The high-stakes strategic pivot of 2027
Let’s be direct: 2027 isn’t just another policy cycle year. For behavioral health organizations – Community Mental Health Centers, large SUD programs, CCBHCs, and integrated behavioral health networks – it is a genuine inflection point that will shape financial sustainability for the next decade.
Here’s why.
ACO REACH ends on December 31, 2026. In its place, CMS is launching the Long-term Enhanced ACO Design (LEAD) model – a 10-year voluntary program that begins January 1, 2027 and runs through December 31, 2036. At the same time, the Medicare Shared Savings Program (MSSP) continues as the permanent, institutional backbone of Medicare’s ACO strategy. Two very different pathways, two very different financial architectures, and for behavioral health organizations, the choice between them is arguably the most consequential strategic decision of the next ten years.
The May 17, 2026 application deadline for the first LEAD cohort makes this decision immediate, not theoretical.
Part 1 of this blog is designed to cut through the policy language and give behavioral health leadership teams – CFOs, CMOs, and operations heads – a clear, practical framework for evaluating which model their organization is truly built for. One structural clarification matters upfront: CMS defines LEAD participants as ACOs comprised of participant TINs, most commonly primary care practices. Behavioral health organizations typically enter this picture as part of an ACO – either by joining an existing one, by partnering to form one anchored by primary care TINs, or in some cases as the organizing entity itself for CCBHCs and integrated health centers. The strategic and financial questions this guide addresses apply regardless of which role your organization occupies in that structure. At blueBriX, we have worked with behavioral health organizations at every stage of this transition – and what follows reflects what consistently separates ACOs that generate meaningful shared savings from those that don’t.
Demystifying the two titans: LEAD and MSSP decoded for behavioral health leaders
Before you can compare them intelligently, you need to understand what each model actually does – not just in federal register language, but in terms of how money flows, how risk is shared, and where each model creates structural advantages or structural traps for behavioral health providers.
The Long-term Enhanced ACO Design (LEAD) model: CMS’s long game
LEAD was built to solve a specific, persistent problem: the fact that high-performing ACOs were being penalized for their own success. In earlier models, including ACO REACH, organizations that successfully reduced costs often saw their benchmark recalibrated downward at renewal – effectively taxing away the efficiency gains they had worked hard to achieve. For behavioral health providers, whose care transformation programs require years of upfront investment before generating measurable savings, this created an impossible math problem.
LEAD addresses this by establishing a historical spending baseline from CY 2024–2026 without benchmark rebasing. LEAD does not rebase benchmarks; CMS plans a regional rate book transition after year five, but that is a methodology refinement rather than the performance-penalizing recalculation that ACO REACH participants experienced. That means every dollar of clinical improvement compounds into a widening gap between the baseline CMS uses and what your organization actually spends – and that gap is where shared savings live. For a fuller breakdown of the LEAD model’s architecture, see the complete guide to ACO LEAD.
LEAD also introduces a 1.5% administrative add-on payment for higher-spending ACOs. For behavioral health organizations that have historically operated on paper-thin margins, this is non-trivial startup capital to fund the infrastructure investments that value-based care requires. LEAD explicitly encourages participation by smaller, independent, and rural-based practices, as well as organizations serving high-needs populations – a category that overlaps significantly with the populations most behavioral health organizations serve.
The Medicare Shared Savings Program (MSSP): the institutional standard
MSSP is not a pilot. It is not a demonstration model. It is the permanent, flagship ACO program for Medicare fee-for-service – and that permanence carries real strategic weight. MSSP offers a BASIC glide path for organizations new to risk and an enhanced track for those ready to take on greater two-sided exposure in exchange for higher shared savings rates.
However, for high-performing behavioral health organizations, MSSP carries a structural liability that deserves serious attention: the rebasing cycle. Every five-year agreement period, the benchmark is recalculated to reflect the ACO’s actual efficiency gains. In practical terms, this means an organization that dramatically reduces avoidable ED visits, unnecessary psychiatric hospitalizations, and SUD-related readmissions enters its next MSSP agreement period with a lower benchmark ceiling – less room to generate savings – even though its care model is performing exactly as intended.
Bottom line: This “ratchet effect” is the primary reason high-performing behavioral health groups are now evaluating LEAD. It is not an ideological preference. It is financial logic.
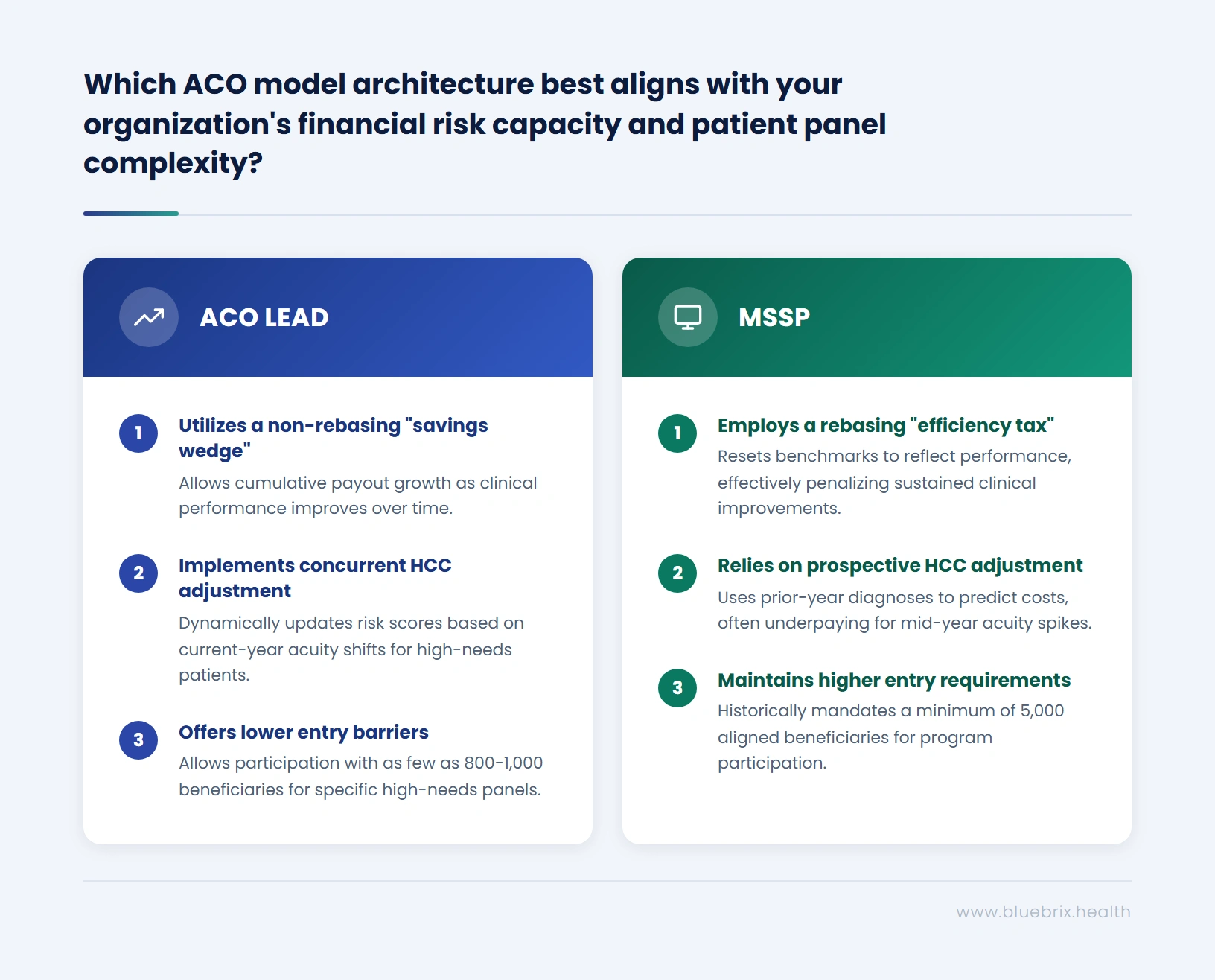
ACO LEAD vs. MSSP: financial risk architecture and shared savings comparison
The structural differences between LEAD and MSSP are not abstract – they translate directly into whether your organization produces a surplus or absorbs a loss at year-end.
Benchmarking methodology: the “savings wedge” vs. the “efficiency tax”
Under LEAD’s non-rebasing baseline, financial planners describe the “Savings Wedge” – a widening gap between the stable benchmark and actual spend that compounds over time as clinical transformation takes hold. Picture an ACO serving a behavioral health-heavy panel that reduces its psychiatric readmission rate over three years. Under LEAD, every subsequent year of that lower readmission rate generates savings against the same baseline – CMS does not recalculate the ceiling to reflect your improved performance. The gap – and the payout – keeps growing.
Under MSSP’s rebasing logic, that same reduction gets written into the new benchmark at the next agreement period. The organization is now expected to perform at its improved level without being compensated for achieving it. This is the efficiency tax in practice.
For any ACO serving a behavioral health-heavy panel and actively investing in care transformation – integrated care workflows, peer support specialists, housing navigation, medication management – the savings compounding effect under LEAD’s stable benchmark can represent a substantial difference in cumulative shared savings compared to MSSP’s five-year renewal cycles. The barriers to VBC adoption in behavioral health are well-documented, and the benchmarking structure is one of the most underappreciated among them.
MSSP and ACO LEAD risk tracks: upside-only vs. two-sided risk for behavioral health ACOs
Both LEAD and MSSP offer two-sided risk tracks, but the structure and demands differ in important ways.
LEAD risk tracks
- Professional Risk Track (up to 50%): No benchmark discount, meaning first-dollar savings are accessible from the start. Primary care capitation is available in this track. Organizations must commit to four years in the Professional track before switching to Global. A structured on-ramp for ACOs serving behavioral health-heavy panels that are newer to downside risk.
- Global Risk Track (up to 100%): The only track offering total care capitation – full coverage of all Medicare Part A and B spending. Primary care capitation is available in both tracks, but total care capitation is exclusive to global risk. This track carries maximum upside but requires capital reserves, robust data infrastructure, and strong utilization management. Not every behavioral health-aligned ACO is operationally ready for this from day one.
MSSP risk tracks
- BASIC Track: A glide path for organizations entering value-based risk for the first time. Lower upside, but limited downside exposure in early years.
- ENHANCED Track (up to 75%): Higher shared savings rates in exchange for corresponding downside exposure – demands the same operational infrastructure as LEAD’s global track.
Key CFO question: Does your organization currently have the claims analytics, reserve capital, and utilization management infrastructure to absorb downside risk? If not, LEAD’s Professional track on-ramp is designed for where you are today.
Risk adjustment for behavioral health populations: why the concurrent HCC model changes everything
This is where the difference between the two models becomes financially decisive for behavioral health providers – not just operationally significant.
The standard prospective HCC (Hierarchical Condition Category) risk adjustment model works like this: it uses a patient’s prior-year diagnoses to predict current-year costs and sets the benchmark accordingly. For a stable diabetic patient, this model works reasonably well. For a psychiatric patient or someone in active SUD recovery – where acuity can shift dramatically mid-year – it creates a systematic underpayment problem. A patient who appears “stable” in January but deteriorates significantly in September generates costs the benchmark never accounted for, and the ACO absorbs the difference.
LEAD’s concurrent HCC model for high-needs populations corrects this by adjusting risk scores using current-year data. If a patient’s complexity spikes in Q3, the risk adjustment updates to reflect that reality rather than locking the ACO into an artificially low benchmark. To be precise: LEAD applies concurrent HCC specifically to its High Needs population segment; Aged and Disabled beneficiaries use prospective adjustment. For behavioral health-heavy patient panels – where SMI and SUD populations routinely experience mid-year acuity shifts and qualify disproportionately for high needs status – this distinction is not a technical footnote. It is the difference between a benchmark that financially accounts for the population you are managing and one that systematically underpays for it.
This distinction is particularly urgent in the context of the ongoing V28 HCC model transition, which has already been affecting risk scores for complex behavioral health diagnoses and comorbidities. The stakes of getting risk adjustment right have never been higher.
ACO LEAD eligibility requirements: beneficiary thresholds and the on-ramp advantage
MSSP has historically required 5,000 aligned beneficiaries as a minimum – a threshold that has effectively locked most small and mid-sized behavioral health providers out of the program. An organization running a 1,200-patient panel with a high proportion of dual-eligible and SMI beneficiaries simply couldn’t clear that bar.
LEAD addresses this with distinct entry thresholds by ACO type. Newly Entering ACOs – those that have not previously participated in a CMS ACO model – can start with as few as 1,000 aligned beneficiaries (600 in a base year). ACOs where more than 40% of beneficiaries qualify as High Needs can enter with as few as 800 beneficiaries (600 in a base year). These are distinct categories with distinct criteria – not a single tiered floor – and they represent a deliberate structural correction for a behavioral health provider ecosystem that has been disproportionately excluded from value-based participation.
Want to model your specific shared savings under both LEAD and MSSP before May 17? The window to lock in your highest possible benchmark is closing, every month of delay is a month of improved performance that gets written into your baseline before you ever sign a contract. If you’re serious about entering LEAD or MSSP in 2027, this is the conversation that needs to happen now, not after the deadline passes.
Schedule a 30-minute readiness callThe behavioral health difference: why standard ACO logic doesn’t apply here
Most ACO playbooks were written with primary care at the center. Behavioral health organizations operate in fundamentally different clinical and financial territory – and the model they choose must account for that.
The total cost of care profile for patients with Serious Mental Illness (SMI) or Substance Use Disorders (SUD) is driven by distinct cost vectors: untreated physical comorbidities (cardiovascular disease, diabetes, and respiratory conditions are dramatically overrepresented in SMI populations), medication interactions, fragmented specialist relationships, and high-acuity crisis episodes that land in EDs. None of these are captured well by standard ACO analytics designed for primary care panels. As covered in depth in our piece on documentation for value-based care in behavioral health, the shift from documenting “sessions” to proving “outcomes” is the central operational challenge for behavioral health organizations entering risk-based models.
The data behind the behavioral health cost premium:
- Medicare spends approximately 50% more annually on beneficiaries with serious mental illness ($19,676 vs. $13,072 risk-adjusted) – a roughly $6,600 per-beneficiary gap driven largely by unmanaged physical comorbidities, not psychiatric care itself. (Figueroa et al., JAMA Network Open, 2020; 4.35M Medicare beneficiaries)
- In 2024, 61.5 million adults – nearly 1 in 4 – experienced any mental illness, with 14.6 million meeting criteria for SMI. Among adults with SMI, nearly 47.3% also met criteria for a substance use disorder – making co-occurring populations the rule, not the exception. (SAMHSA, 2024 NSDUH)
- Mental health disorders account for approximately 12.7% of all Medicare spending – three times the share attributable to mental health services alone, with the remaining two-thirds driven by downstream physical health costs in populations with untreated or undertreated psychiatric conditions. (Figueroa et al., JAMA Network Open, 2020
Social Determinants of Health (SDOH) are not a values statement for behavioral health organizations – they are an operational necessity directly tied to shared savings performance. Housing instability drives psychiatric readmissions. Transportation gaps cause missed medication management appointments. Food insecurity worsens treatment adherence. For a behavioral health-led ACO under either LEAD or MSSP, the ability to systematically identify, document, and address SDOH factors is the difference between a panel that trends toward lower utilization and one that cycles through crisis episodes indefinitely.
LEAD introduces CMS-Administered Risk Arrangements (CARA) as a voluntary tool – but with important parameters that need to be understood clearly. CARA is available only to LEAD ACOs that elect the Global Risk Option, and episode triggering is expected to begin in PY2028 – these dates are tentative and subject to change per CMS’s own factsheet. For ACOs that qualify and elect it, CARA enables specialists to participate in shared risk arrangements for specific episodes through a CMS-standardized mechanism, without requiring the ACO to negotiate complex bilateral contracts. For behavioral health-aligned ACOs that eventually move to global risk, CARA has real potential to bridge the structural gap between behavioral and physical care delivery – but organizations should plan for that capability to become operational in year two, not year one.
The decision framework: how to choose between LEAD and MSSP
This is the core of what behavioral health leadership teams need to work through – not in the abstract, but in concrete operational terms applied to your specific organization.
Organizational readiness assessment: 5 questions every behavioral health leadership team must answer
Before modeling financials, answer these five questions with operational candor:
- Does your panel meet LEAD’s beneficiary thresholds? LEAD offers reduced entry thresholds for specific ACO types: 1,000 beneficiaries for newly Entering ACOs, and 800 for ACOs where more than 40% of beneficiaries qualify as High Needs. These are distinct criteria, not a single tiered floor. If your panel is under 5,000, confirm which category your organization qualifies for – MSSP’s 5,000-beneficiary minimum may still be a barrier.
- Do you have real-time claims analytics and attribution monitoring? Value-based contracts require continuous visibility into utilization patterns, cost trends, and attributed beneficiary lists. If you’re relying on periodic payer reports rather than real-time internal analytics, you have a readiness gap that needs to close before go-live.
- Can your organization absorb downside risk today? This is a CFO question, not a strategy question. Downside risk requires actual capital reserves or reinsurance arrangements. Wishful thinking about future performance is not a risk management strategy.
- Are your clinical workflows built for point-of-care quality capture? MSSP ACOs are required to report APP Plus quality data, with CMS permitting eCQMs, MIPS CQMs, or Medicare CQMs as reporting methods. LEAD phases in eCQM requirements over four years. Either way, quality data captured retrospectively via chart review rather than at the point of care will underperform your actual clinical results – and leave shared savings on the table.
- Is your care coordination infrastructure ready for whole-person risk? TCM protocols, warm handoff workflows, peer support integration, and community health worker programs aren’t nice-to-haves under risk. They are the primary levers your care team has to bend the utilization curve on high-cost populations.
What compliance and quality leaders need to know
Model selection carries distinct compliance obligations that deserve early attention from quality and compliance leadership – not just the CFO and CMO.
Quality reporting: Both models require quality reporting, but on different timelines. MSSP ACOs must report APP Plus measures beginning PY2025. LEAD offers a four-year eCQM phase-in. In either case, quality data captured retrospectively through chart review consistently underperforms what organizations actually achieve clinically – and that gap translates directly into shared savings left on the table. The compliance imperative is to build point-of-care capture workflows now, not at year three.
Behavioral health parity and documentation: CMS is actively expanding behavioral health quality measures under both programs. Organizations that do not have structured documentation workflows for SDOH screening, depression follow-up, and SUD treatment engagement will face quality score deficits – and compliance exposure – as these measures move from optional to required.
Downside risk governance: For organizations entering two-sided risk, compliance leadership should be involved in the reserve capital analysis and reinsurance decisions early. Shared loss repayment obligations require the same rigor as any other financial liability – and ACOs that absorb losses without a pre-established governance framework face operational disruption that extends well beyond the finance team.
Financial modeling: running the savings wedge scenario for your population
The most important financial exercise you can do before the May 17 deadline is to run a five-year and ten-year shared savings projection under both models using your own utilization data.
The variables that matter most for behavioral health populations in this analysis are: ED utilization rates (particularly psychiatric ED visits), avoidable inpatient psychiatric hospitalizations, post-discharge follow-up rates at 7 and 30 days, and polypharmacy-related adverse events. These are the categories where behavioral health organizations have the most leverage to reduce costs – and where the difference between LEAD’s locked benchmark and MSSP’s rebased benchmark becomes most visible over time.
If your panel shows a meaningful opportunity to reduce psychiatric readmissions or ED utilization through improved care management, the compounding effect under LEAD’s non-rebasing benchmark is likely to be substantially more favorable than five-year MSSP renewal cycles – because under LEAD, those savings keep paying out against the same baseline year after year, rather than being baked into a recalculated ceiling.
Clinical capacity: assessing readiness for whole-person care under risk
Value-based risk requires integrated care workflows that most behavioral health organizations have not yet fully operationalized. What does physical-behavioral integration look like in practice for your organization today?
Specifically: Do your care teams have reliable access to patients’ physical health data – lab results, primary care visit summaries, specialist notes – at the point of behavioral health encounters? Do you have systematic TCM protocols that activate when a patient is discharged from an inpatient psychiatric stay? Do your case managers know within 24 hours when a high-risk patient presents to an ED?
These are not aspirational questions. Under either LEAD or MSSP, these workflows are the operational engine that drives performance. Organizations that have built these capabilities – even partially – are in a meaningfully different position to succeed under risk than those that have not.
Technology readiness: can your systems support what these models require?
EHR data completeness, ADT (Admission-Discharge-Transfer) feed integration, and eCQM readiness are not optional enhancements – they are baseline requirements for performing under risk.
LEAD provides a structured four-year eCQM phase-in, which creates a genuine window to build toward full compliance rather than requiring it at day one. But “phase-in” is not a synonym for “optional.” Organizations that use the phase-in period to build solid quality infrastructure will emerge in years three and four with strong quality performance that drives additional shared savings. Those that treat the phase-in as a reason to delay technology investment will find themselves playing catch-up when full quality reporting requirements kick in.
The technology gap most behavioral health-aligned ACOs face is not primarily about EHR selection – it’s about data flow: getting ADT alerts in real time, connecting behavioral health data to physical health claims, maintaining an attributed population list that is current and actionable, and building the analytics layer that tells care coordinators who to call, when to call them, and why. The shift in how behavioral health documentation must function under value-based care – from capturing services to proving outcomes – is inseparable from this data infrastructure question.
Side-by-side decision matrix
The table below summarizes the most consequential differences across the criteria that matter for behavioral health organizations. Use it as an alignment tool for your leadership team.
| Criteria | ACO LEAD | MSSP |
|---|---|---|
| Benchmarking stability | No benchmark rebasing throughout the performance period. CMS plans a regional rate book methodology transition after year five – a refinement, not a performance penalty. Savings compound against the same baseline. | Rebased every 5-year agreement period. Efficiency gains get written into the next period’s benchmark: the ratchet effect. |
| High-needs population fit | Concurrent HCC risk adjustment for the High Needs population segment – updates mid-year when patient acuity spikes. Aged & Disabled use prospective adjustment. Built for SMI/SUD panels. | Prospective HCC only – prior-year diagnoses drive current-year benchmark. Systematically underpays for mid-year acuity shifts. |
| Entry requirements | Newly Entering ACOs: 1,000 beneficiaries (600 base year). ACOs with >40% High Needs: 800 (600 base year). Standard minimum: 5,000. Three distinct categories, each with specific criteria. | 5,000 beneficiaries from day one – a longstanding barrier for smaller behavioral health providers. |
| Risk track options | Professional (up to 50%, primary care capitation available) and Global (up to 100%, total care capitation exclusive to this track). 4-year commitment before switching tracks. | BASIC glide path and ENHANCED track (up to 75%). Structured for providers at various risk maturity levels. |
| Administrative support | 1.5% add-on payment for higher-spending ACOs – non-repayable startup capital. | No comparable add-on payment for new entrants. |
| eCQM readiness timeline | 4-year phased approach: optional (PY1–2), pay-for-reporting (PY3–4), pay-for-performance (PY5–10). Structured window to build quality infrastructure. | ACOs report APP Plus quality data beginning PY2025. CMS permits reporting via eCQMs, MIPS CQMs, or Medicare CQMs per 2026 guidance. |
| Specialist coordination | CARA (CMS-Administered Risk Arrangements) available voluntarily to ACOs electing Global Risk, with episode triggering expected to begin in PY2028 (tentative per CMS). Standardized episodes – no bilateral contracting required. | Direct contracting with specialists required. More complex to operationalize for behavioral health-aligned ACOs. |
| Model duration & permanence | 10 years (2027–2036). Longest CMS ACO model ever – predictable long-term planning horizon. | Permanent program – 5-year renewable agreements. Not a demonstration model; long-term CMS policy direction. |
| Best fit for BH organizations | High-performing or high-needs-serving organizations seeking long-term benchmark stability; new-to-ACO entrants with panels 800–5,000. | Organizations with larger panels, established MSSP track record, or preference for a permanent program. |
The cost of standing still: why delay is not a neutral choice
Before closing the decision framework, it is essential to name the risks of inaction directly. Every behavioral health organization considering LEAD or MSSP should weigh what staying still actually costs:
- Baseline erosion: Every year a behavioral health organization improves care delivery outside of a VBC contract, it lowers the spending baseline that any future contract will be measured against. Entering LEAD in 2027 locks in the benchmark at its highest defensible historical point. Waiting until 2029 means entering with an already-compressed benchmark and less room to generate savings from day one.
- Compliance costs without upside: CMS is expanding quality reporting mandates – including behavioral health measures – regardless of what payment model an organization participates in. Organizations outside a VBC contract absorb those reporting costs with no shared savings upside to offset them.
- The 2030 mandate and closing window: CMS has set a clear policy direction of 100% of Traditional Medicare beneficiaries in accountable care relationships by 2030. Late entry means smaller attribution panels, compressed benchmarks, and a weaker negotiating position with network partners who increasingly prefer established ACO relationships.
- The May 17, 2026 deadline is a genuine strategic marker: Applications for the first LEAD cohort are due May 17, 2026. Missing that window does not mean waiting one year – it means waiting until the next cohort with a lower historical baseline and less runway to build the care model before savings are measured.