

For decades, children and youth with complex medical and behavioral health needs have fallen through the cracks of a fragmented care system. Families struggle to navigate between primary care, behavioral health, specialty services, and community supports — often with no single entity accountable for the whole child. The results are predictable: delayed diagnoses, missed interventions, poor health outcomes, and a troubling pipeline of young people entering adulthood already burdened by unmanaged chronic conditions.
The Centers for Medicare & Medicaid Services (CMS) is moving to change that. With the introduction of the ASPIRE Model — the Accelerating State Pediatric Innovation Readiness and Effectiveness Model. CMS is signaling a major shift in how it expects Medicaid and CHIP to serve the nation’s most vulnerable children and youth.
This is not a distant policy change. With a Notice of Funding Opportunity (NOFO) expected in 2026, states and the healthcare organizations operating within them have a narrow window to understand, prepare, and position themselves for what comes next.
This guide is written for that window. Whether you are a pediatric clinic, a behavioral health provider, a Federally Qualified Health Center (FQHC), an Accountable Care Organization (ACO), or a state Medicaid agency, this article breaks down what ASPIRE is, what it demands of you, and how technology specifically blueBriX can help you meet those demands before the model goes live.
Understanding the ASPIRE Model

ASPIRE is a new care delivery and payment model developed by the CMS Innovation Center (CMMI), the same body responsible for landmark programs like ACO REACH, the Comprehensive Primary Care Plus (CPC+) model, and the Integrated Care for Kids (InCK) model. It is designed to fundamentally restructure how Medicaid and the Children’s Health Insurance Program (CHIP) serve children and youth with complex needs shifting from a fragmented, transactional model to one that is coordinated, whole-person, and accountable for outcomes.
Key Definition: ASPIRE is a state-based, voluntary, 10-year model authorized under Section 1115A of the Social Security Act. Up to five states will be selected to participate through competitive Cooperative Agreements.
The problem ASPIRE is solving
The motivation behind ASPIRE is stark. Approximately half of all children and youth who have or are at risk of developing complex medical and behavioral health needs are covered by Medicaid or CHIP. Yet the care landscape for these children is, at best, difficult to navigate, and at worst, outright inaccessible.
The consequences are not merely clinical. Children who do not receive timely, coordinated care for complex needs face a dramatically elevated risk of:
- Poor educational outcomes and school disengagement
- Escalating care needs that require more intensive and more expensive interventions
- Greater likelihood of entering adulthood with unmanaged chronic conditions
- Higher utilization of emergency departments and inpatient settings as primary care substitutes
- Disrupted family stability, with caregivers bearing disproportionate burdens
ASPIRE is CMS’s answer to this systemic failure. By introducing accountability, coordination, and whole-person care into the Medicaid ecosystem for children, it aims to close these care gaps at scale.
Who is ASPIRE designed for?
ASPIRE targets two distinct populations of children and youth enrolled in Medicaid or CHIP, up to age 21:
- High-Risk Children and youth already living with medically and/or behaviorally complex conditions and those who currently require significant care coordination across multiple systems and settings.
- Rising-Risk Children and youth who have one or more identifiable risk factors for developing a complex condition, those for whom early intervention could prevent a trajectory toward high-cost, high-intensity care.
The dual focus on high-risk and rising-risk populations is intentional and important. ASPIRE is not only a model for managing existing complexity. It is a prevention strategy. This upstream orientation changes the economics and clinical logic of the model significantly.
What conditions does ASPIRE cover?
ASPIRE is deliberately broad in the conditions it encompasses, reflecting the reality that complex pediatric need rarely fits into a single diagnostic category. Covered conditions include:
- Behavioral health conditions (anxiety, depression, trauma, ADHD, and more)
- Substance use disorders
- Chronic physical health conditions (asthma, diabetes, obesity, cardiovascular risk)
- Physical disabilities
- Intellectual and developmental disabilities (IDD)
This breadth is a feature, not an oversight. It reflects CMS’s recognition that the children most in need of coordinated care rarely present with only one challenge — they present with many, spanning clinical, behavioral, social, and developmental domains simultaneously.
State-based structure: 10 years, up to 5 states
ASPIRE is structured as a state-level model, with individual state Medicaid agencies (SMAs) as the primary participants. This is an important design choice, it recognizes that Medicaid infrastructure, provider networks, and care ecosystems vary enormously by state, and that durable change requires state-level leadership and investment.
Key structural parameters:
- Duration: 10 years — long enough to measure population-level outcomes
- Scale: Up to 5 states selected nationally
- Funding mechanism: Cooperative Agreements between CMS and selected SMAs
- Infrastructure investment: States may use a portion of their Cooperative Agreement funding to build care coordination infrastructure and expand access to wrap-around services
Current status and what’s coming
As of early 2026, ASPIRE is in the Announced stage. The model has been formally unveiled by CMS but has not yet begun the state selection process.
Timeline Alert: CMS is expected to release the Notice of Funding Opportunity (NOFO) in 2026. Once released, state Medicaid agencies will have a defined window to submit applications. Organizations that want to serve as accountable entities must begin laying groundwork now.
To be selected, states must demonstrate that sufficient accountable entities exist within the state or that the capacity to build them can be developed during a pre-implementation phase. This means that healthcare organizations in interested states have a direct role to play in shaping their state’s eligibility.
For providers, clinics, health systems, and managed care organizations, the message is clear: the time to prepare is not when the NOFO drops. It is now. Organizations that invest in the infrastructure, workflows, and capabilities required by ASPIRE before the model launches will be positioned to participate and to lead.
Key features of the ASPIRE Model
Whole-person, coordinated care delivery
The organizing philosophy of ASPIRE is whole-person care. This means that participating entities are not expected to address only the presenting clinical condition. They are expected to understand and respond to the full context of a child’s health, including behavioral health, social drivers, family dynamics, and developmental needs. Care coordination is not a supplementary service under ASPIRE, it is the central mechanism. Accountable entities are responsible for ensuring that children receive the right care, at the right time, in the least restrictive setting possible. This requires cross-domain coordination between primary care, behavioral health, specialty providers, schools, and community organizations.
Accountable entities and total cost of care
One of the most structurally significant features of ASPIRE is its accountability framework. States will partner with ‘accountable entities’ organizations that take on responsibility for managing both the quality and total cost of care for covered children and youth. Examples of accountable entities include Managed Care Plans and Accountable Care Organizations (ACOs). These entities must partner with providers who have specialized experience delivering care for high- and rising-risk children. The total cost of care model introduces financial accountability alongside quality accountability, a meaningful departure from the fee-for-service logic that has dominated Medicaid pediatric care.
Wrap-around services and family empowerment
ASPIRE recognizes that clinical care alone is insufficient for children with complex needs. The model explicitly requires the delivery of supportive, wrap-around services that address physical and behavioral health needs holistically including housing support, transportation, food security, school coordination, and other social determinants. Equally important is the model’s emphasis on family empowerment. Parents and caregivers are not passive recipients of information under ASPIRE. They are active partners in care. The model requires that resources and education be provided to help families understand their child’s conditions, navigate care systems, and participate meaningfully in care planning and decision-making.
Transition-to-adulthood planning
Perhaps the most forward-looking feature of ASPIRE is its explicit focus on the transition from pediatric to adult care. For young people with complex health needs, this transition is notoriously poorly managed, and the consequences are severe. Many young adults experience a dramatic deterioration in health outcomes, employment, and independence in the years immediately following their exit from pediatric care systems. ASPIRE builds long-term transition planning into its care model from the outset. Participating entities are expected to develop and execute plans that support health, productivity, and economic stability as children age into adulthood, making ASPIRE one of the first Medicaid models to treat the transition to adulthood as a core quality and outcome metric, not an afterthought.
What providers and healthcare organizations need to know
ASPIRE touches a wide range of stakeholders across the healthcare ecosystem. Each has a distinct stake in and a distinct role to play within the model. Here is what each audience needs to understand.
Pediatric specialists and clinicians
For pediatricians, child psychiatrists, developmental pediatricians, and other pediatric specialists, ASPIRE represents a fundamental shift in what ‘good care’ is measured against. Quality metrics under ASPIRE will reflect whole-person outcomes not just individual encounter quality. This means that specialists will increasingly need to:
- Document and share care plans across organizational boundaries
- Coordinate with behavioral health and social service providers as routine practice
- Track patient outcomes longitudinally, not episodically
- Engage families as partners in goal-setting and care execution
Specialists who are accustomed to functioning as independent referral destinations will need to adapt to a more integrated care team model. Those who proactively build the workflows and relationships to support this shift will have a significant competitive and quality advantage.
FQHCs and community health clinics
Federally Qualified Health Centers and community health clinics serve disproportionately high concentrations of Medicaid and CHIP enrolled children with complex needs. They are natural candidates to serve as or to partner with accountable entities under ASPIRE. For FQHCs, ASPIRE represents both an opportunity and an obligation. The model’s emphasis on wrap-around services, family empowerment, and community-based care aligns closely with the FQHC mission. However, participating effectively in ASPIRE requires significant investment in care coordination infrastructure and in the capabilities needed to manage complex, multi-domain patient panels at scale, report on quality metrics, and coordinate care across a broad ecosystem of partners.
Behavioral health providers
ASPIRE is one of the most significant federal investments in integrated behavioral health for children in a generation. Behavioral health conditions are among the most prevalent complex needs in the target population, and the model explicitly requires that behavioral health be integrated into and not siloed from the overall care model. For behavioral health organizations, ASPIRE creates a real opportunity to move from the periphery of the care system to its center. But this requires demonstrating the ability to coordinate with physical health providers, share clinical data across systems, participate in joint care planning, and report outcomes in the language of value-based care. Behavioral health providers who can credibly operate in this integrated model will be essential partners for any accountable entity seeking to serve ASPIRE’s target population.
ACOs and managed care plans
For Accountable Care Organizations and Managed Care Plans, ASPIRE creates a new accountability surface: total cost of care for a high-complexity pediatric population. This is both a financial opportunity and a financial risk. The upside is significant — organizations that can effectively coordinate care and reduce avoidable utilization in this population will generate meaningful savings under the model’s payment structures. But realizing that upside requires genuine capability in pediatric care coordination, risk stratification, and quality reporting, capabilities that many ACOs built for adult populations will need to adapt significantly for a pediatric context. ACOs and MCOs should begin now by assessing their current pediatric care coordination capabilities, identifying gaps in their provider networks for high- and rising-risk children, and investing in the technology infrastructure that will allow them to meet ASPIRE’s reporting and accountability requirements.
State Medicaid agencies
State Medicaid agencies are the primary entry point for ASPIRE. Only SMAs can apply for and receive Cooperative Agreement funding. But the selection criteria which will be detailed in the NOFO will hinge significantly on the strength and readiness of the accountable entities and provider networks within the state. States interested in participating should be conducting ecosystem assessments now:
- Which organizations in our state have the capacity to serve as accountable entities?
- Where are the gaps in our pediatric behavioral health and specialty provider networks?
- What data infrastructure exists, and what needs to be built?
States that have already invested in care coordination technology infrastructure, integrated behavioral health, and value-based care contracting will be better positioned to compete for the limited number of ASPIRE slots.
Health systems with pediatric programs
Large health systems with pediatric programs or children’s hospitals have a unique role in the ASPIRE ecosystem. They typically have the clinical depth, specialty networks, and data infrastructure that accountable entities will need to access but their organizational complexity can also make them slow to adapt. Health systems should evaluate ASPIRE not only as a compliance or regulatory matter, but as a strategic one. The model will reshape referral patterns, care coordination expectations, and quality benchmarking in the Medicaid pediatric market. Systems that align their operational and technology infrastructure with ASPIRE’s requirements ahead of the model launch will be positioned as preferred partners for accountable entities seeking network depth.
The operational challenges ASPIRE will create

Understanding ASPIRE conceptually is one thing. Operationalizing it is another. Across every segment of the provider ecosystem, ASPIRE will create real, concrete operational demands that current systems and workflows are often poorly equipped to meet. Here are the five most significant challenges organizations will face.
Managing high-risk and rising-risk populations at scale
ASPIRE requires accountable entities to identify, stratify, and actively manage two distinct patient populations simultaneously. The high-risk population requires intensive, ongoing coordination. The rising-risk population requires proactive outreach and early intervention meaning organizations must act on patients who have not yet presented with a crisis. Most organizations lack the ability to do both simultaneously at population scale. Manual tracking, fragmented EHR data, and siloed care teams make it nearly impossible to maintain consistent visibility into which patients need immediate intervention and which need preventive outreach.
Coordinating across physical, behavioral, and social domains
ASPIRE’s whole-person care model requires coordination across clinical domains that have historically operated in almost complete isolation. Primary care providers, behavioral health clinicians, social workers, school liaisons, and community health workers must function as a coherent care team sharing information, aligning on care plans, and closing care loops reliably. The technology infrastructure to support this kind of cross-domain coordination; shared care plans, closed-loop referral management, multi-role care team workbenches is absent in most organizations today.
Reporting on quality and cost outcomes to CMS
ASPIRE is a value-based model, and value-based models require value-based reporting. Accountable entities will need to demonstrate performance on quality metrics and total cost of care on an ongoing basis. This requires that clinical activity, care coordination touchpoints, and outcomes be captured systematically and not reconstructed retroactively from billing data. Organizations that lack automated, real-time quality and compliance reporting will face significant manual burden and reporting risk under ASPIRE.
Empowering families as active care partners
ASPIRE’s emphasis on family empowerment is a structural requirement of the care model. Organizations must have the tools to engage parents and caregivers meaningfully:
- Communicating care plans in accessible formats
- Capturing caregiver input
- Tracking family-defined goals
- Maintaining engagement between clinical encounters.
This level of patient and family engagement is significantly more demanding than the portal access and appointment reminders that most organizations currently provide.
Planning for and executing the transition to adulthood
Longitudinal transition planning is an area where virtually every pediatric care system is currently underprepared. Most organizations have no systematic process for identifying young patients approaching the transition age, initiating transition planning, coordinating with adult-care providers, and tracking outcomes post-transition. ASPIRE will require this capability at scale. Organizations that build it proactively will meet the model’s requirements, and they will deliver genuinely better outcomes for some of the most vulnerable young people in their care.
How blueBriX can help you prepare for ASPIRE
blueBriX is an enterprise care management platform built specifically for value-based care. With integrated EHR capabilities, configurable care coordination workflows, population health tools, and CMS-ready reporting, blueBriX is designed to address exactly the operational challenges that ASPIRE will create. Here is how.
Care coordination built for complex, multi-domain populations
blueBriX is a care coordination platform that is purpose-built for the kind of complex, multi-domain population management that ASPIRE requires. The platform provides care teams with a centralized workbench that surfaces patient priorities, routes tasks, and enables seamless collaboration across disciplines all without requiring clinicians to juggle multiple disconnected systems. For ASPIRE-participating organizations, this means care coordinators can manage both high-risk and rising-risk children within a single platform, with real-time visibility into each patient’s care plan status, open care gaps, scheduled touchpoints, and outstanding referrals. Organizations using blueBriX can enable coordinators to manage
30–40% more patients without increasing burnout; a critical capability for organizations taking on accountability for large pediatric populations.
Configurable workflows for pediatric and behavioral health programs
ASPIRE’s requirement for integrated physical and behavioral health care demands workflows that can span clinical domains. blueBriX’s low-code, no-code workflow engine allows organizations to design and deploy care workflows that reflect the actual clinical logic of pediatric and behavioral health integration without expensive custom development. Organizations can configure ASPIRE-aligned programs within the platform: intake workflows, assessment tools, care planning templates, and intervention protocols tailored to the specific needs of high-risk and rising-risk pediatric populations. These workflows can be adapted as the model evolves, ensuring that organizations remain agile as ASPIRE implementation matures.
Risk stratification and population health management
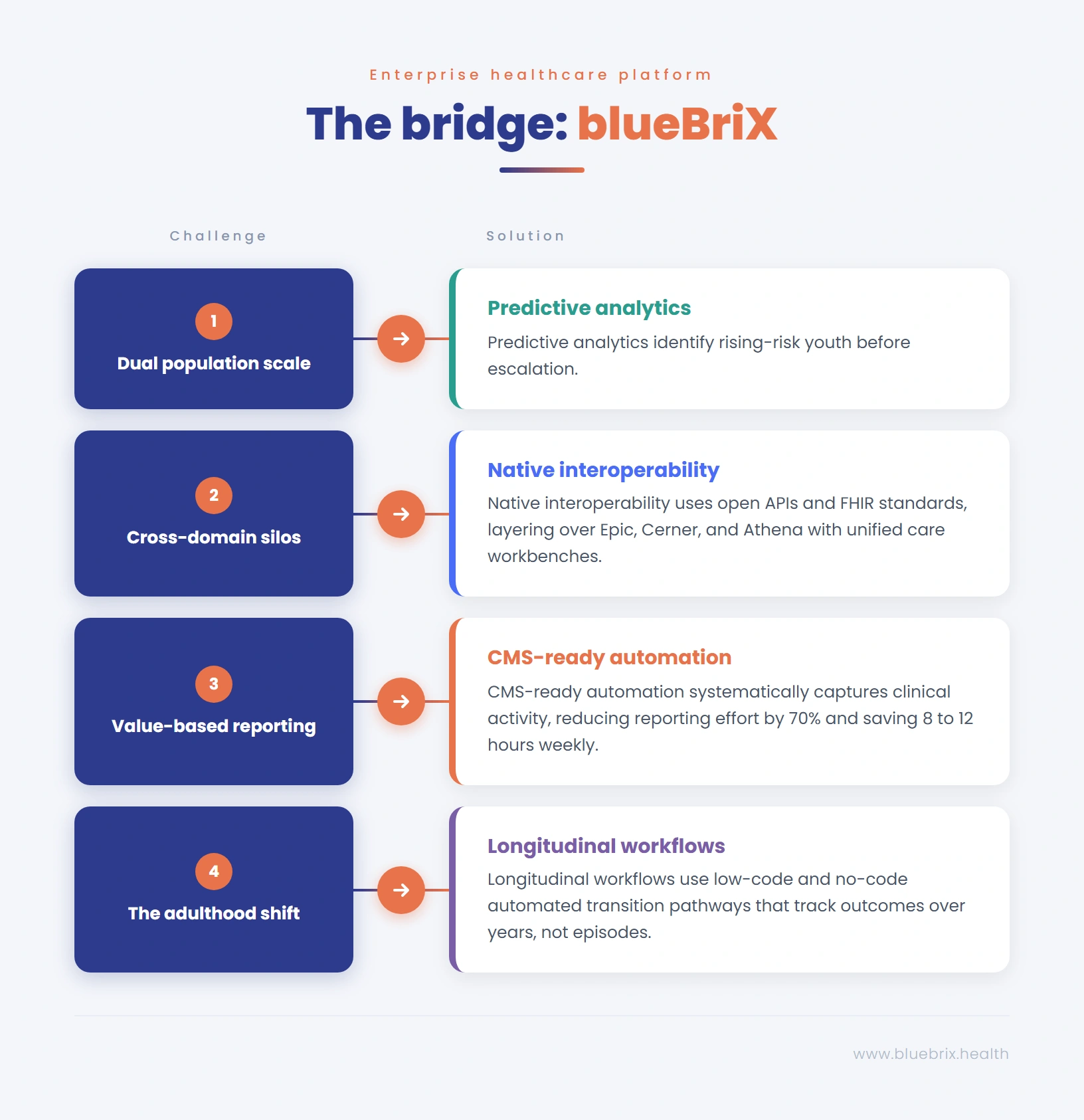
Meeting ASPIRE’s dual population mandate serving high-risk patients intensively and proactively reaching rising-risk patients requires sophisticated risk stratification. blueBriX’s population health management tools aggregate clinical data across the patient panel, identify patients by risk tier, and generate actionable outreach lists for care teams. Predictive analytics capabilities allow organizations to surface rising-risk patients before they escalate enabling the kind of early intervention that is at the core of ASPIRE’s prevention strategy and that generates the most significant long-term savings under a total cost of care model.
CMS-ready reporting and compliance documentation
Accountability under ASPIRE means reporting. blueBriX captures operational, quality, and value-based measures as care is delivered ensuring that CMS, payer, and Cooperative Agreement reporting is always complete, traceable, and submission-ready. Organizations can cut reporting effort by up to 70% and save 8–12 hours weekly per compliance to lead a meaningful return on investment for organizations facing the demanding reporting requirements of a multi-year federal model. For accountable entities managing ASPIRE Cooperative Agreement compliance, this level of reporting automation is a necessity.
Family and caregiver engagement tools
blueBriX includes robust patient and family engagement capabilities designed to support the kind of meaningful caregiver partnership that ASPIRE requires. Care plans can be shared with families in accessible formats, family-defined goals can be incorporated into the treatment plan, and engagement touchpoints can be tracked longitudinally, creating a documented record of family involvement that meets ASPIRE’s accountability standards.
Interoperability with Existing EHRs
ASPIRE will require data sharing across a complex ecosystem of providers. blueBriX integrates seamlessly with all major EHR platforms Epic, Athena, Cerner, Meditech, and others via open APIs and FHIR-standard data exchange. This means organizations do not need to rip and replace their existing clinical infrastructure to participate in ASPIRE. blueBriX layers on top of existing systems, consolidating the patient data needed for coordinated care without disrupting clinical workflows. For accountable entities managing networks of diverse providers each with their own EHR this interoperability capability is essential for maintaining the unified patient view that whole-person care requires.
Supporting the Transition-to-Adulthood Continuum
The transition from pediatric to adult care is one of the most complex and consequential clinical challenges in ASPIRE’s scope and one of the areas where most organizations currently have the largest gaps. blueBriX supports longitudinal care planning that can track a patient’s care trajectory over years, not just episodes. Organizations can configure transition planning workflows within the platform triggering structured transition processes when patients approach the relevant age thresholds, coordinating with adult-care providers, documenting transition plans, and tracking outcomes post-transition. This capability transforms transition planning from an ad hoc, provider-dependent process into a systematic, accountable program.


