The green dashboard illusion
Picture this: It is the first Monday of the month. You are the VP of revenue cycle for a mid-sized health system. You walk into the monthly finance meeting, coffee in hand, feeling good. The dashboard on the screen is mostly green. Days in A/R are down. The clean claim rate is up to 94%. The denial rate has ticked down by half a percent.
On paper, your team is winning. But then the CFO asks a question that stops the room cold: “If our efficiency metrics are up, why is our Net Patient Revenue (NPR) per case slipping for our Medicare Advantage population?”
The room goes quiet. You don’t have an answer immediately, but the answer is hiding in plain sight. It isn’t in the claims you didn’t get paid for (denials). It is in the claims you did get paid for.
You are suffering from the underpayment epidemic.
We treat the paid status in our billing systems like a victory flag. When a claim turns green, we move on. But in the complex world of value-based care (VBC), a paid claim is often a partially paid claim in disguise.
Industry data suggests providers lose an estimated 3-5% of their net revenue annually to underpayments. In a fee-for-service world, that was a margin error. In a value-based world, where margins are razor-thin and operational costs are soaring, losing 5% of your revenue to bad payer math is a crisis you cannot afford to ignore.
This blog is about how we stop trusting the paid status and start verifying it. It is about the shift from denial management to revenue integrity, and how a new approach called shadow reconciliation is the only way to survive the complexity of modern payer contracts.
The counter-agentic reality: bringing a calculator to a supercomputer fight
In our previous article on automating coordination of benefits, we explored the concept of counter-agentic AI. This is the reality that payers, large commercial insurers and even CMS intermediaries, are not neutral administrative bodies. They are active agents with their own financial imperatives.
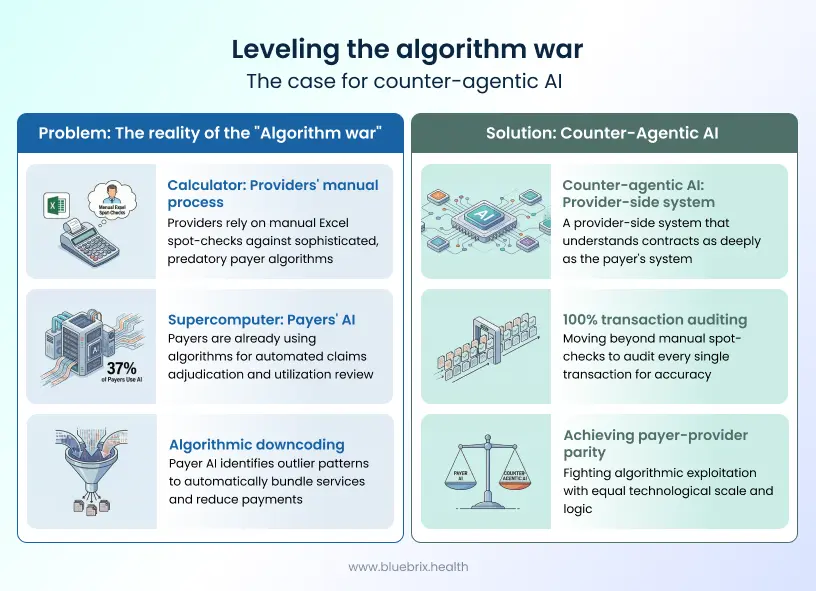
Today, payers are deploying sophisticated AI algorithms to adjudicate your claims. These systems are not just looking for typos; they are optimizing payment logic in their favor.
- They use AI to identify outlier coding patterns and automatically downcode them.
- They use algorithms to bundle distinct services into a single payment.
- They use predictive models to interpret clinical data in the way most favorable to their bottom line.
According to a recent report, 37% of payers are now using AI for claims adjudication and utilization review. Here is the problem: Most providers are still checking these claims with Excel spreadsheets and manual spot checks.
You are effectively bringing a pocket calculator to a supercomputer fight. If your RCM strategy relies on human billers catching algorithmic underpayments, you have already lost. The payer’s AI knows exactly where the gray areas in your contract are, and it exploits them at scale.
To fight this, you need counter-agentic AI of your own. You need a system that understands the contract as well as the payer’s system does, and audits every single transaction—not just the ones that get denied.
The three leakage zones in value-based contracts
In the old fee-for-service (FFS) world, underpayments were relatively easy to spot. If your contract said a Level 3 office visit (99213) pays $100, and you received $85, a basic variance report would flag it.
But in value-based care, the price of a service is fluid. It changes based on the patient’s health, the quality of your documentation, and the performance of your entire network. This complexity creates three massive leakage zones where revenue disappears unnoticed.
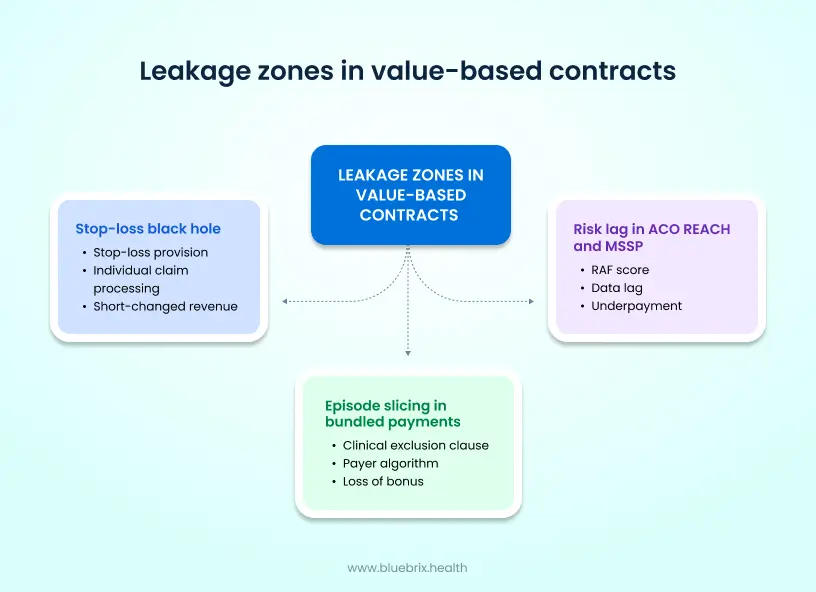
1. The risk lag in ACO REACH and MSSP
In models like ACO REACH or the Medicare Shared Savings Program (MSSP), your reimbursement is heavily tied to the risk adjustment factor (RAF) of your patient population.
- The scenario: You treat Mrs. Higgins, a 78-year-old patient with newly diagnosed diabetes complications and COPD. Your clinical team documents this perfectly in the EMR. Her RAF score should increase to 1.45 to reflect this complexity.
- The leak: The payer’s system operates on a data lag, or fails to ingest the new diagnosis codes from your claim. They continue to pay you a capitated rate based on her previous year’s score of 1.05.
- The result: You are being underpaid by nearly 40% for managing Mrs. Higgins’ care every month. Because the check arrives and clears, your finance team marks it as paid. But you are bleeding revenue on your sickest patients.
2. The episode slicing in bundled payments
If you participate in bundled payment programs (like BPCI Advanced or the new EOM for oncology), you are paid a target price for an episode of care (e.g., a knee replacement + 90 days of recovery).
- The scenario: A patient in a knee replacement bundle gets admitted to the hospital for pneumonia 45 days after surgery.
- The contract: Your contract likely has a clinical exclusion clause. It states that unrelated admissions (like pneumonia) should not be counted against your bundle costs because they are not related to the knee surgery.
- The leak: The payer’s algorithm automatically lumps the pneumonia admission into the bundle, inflating your costs and wiping out your reconciliation payment (the gainsharing bonus).
- The result: You lose your bonus because you failed to catch that the payer included a claim they shouldn’t have.
3. The stop-loss black hole
Most commercial risk contracts have a stop-loss provision. This protects you from catastrophic costs. For example, the contract might say: “If a single patient’s costs exceed $100,000, the payer covers 90% of costs above that threshold.”
- The scenario: A patient has a complex car accident and racks up $250,000 in bills over a three-month period.
- The leak: The payer processes the claims individually. They pay the first $100k, then continue paying the standard rate for the rest, ignoring the stop-loss clause that requires them to pay more (90% of charges) for the catastrophic portion.
- The result: Unless you have a system tracking cumulative patient spend against the specific stop-loss threshold of that specific contract, you will never know you were short-changed $50,000.
The solution: shadow reconciliation (the truth engine)
You cannot solve these problems by hiring more billers. The logic is too complex for human memory, and the volume is too high for manual review.
The solution is a technological strategy called shadow reconciliation (sometimes called Shadow Pricing).
Think of shadow reconciliation as a digital twin of your payer contracts. It is a mirror image of the payer’s adjudication engine, but one that you control.
How it works at blueBriX
At blueBriX, we don’t just process claims; we adjudicate them internally before we even look at the payer’s response.
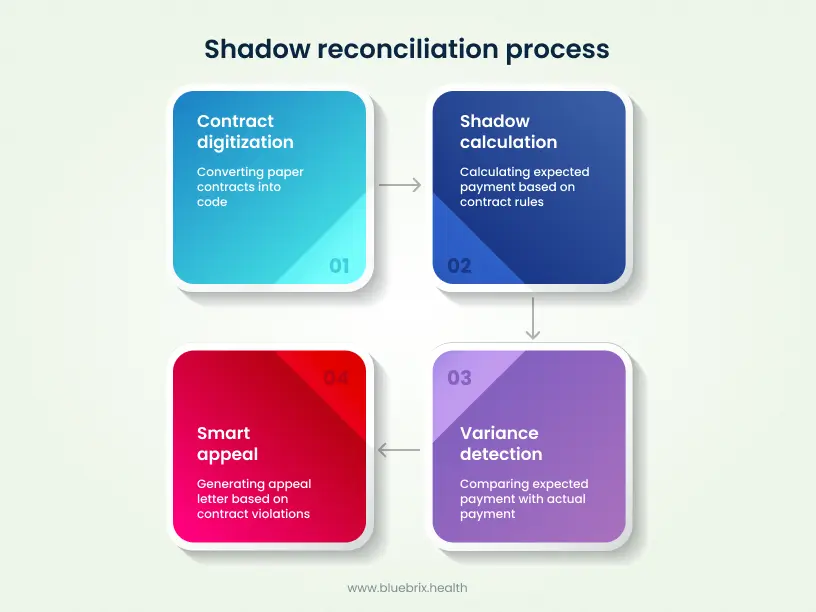
Step 1: Contract digitization
We take your paper contracts—complex PDF documents full of legalese about shared savings, quality gates, and stop-loss limits—and we ingest them into our rules engine. We turn “legal terms” into “code.”
Example: If the contract says “Pay 110% of Medicare rates for Oncology,” our engine learns that rule.
Step 2: The shadow calculation
When you generate a claim or close a month for a capitated population, the blueBriX engine calculates exactly what the payment should be. It accounts for the current RAF scores, the active fee schedules, and the specific patient attributes.
This generates the Expected Allowable.
Step 3: Automated variance detection
When the electronic remittance advice (835) comes in from the payer, our system doesn’t just post the cash. It runs a comparison:
- Payer amount: $450.00
- blueBriX shadow amount: $525.00
- Variance: -$75.00 (Underpayment)
Step 4: The smart appeal
The system flags this variance. But it goes further. Because it knows why the variance happened (e.g., “Payer applied 2024 rates to a 2025 claim”), it can auto-generate an appeal letter citing the specific contract clause that was violated.
Why healthcare leaders need this now
If you are reading this, you are likely in the “Consideration” stage of the buyer’s journey. You know you have a problem. You see your margins shrinking despite volumes growing. You are looking for a solution.
You might be thinking, “Is this worth the investment? Can’t we just focus on denials?”
Here is the hard truth: Denial recovery is expensive. Underpayment recovery is pure margin.
When you fight a denial, you often have to re-submit documentation, get doctors to write letters, and spend hours on the phone. It costs money to get that money.
But recovering an underpayment is different. You have already done the work. The claim is already in the system. You are simply pointing out a math error. The “Cost to Collect” on underpayments is significantly lower than denials, meaning every dollar you recover goes straight to your bottom line.
A case for revenue integrity
Transitioning to blueBriX isn’t just about buying software; it’s about adopting a philosophy of revenue integrity. Revenue cycle is about processing transactions. Revenue integrity is about ensuring you are paid every cent you earned for the value you delivered.
In a Value-based world, where you are taking on risk, you cannot afford to lack integrity in your data. If your risk scores are wrong, you lose. If your quality data isn’t attributed correctly, you lose. If you don’t catch the payer’s math errors, you lose.
blueBriX serves as your shield. Our platform is built on a “Low-Code/No-Code” architecture, which means as payers change their rules (which they do, constantly), we can update your Shadow Reconciliation logic in hours, not months. We don’t need to rewrite the software; we just update the rule.