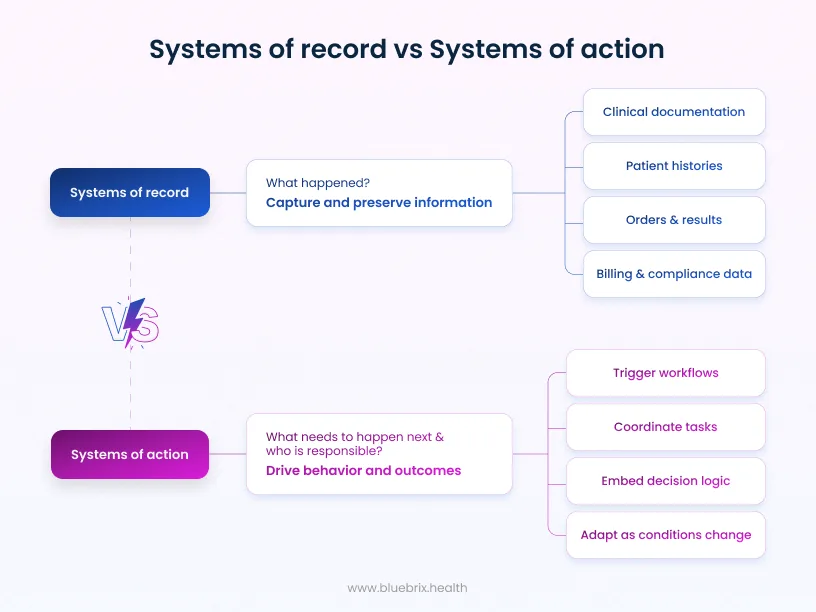
Systems of record
Systems of record are designed to capture and preserve information. In healthcare, this includes:
- Clinical documentation
- Patient histories
- Orders and results
- Billing and compliance data
These systems answer an important but limited question: What happened?
Systems of action
Systems of action are designed to drive behavior and outcomes. They:
- Trigger workflows based on events
- Coordinate tasks across people and systems
- Embed decision logic into operations
- Adapt as conditions change
They answer a different question: What needs to happen next, and who is responsible?
Modern healthcare, especially value-based, coordinated, and longitudinal care depends far more on the second question than the first. Delays in action translate directly into higher cost, poorer outcomes, and clinician burnout.
A cloud EHR that remains primarily a system of record may be compliant and reliable, but it will struggle to support modern care delivery.
This is the leadership trap: systems of record scale compliance and reporting, but they scale action only through people. Every time care teams compensate for system gaps with manual coordination, leaders are unknowingly funding operational drag.
Over time, this creates an organization that appears digitally mature on paper, yet remains strategically immobile in practice. Transformation stalls because the system was never designed to move with them.
What cloud EHRs should enable in a modern care environment
When evaluated through a system-of-action lens, Cloud EHR expectations shift dramatically.
Event-driven, continuous care
Care today unfolds continuously. Lab results, remote monitoring data, patient messages, and social determinants all generate signals. Cloud EHRs should treat these as actionable events, not passive data points.
This means workflows that automatically initiate outreach, escalate risks, or adjust care plans without waiting for the next visit or manual review.
Intelligent workflow orchestration
True orchestration goes beyond task lists. It involves routing work dynamically based on role, capacity, urgency, and context. It makes ownership visible and bottlenecks measurable.
Decision support that reduces friction
Clinicians do not need more alerts; they need fewer decisions to make under pressure. Effective cloud EHRs embed guidance directly into workflows, supporting consistent action while preserving clinical judgment.
When these capabilities are absent, organizations compensate with staffing, spreadsheets, and parallel systems, quietly eroding the value of the EHR itself.
The real advantages of cloud EHR: when architecture gets it right
When cloud EHRs are built natively for adaptability, their advantages extend well beyond IT efficiency.
Organizations gain:
- Faster configuration of workflows without code changes
- The ability to launch new care programs without platform rework
- Easier integration of third-party tools and digital health solutions
- Incremental innovation through frequent, low-disruption releases
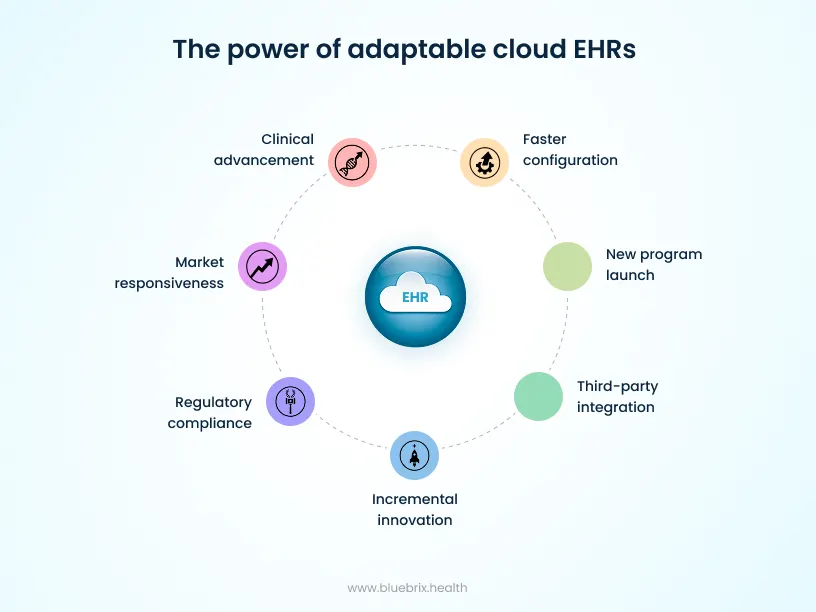
These advantages compound over time, enabling organizations to respond to regulatory changes, market pressures, and clinical innovation with far less friction.
The trade-offs leaders must confront honestly
No technology choice is without compromise, and cloud EHRs are no exception.
Workflow lock-in as the new constraint
While cloud adoption reduces infrastructure dependency, it can increase dependency on vendor-defined workflows. When care models evolve, rigid systems force organizations to adapt processes to technology rather than the reverse.
Customization vs complexity
Highly configurable systems reduce dependency but require governance. Without discipline, flexibility can introduce inconsistency. The challenge is choosing platforms that allow configuration with guardrails.
Dependency and resilience
Cloud uptime is generally high, but outages do occur. Leaders must evaluate not just reliability metrics, but transparency, recovery processes, and operational contingency planning.
Understanding these trade-offs upfront enables informed, strategic decision-making.
Cloud does not automatically mean composable
Composable architecture is often misunderstood. Beyond APIs or integrations, it is about modularity – components that can evolve independently without destabilizing the whole.
Many cloud EHRs expose APIs while retaining tightly coupled internal logic. Integration becomes possible, but orchestration remains limited. Complexity shifts outward, increasing operational burden.
True composability requires an orchestration layer that coordinates services, workflows, and data flows across the ecosystem.
The questions healthcare leaders must ask before choosing a cloud EHR
At this stage, leading organizations stop thinking in terms of vendor comparisons and start thinking in terms of operating leverage. Rather than asking what a cloud EHR can do out of the box, they focus on how the platform behaves when reality changes because it always does.
Before selecting a cloud EHR, leaders should pause the feature checklist and ask deeper questions. More importantly, they should understand why each question matters and what a strong answer actually looks like in practice.
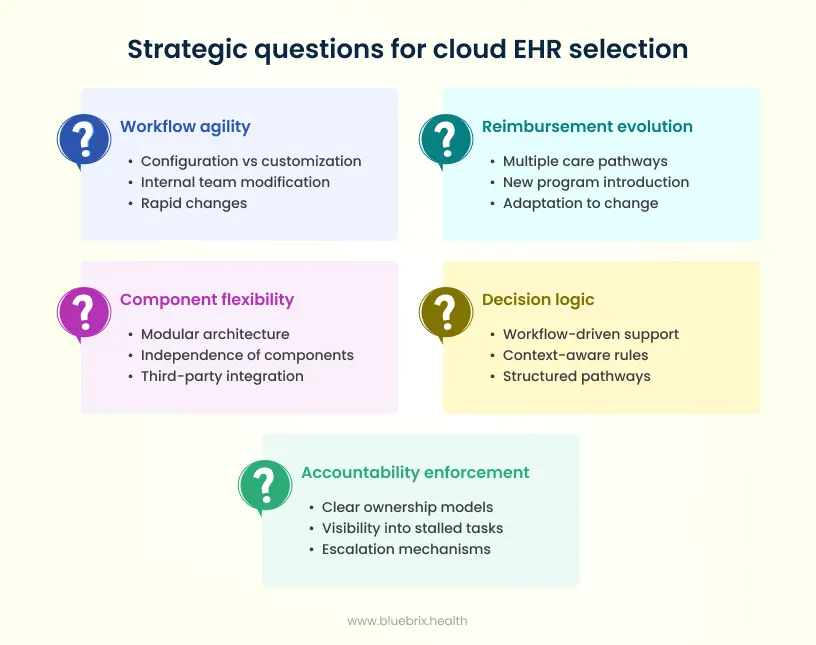
1. How quickly can workflows be changed without vendor involvement?
Care models, regulatory requirements, and operational realities change far more frequently than EHR contracts. If every workflow change requires a vendor ticket, roadmap approval, or custom development, agility disappears quickly.
What good looks like:
- Clear separation between configuration and customization
- Evidence that internal teams can modify workflows safely and repeatedly
- Real examples of changes made in days or weeks—not quarters
2. What happens when reimbursement models or care pathways evolve?
Value-based care, bundled payments, and specialty-specific pathways are still evolving. An EHR that is optimized only for today’s models becomes tomorrow’s constraint.
What good looks like:
- Support for multiple, parallel care pathways
- The ability to introduce new programs without disrupting existing ones
- Proof that the platform has adapted to real-world reimbursement change
3. Can components be replaced or extended without disrupting core operations?
No single vendor will remain best-in-class across every capability. Over time, organizations will need to integrate, swap, or extend components without destabilizing the system.
What good looks like:
- Modular architecture with clear boundaries
- Independence between core records and workflow logic
- Examples of third-party tools added without major rework
4. Where does decision logic live—inside the system or in people’s inboxes?
When decision-making relies on emails, reminders, or individual memory, consistency breaks down. This increases risk, burnout, and variability in care.
What good looks like:
- Workflow-driven decision support embedded into daily operations
- Context-aware rules that guide next-best actions
- Fewer alerts, more structured pathways
5. How is accountability enforced when processes break down?
In complex care environments, things will go wrong. The question is whether the system surfaces issues early—or hides them until outcomes suffer.
What good looks like:
- Clear ownership models within workflows
- Visibility into stalled tasks and handoffs
- Built-in escalation and reporting mechanisms
Vendors who can answer these questions clearly—and demonstrate them contractually and operationally—tend to be far stronger long-term partners than those who rely on feature lists and roadmaps.
What are the common implementation challenges of cloud EHR projects?
Cloud reduces infrastructure friction, but implementation risk remains significant.
Common failure patterns include:
- Weak governance and unclear ownership
- Translating existing workflows instead of redesigning them
- Underestimating clinician trust and change management
- Migrating data without defining its operational role
Successful organizations treat cloud EHR implementation as organizational transformation, not system replacement.
Security, compliance, and trust in a cloud-first world
Cloud security is often reduced to certifications and audit reports. While frameworks such as HIPAA, SOC 2, and HITRUST establish essential baselines, they do not, by themselves, create trust. For healthcare leaders, trust is not a legal construct—it is an operational reality experienced daily by clinicians, staff, patients, and partners.
In cloud-first environments, security follows a shared responsibility model. Vendors may secure infrastructure, but organizations remain accountable for how data is accessed, used, and acted upon across workflows. When security is treated as a layer added after workflows are designed, it inevitably becomes a source of friction.
What mature cloud EHR security looks like in practice:
- Role-based access tied to workflows, not just job titles, ensuring users see only what they need at the moment of action
- Auditability built into everyday operations, so compliance is continuous rather than episodic
- Data segmentation and least-privilege principles that reduce blast radius without slowing care
- Real-time monitoring and anomaly detection aligned to clinical and operational context
Why this matters?
Security failures in healthcare rarely stem from malicious intent alone. They more often arise from workarounds—shared logins, offline notes, duplicate systems—created when security controls make it harder to do the right thing than the fast thing.
When security is embedded directly into workflows, it reinforces trust instead of eroding it. Clinicians spend less time navigating barriers. Leaders gain confidence that compliance is being upheld in real time, not reconstructed after the fact. And organizations avoid the false trade-off between safety and speed.
In a cloud-first world, the most secure EHRs are those where security, usability, and care delivery are designed as a single system.
Measuring cloud EHR success beyond adoption metrics
Adoption is a starting point, not a finish line. Logging in, completing training, and using core features only confirm that a system is in use not that it is delivering strategic or operational value.
For cloud EHRs positioned as enablers of modern care, success must be measured by movement, adaptability, and impact, not familiarity.
Below are the dimensions healthcare leaders should evaluate and why each one matters.
1. Time-to-change (organizational agility)
What it measures:
How quickly workflows, forms, pathways, and rules can be modified when clinical, regulatory, or operational needs change.
Why this matters:
Healthcare operates in a state of near-constant change—new reimbursement models, evolving clinical guidelines, regulatory updates, and shifting patient expectations. If every change requires months of planning or vendor dependency, the organization falls behind reality.
What good looks like:
- Workflow changes executed in days or weeks, not quarters
- Minimal reliance on vendor professional services
- Clear ownership of configuration within internal teams
Time-to-change is one of the most honest indicators of whether a cloud EHR is enabling progress or quietly accumulating technical debt.
2. Care coordination velocity
What it measures:
The speed at which care transitions occur—referrals closed, follow-ups completed, gaps addressed, and handoffs resolved.
Why this matters:
In coordinated and value-based care models, delays are not neutral. They increase clinical risk, patient dissatisfaction, and cost leakage. Slow coordination often signals workflow fragmentation and poor orchestration.
What good looks like:
- Reduced referral and follow-up turnaround times
- Fewer manual escalations and reminders
- Real-time visibility into stalled or delayed tasks
Cloud EHRs that function as systems of action make coordination measurable—and improvable.
3. Reduction in manual workarounds
What it measures:
The extent to which staff rely on spreadsheets, emails, phone calls, and shadow systems to get work done.
Why this matters:
Workarounds are symptoms of system gaps. While they keep operations moving in the short term, they introduce risk, inconsistency, and burnout over time.
What good looks like:
- Declining dependence on external trackers and inboxes
- More work happening inside structured workflows
- Less institutional knowledge trapped in individuals
A cloud EHR delivering real value steadily absorbs workarounds back into the system.
4. Alignment across clinical, operational, and financial outcomes
What it measures:
Whether improvements in one area create friction or progress in another.
Why this matters:
Healthcare technology has a long history of optimizing documentation at the expense of clinicians, or revenue at the expense of care teams. Cloud EHRs should reduce these trade-offs, not reinforce them.
What good looks like:
- Clinical workflows that support accurate, timely documentation
- Operational efficiency without increased clinician burden
- Financial performance that reflects real care activity
When cloud EHRs align these dimensions, organizations stop choosing between efficiency and quality.
5. Decision latency
What it measures:
The time between a meaningful signal (clinical, operational, or patient-generated) and an appropriate action.
Why this matters:
In modern care environments, delayed decisions are costly. Whether it’s a missed risk signal or a delayed intervention, latency directly affects outcomes.
What good looks like:
- Event-driven triggers that initiate workflows automatically
- Decision support embedded where work happens
- Fewer delays caused by manual review queues
Low decision latency is a hallmark of systems designed for action, not documentation.
6. Sustainability of improvement
What it measures:
Whether gains persist after initial go-live enthusiasm fades.
Why this matters:
Many cloud EHR implementations show early improvement followed by plateau. This often indicates that the system cannot evolve alongside the organization.
What good looks like:
- Continuous optimization without major reimplementation efforts
- Steady improvement in operational metrics over time
- Confidence that the platform can support future care models
If a cloud EHR cannot sustain momentum, its strategic value will peak early—no matter how strong adoption appears.
The future of cloud EHR: from documentation to orchestration
The next generation of cloud EHRs will be:
- AI-native rather than AI-augmented
- Event-driven rather than visit-centric
- Continuously compliant rather than audit-driven
- Designed for orchestration across the care continuum
- Systems that fail to evolve in this direction will remain increasingly peripheral.
Where blueBriX fits: enabling systems of action in the real world
Throughout this guide, one theme has surfaced repeatedly: the gap between cloud-hosted EHRs and systems truly designed to enable action. This is precisely the gap blueBriX was built to address.
blueBriX is not positioned as “another cloud EHR.” It is designed as an intelligent care orchestration platform that can function as a system of action—either alongside existing EHRs or as the foundation for modern care delivery models.
How blueBriX aligns with what healthcare leaders actually need
Architecture designed for change
blueBriX emphasizes configuration over customization. Care teams and operational leaders can adapt workflows, programs, and pathways without waiting for vendor-led development cycles. This directly addresses the time-to-change constraint that limits most cloud EHRs.
Workflow orchestration as a first-class capability
Rather than treating coordination as an add-on, blueBriX embeds orchestration into the core platform. Tasks, events, escalations, and accountability are designed to move seamlessly across care teams, settings, and systems.
Composable by design
blueBriX supports modular adoption. Organizations can integrate third-party tools, extend capabilities, or modernize specific workflows without destabilizing existing environments. This allows leaders to evolve their technology stack without wholesale replacement.
Built for value-based and longitudinal care
blueBriX is optimized for care models where action between visits matters most—chronic care, population health, virtual-first programs, and coordinated care networks. Event-driven workflows, continuous engagement, and real-time visibility are foundational, not retrofitted.
Security and compliance embedded into workflows
Rather than layering controls on top of static processes, blueBriX integrates security, auditability, and role-based access directly into how work gets done—supporting continuous compliance without slowing care delivery.
In short, blueBriX operationalizes the system-of-action principles this article advocates. It does not ask organizations to choose between stability and adaptability—it is designed to support both.


