

You already know value-based care is hard. This is about why your execution isn’t matching your strategy and what to do about it.
Your quality scores aren’t moving. Your care managers are busy, but care gaps aren’t closing. Your physicians are frustrated. Your payer is starting to ask harder questions. And somehow, despite months of work and real investment, your VBC program feels like it’s running in place.
Most leaders in this position look for the problem in the wrong places the contract terms, the EHR, the patient population, the physicians who “just don’t get it.” These are real friction points, but they rarely explain why a well-resourced program with genuine clinical commitment still underperforms.
The real culprit, in our experience, is almost always the same: the infrastructure holding the program together is too weak for the complexity of the work. Not the strategy. Not the intent. The execution infrastructure governance, accountability, visibility, and change management.
If you’ve already diagnosed that something is wrong with how your program runs, this piece is for you. Not to confirm the problem, but to give you a framework for fixing it.
Five signs your program management is holding you back
Weak program management rarely announces itself. It hides in busyness, in optimistic status reports, in the belief that more effort will eventually break through. These are the patterns worth looking for honestly.
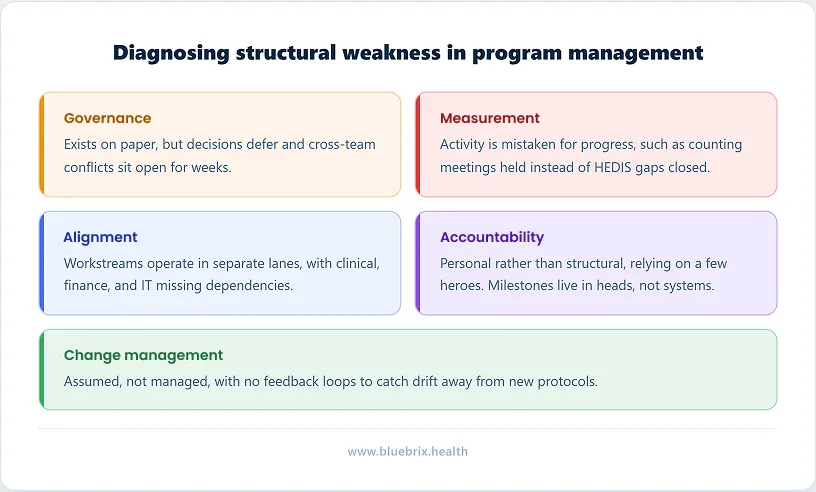
- Governance exists on paper, not in practice: Your steering committee meets, but decisions get deferred. When a workstream conflict surfaces say, IT prioritization versus clinical deployment timelines there’s no clear authority to resolve it. Issues that should take 72 hours to close sit open for weeks.
- Activity is being mistaken for progress: Status reports are full of meetings held, trainings completed, and workflows designed. But when you ask directly how many high-risk patients received a care management touchpoint last month? what is our HEDIS gap closure rate this quarter? no one can answer cleanly. The program measures effort, not outcomes.
- Workstreams operate in separate lanes: Clinical makes decisions about care protocols without knowing the EHR workflow implications. Finance models risk exposure without input from care management on patient outreach capacity. Misalignments aren’t discovered until they’ve already created rework, delay, or cost and no one is mapping dependencies between teams.
- Accountability is personal, not structural: One or two people hold the program together through sheer effort and institutional knowledge. If they left tomorrow, the program would stall. Milestones are owned in someone’s head, not in a system. When targets are missed, the response is a conversation not a formal corrective action with re-baselining and revised ownership.
- Change management is assumed, not managed: New care protocols are deployed and clinicians are trained. But six months later, workflow adherence is inconsistent, care managers have reverted to old habits, and the promised behavior change hasn’t materialized. No one measured adoption. No feedback loop caught the drift. Implementation was treated as the finish line, when it was only the starting line.
If two or more of these patterns feel familiar, the gap isn’t in your clinical model or your contracts. It’s in how the program is being run.
How weak program management erodes your VBC strategy?
Value-based care is built on a simple but demanding premise: deliver measurably better care at lower cost, and get paid accordingly. Every component of that equation depends on program management working at a high level. When it doesn’t, the damage compounds across several dimensions.
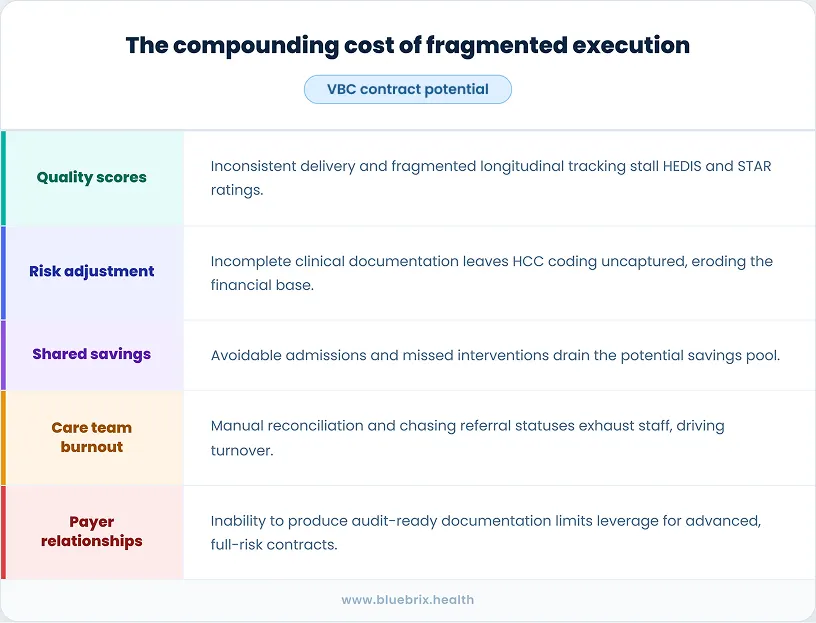
- Quality scores suffer: VBC contracts are tied to performance on quality measures — HEDIS gaps, STARS ratings, MIPS scores, chronic condition metrics. These scores depend on care being delivered consistently, documented accurately, and tracked longitudinally. Weak program management breaks each of those requirements.
- Risk adjustment erodes: Accurate risk adjustment whether HCC coding in Medicare Advantage or PMPM rate-setting in other models requires complete, current clinical documentation tied to active care programs. When program management is weak, documentation is inconsistent and risk scores go uncaptured. Organizations end up getting paid for a healthier population than the one they’re actually managing, eroding the financial foundation of the VBC model.
- Shared savings evaporate: In shared savings models, every avoidable admission, every duplicated test, every missed preventive intervention represents a cost that comes out of your potential savings pool. Strong program management prevents these leakages by ensuring high-risk patients are identified early, enrolled proactively, and managed with the right level of intensity. Weak program management lets those leakages accumulate quietly, consistently, and expensively.
- Care teams burn out: The administrative burden of navigating fragmented programs is exhausting. When coordinators spend hours tracking down referral statuses, reconciling duplicate records, or manually chasing down open care gaps, they have less time for the patient interactions that actually drive outcomes. Turnover rises. Morale falls. And the organization finds itself hiring more staff to compensate for system inefficiency rather than investing in care capacity.
- Payer relationships weaken: Payers evaluating your performance don’t just look at final quality scores. They look at the operational rigor behind them. Can you demonstrate consistent program execution? Can you produce audit-ready documentation? Can you show outcome trends across specific patient cohorts? Weak program management makes all of this difficult to demonstrate, which weakens your negotiating position and limits your ability to take on more advanced, full-risk contracts.
The root cause: managing programs without the right infrastructure
Many clinics attempt to run sophisticated VBC programs on infrastructure that was never designed for it. Legacy EHRs built for fee-for-service documentation, bolted-on care management tools that don’t communicate with billing systems, and spreadsheet-based tracking that breaks down as soon as volume increases were used.
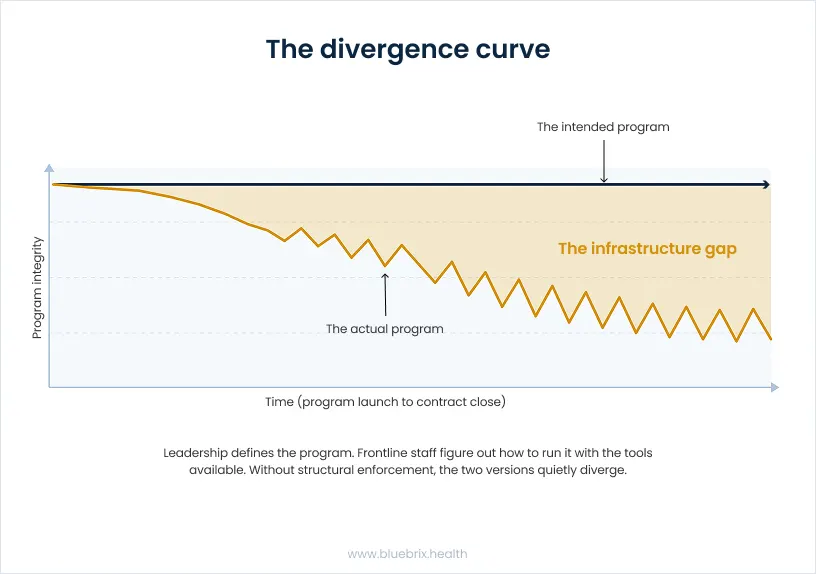
The result is a constant gap between program design and program execution. Leadership defines what a program should look like. Frontline staff figure out how to run it with the tools available. And the two versions of the program, the intended and the actual quietly diverge over time.
This isn’t a people problem. It’s an infrastructure problem. And the answer isn’t more training or more staff. It’s a purpose-built program management engine that makes the right way to run a program the easiest way to run it.
How blueBriX fixes your program management foundation
blueBriX is built from the ground up for value-based care, and program management is one of its core design principles.

A configurable program management engine
At the center of the blueBriX platform is a purpose-built program management engine that allows organizations to define, configure, and govern care programs with clinical and operational precision. You can set explicit rules for patient inclusion and exclusion based on clinical criteria, payer contracts, CPT codes, provider type, and more. Programs are not ad hoc constructs — they are structured entities with defined enrollment logic, billing strategies, care team assignments, and referral rules built in from the start.
Standardized, program-driven treatment plans
blueBriX embeds care pathways directly into the workflow. Standardized, program-driven treatment plans ensure that care is delivered consistently, tracked longitudinally, and adapted as patient needs evolve. Clinical protocols aren’t stored in a binder — they’re built into the platform so that the care team is guided through the right steps at the right time, regardless of who is on shift or how long they’ve been with the organization.
A unified care team workbench
One of the most damaging aspects of weak program management is that no single person has visibility into the full patient journey within a program. blueBriX addresses this through a centralized execution surface with a unified workbench where care teams see patient priorities, pending tasks, open care gaps, and coordination needs across programs, roles, and care settings, without jumping between systems or losing context. Coordinators can manage 30 to 40 percent more patients without increased burnout — not because the work gets easier, but because the platform eliminates the time spent navigating fragmentation.
Multi-program complexity, managed
For patients who qualify for multiple programs simultaneously, blueBriX provides the infrastructure to manage overlapping enrollments without creating operational chaos. Program-level configurations govern how patients move between programs, how referrals are triggered based on assessment scores, and how billing rules are applied across complex multi-payer scenarios.
Real-time quality and risk intelligence
blueBriX captures operational, quality, and value-based performance measures as care is delivered. Care gap status, HEDIS measure progress, risk score trends, and shared savings performance are surfaced in real time, giving care teams and leadership the ability to course-correct before a contract period closes rather than after the damage is done. AI agents integrated into the platform identify rising-risk patients, flag open care gaps, and trigger care plans proactively.
Audit-ready compliance reporting
CMS, Medicare, and payer reporting is always complete, traceable, and submission-ready because data is captured at the point of care, within program-specific workflows. Organizations using blueBriX report cutting reporting effort by up to 70 percent and saving 8 to 12 hours weekly per compliance lead because the infrastructure ensures the right data is captured from the start.
Why well-resourced healthcare programs still underperform
Ready to see how blueBriX’s program management engine can strengthen your VBC strategy? Schedule a demo and let’s talk about what’s holding your programs back.
Explore the hidden causes of program underperformance