Across cities in the United States, homelessness and addiction continue to rise side by side. On any given night, hundreds of thousands of people sleep in shelters, cars, or on sidewalks. Many are also living with substance use disorders, untreated mental health conditions, or chronic medical needs.
For this population, care is often fragmented or out of reach. Emergency rooms become the default entry point. Short hospital stays are followed by discharge back to the streets. Detox, treatment, housing, and social services rarely connect in meaningful ways. What should be coordinated care, turns into a cycle of crisis management.
This exposes a deeper issue within U.S. healthcare. The system is built to treat episodic illness, not complex, long-term needs shaped by housing instability, addiction, and behavioral health challenges. As a result, sidewalks become waiting rooms and emergency departments become revolving doors.
Homelessness and addiction are no longer only social service concerns. They represent a growing healthcare crisis that demands new models of care, better care coordination, and stronger accountability for outcomes.
What is the STREETS integrated care program? Inside the new federal homelessness and addiction pilot
The STREETS program (Safety Through Recovery, Engagement, and Evidence-based Treatment and Supports) is a new $100 million federal pilot initiative of integrated care program launched by the U.S. Department of Health and Human Services to address the connected crises of homelessness and substance use disorder across eight U.S. communities.
Led under Secretary Robert F. Kennedy Jr., the program aims to move beyond short-term interventions and build coordinated care pathways for people who are both unhoused and struggling with addiction or serious mental illness.
At its core, STREETS focuses on bringing multiple services together into a single, continuous recovery journey. Instead of relying on emergency rooms, shelters, or law enforcement as isolated touchpoints, the program is designed to connect:
- Street outreach teams that engage people early, before repeated ER visits or incarceration
- Medical and psychiatric stabilization, including evidence-based addiction treatment
- Housing options that support long-term recovery and independence, not just temporary shelter
The goal is to turn episodic street encounters into structured care plans that follow individuals over time.
How STREETS integrated care program differs from past approaches?
STREETS represents a shift in federal strategy. Rather than prioritizing placement alone, the program emphasizes treatment-first recovery models with accountability for long-term outcomes.
Key elements include:
- Outcome-based funding, where providers are measured on sustained housing and reduced relapse, not just initial engagement
- Ownership of the patient journey, assigning a consistent care team or lead organization to support individuals over several years
- Cross-system coordination, bringing together healthcare, housing, social services, law enforcement, and courts to divert people from jail or repeated emergency care into treatment and recovery programs
Another notable aspect is the inclusion of faith-based organizations alongside community providers. These groups are eligible for funding if they meet federal standards, expanding the network of shelters, recovery homes, and counseling programs involved in care delivery.
The pilot is part of a broader recovery-focused federal effort announced under President Donald Trump. It will operate in eight high-need communities as a test of whether integrated, outcome-driven care can more effectively break cycles of homelessness, addiction, and repeated crisis.
In practice, STREETS integrated care program treats the street itself as a starting point for care. Outreach workers, clinicians, housing partners, and social services collaborate to guide people into continuous recovery pathways, replacing fragmented interventions with coordinated, long-term support.
Why traditional behavioral health and homelessness programs fall short?
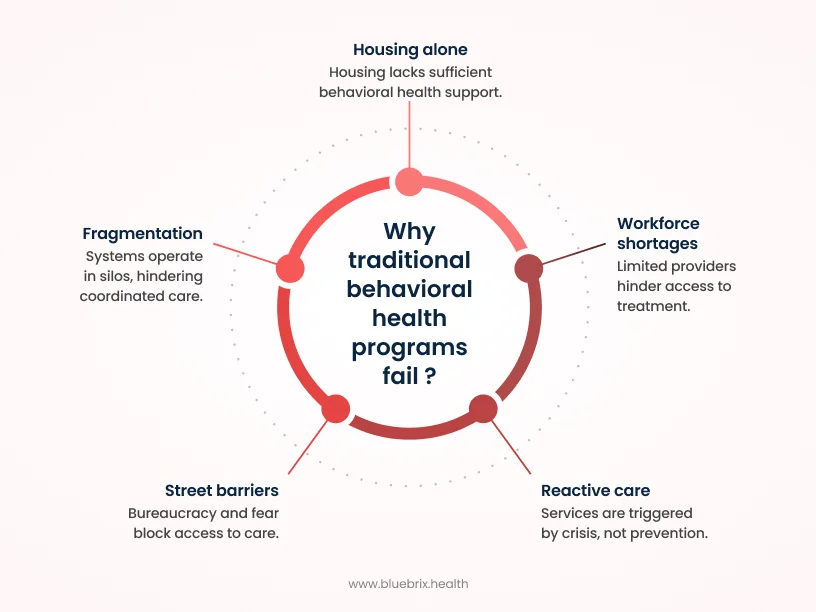
Traditional behavioral health and homelessness programs often struggle because they are fragmented, crisis-driven, and poorly aligned with the realities of life on the street. Instead of creating continuity, they frequently reinforce cycles of relapse, repeated emergency department visits, and short shelter stays.
At the center of the problem is fragmentation
Housing, behavioral health, primary care, and criminal justice systems typically operate in separate silos. Each has its own eligibility rules, funding streams, and data systems. As a result, someone may qualify for housing support but not intensive addiction treatment, or receive brief medical care without access to ongoing behavioral health services. Outreach workers, shelters, and clinics rarely share care plans, which makes it easy for people to fall through the cracks as they move between settings.
Care is also largely reactive rather than continuous
Most services are triggered by crisis, not prevention. Clinics and community mental health centers are often difficult for unhoused individuals to access due to limited hours, paperwork requirements, location barriers, and stigma. Many interventions are short-term, such as a brief detox stay or a few counseling sessions, without sustained case management, medication-supported treatment, or housing coordination. Without long-term support, relapse and return to homelessness are common.
Housing alone is not enough
While housing-first approaches have helped improve placement rates, they have not consistently improved mental health or substance use outcomes. In many programs, housing is provided with minimal behavioral health services. Serious mental illness and addiction remain under-treated. People with the highest clinical needs are often excluded or poorly served because programs lack staff trained to manage complex psychiatric or substance use conditions.
Workforce shortages make the situation worse
Across the U.S., behavioral health providers are in short supply, especially those experienced in caring for homeless populations. This leads to long waitlists, limited access to residential or intensive outpatient programs, and overburdened care teams. Even when people are ready to engage, many never receive evidence-based treatment simply because capacity is not there.
Street-level barriers add another layer of difficulty
For people living outdoors, traditional programs can feel distant and bureaucratic. Lack of insurance, identification, or a stable address blocks access to care. Many also fear judgment, coercion, or legal consequences, particularly when treatment is tied to mandates rather than trust-based engagement.
Taken together, these gaps explain why outcomes remain poor. Housing, addiction, and mental health are treated as separate problems, delivered through disconnected systems. But for people experiencing homelessness, these needs are deeply intertwined. Without integrated, long-term support, traditional models struggle to move individuals out of crisis and into sustained recovery.
How STREETS care program integrates detox, treatment, housing, and workforce support?
The STREETS program is built around a single idea: people experiencing homelessness and addiction should not have to navigate disconnected systems on their own. Instead, detox, treatment, housing, and workforce support are designed to work together as one continuous care pathway. Rather than treating crisis as a one-time event, STREETS connects street outreach directly to medical care, recovery services, and long-term stability.

Detox and medical stabilization
Care often begins on the street. Targeted outreach teams engage individuals where they are and connect them to crisis intervention, detox, and medical stabilization. This includes psychiatric and medical support for people with both substance use disorders and serious mental illness, helping ensure they are clinically stable before moving into longer-term care. The goal is to shorten the gap between crisis and treatment. Mobile and low-threshold services make it possible to start care early, instead of waiting until someone reaches a breaking point or lands in the emergency department.
Treatment and recovery-focused care
Once stabilized, STREETS prioritizes recovery-oriented, evidence-based treatment rather than short detox stays or isolated counseling sessions. This includes:
- Medication-assisted treatment and counseling delivered through clinics, community providers, and recovery programs
- Longer-term engagement models, where providers are expected to support individuals for years, not just during a brief rehab episode
- Participation from faith-based and community organizations, expanding access to peer-driven and spiritually informed recovery support
Importantly, funding is tied to sustained recovery outcomes. This shifts incentives away from repeated admissions and toward long-term progress, encouraging providers to focus on relapse prevention, continuity of care, and real-world stability.
Housing with a recovery focus
Housing under STREETS is not treated as a standalone solution. Participants are connected to recovery-oriented housing that supports independence and sobriety, such as sober living or treatment-linked housing, rather than temporary shelter alone. Housing is integrated with ongoing clinical care, so residents can access counseling, medication support, and case management without navigating multiple disconnected locations. This approach moves away from traditional housing first models by tying housing more closely to treatment participation. While this has raised concerns about serving the most complex cases, the intent is to align housing with sustained recovery rather than short-term placement.
Workforce and system support
STREETS also invests in the people delivering care. Funding is used to expand capacity among community and faith-based providers already serving homeless populations. Programs are encouraged to build integrated care teams that may include outreach workers, clinicians, case managers, and peer recovery specialists, all coordinating around the same individuals. Outcome-based payment models push organizations to strengthen training, supervision, and data systems so they can track housing stability, recovery progress, and reductions in emergency room visits or incarceration over time.
In practice, STREETS brings detox, treatment, housing, and workforce development into one coordinated system. Outreach on the street leads directly into stabilization, then into recovery-focused housing and ongoing support, all connected by accountability for long-term outcomes.
What STREETS integrated care program means for health systems, community providers, and public agencies?
For health systems, community organizations, and public agencies, STREETS represents both an opportunity and a pressure point. The program brings new funding and momentum for integrated homeless and addiction care, but it also raises expectations around coordination, accountability, and long-term outcomes. Participation is not just about delivering services. It requires organizations to rethink how care is designed, tracked, and sustained.
For health systems: earlier engagement and outcome accountability
Hospitals, clinics, and health plans are being pushed upstream. By funding street outreach and early stabilization, STREETS encourages health systems to intervene before people cycle repeatedly through emergency departments and inpatient units. The focus shifts from crisis response to proactive engagement.
At the same time, health systems partnering with STREETS-supported providers may face new performance expectations tied to outcomes such as housing stability, reduced relapse, and fewer emergency visits. This can influence how discharge planning, case management, and street medicine programs are structured.
Clinics are also likely to play a larger role in coordinating with mobile outreach teams. Instead of discharging patients back to the streets with limited follow-up, systems are expected to share data and connect individuals directly into STREETS care pathways.
For community providers: expanded scope with higher expectations
Community-based organizations, behavioral health agencies, and faith-based recovery programs gain access to federal funding specifically targeted at integrated homelessness and addiction care. This creates opportunities to scale outreach, medication-assisted treatment, recovery housing, and peer support.
However, STREETS also pushes providers toward recovery-focused models. Many organizations may need to strengthen structured treatment tracks, sober living options, and longer-term engagement strategies, moving beyond short detox stays or low-intensity counseling alone.
With that comes greater accountability. Grantees are expected to track and report outcomes such as housing retention, sobriety, and reduced ER or jail use. For smaller organizations, this can strain operational capacity, but it also creates a clearer way to demonstrate impact to payers and policymakers.
For public agencies: shared responsibility across systems
City and county governments, public health departments, housing agencies, law enforcement, and courts are being asked to work together more closely than before. STREETS explicitly calls for multi-agency teams, which means formalizing shared data, referral pathways, and care protocols instead of operating in silos. Housing authorities may be encouraged to prioritize recovery-oriented or sober housing for participants, even when this challenges traditional Housing First approaches.
Law enforcement and courts are also expected to play a different role. Rather than defaulting to citations or incarceration, agencies may divert more people into STREETS-linked treatment and housing programs. While this can reduce criminal justice costs, it also raises important questions about consent, coercion, and civil liberties.
A system-wide shift
Taken together, STREETS asks all three sectors to treat homelessness and addiction as a shared responsibility. More resources are flowing toward integrated, outcome-driven models. In return, organizations are expected to coordinate across boundaries, share data, and commit to long-term recovery success rather than short-term service delivery. For many communities, this represents a meaningful shift: from fragmented interventions to a collective approach focused on stability, treatment, and sustained change.
Care coordination, compliance, and reporting requirements under STREETS integrated care program
Under STREETS, care coordination, compliance, and reporting are designed to ensure people move through a continuous and accountable pathway, from street outreach to treatment and stable housing. While detailed program rules are still emerging, early guidance and existing federal behavioral health frameworks point to clear expectations around coordination, standards of care, and measurable outcomes.
Care coordination: one journey, one accountable team
A central principle of STREETS is that one team or lead agency “owns” each participant’s care journey. In practice, this means grantees are likely expected to assign a dedicated care coordinator or case manager who conducts comprehensive needs assessments across housing, medical, behavioral health, legal, and employment domains. Coordinators then develop individualized service plans with clear short- and long-term goals, such as detox, medication-assisted treatment, housing placement, and workforce engagement.
Care teams must coordinate across multiple settings, including:
- Street outreach and mobile care teams
- Emergency departments, primary care clinics, and behavioral health providers
- Shelters, housing authorities, and recovery-oriented housing programs
Transitions between settings, such as moving from detox into residential treatment or from shelter into permanent housing, are expected to include warm handoffs, shared records, and follow-up visits to reduce drop-off. Importantly, coordination is meant to be trauma-informed and street-accessible. Rather than forcing people into clinic-centered workflows, programs are encouraged to use mobile and low-threshold models that meet individuals where they are.
Compliance: federal standards with real oversight
Compliance under STREETS centers on meeting federal grant requirements, clinical standards, and civil rights protections. Programs must target people experiencing homelessness who also have substance use disorders or serious mental illness, and services are expected to be evidence-based, including medication-assisted treatment, trauma-informed care, and recovery-oriented practices.
Housing placements must meet minimum safety, health, and recovery-support standards, while detox and treatment providers must follow state licensing and accreditation rules for behavioral health services. Grantees are also expected to comply with civil rights requirements, including non-discrimination and reasonable accommodations for people with disabilities or limited English proficiency.
From a financial perspective, organizations must demonstrate proper use of federal funds, maintain clear cost allocation, and participate in audits or monitoring visits. If performance or compliance falls below expectations, corrective action plans may be required.
Reporting: shifting the focus to outcomes, not volume
STREETS is explicitly outcome-driven. Reporting will focus less on how many people were served and more on whether lives are actually stabilizing. Core metrics are likely to include:
- Housing outcomes, such as the percentage of participants who secure stable housing and how long they remain housed
- Substance use and behavioral health outcomes, including engagement in ongoing treatment and reductions in use
- Health system utilization, such as changes in emergency department visits, hospital admissions, and ambulance use
- Justice system involvement, including reductions in arrests or jail days
Beyond outcomes, programs will also need to submit activity data, such as:
- Street-level contacts, assessments, and referrals
- Time from outreach to detox, treatment, or housing placement
- Demographic and clinical profiles to monitor equity and targeting
Reporting will follow a tiered schedule, with quarterly or biannual performance reports, annual or mid-term evaluations, and data submissions to federal systems that support cross-site analysis and national learning.
The role of data integration and interoperability in homelessness and addiction care
Data integration and interoperability are central to STREETS’ promise. Without shared, real-time information across health, housing, and social service systems, the program risks repeating the same fragmented, episodic care patterns that have long failed people experiencing homelessness and addiction. STREETS is built around continuous, accountable care. That vision only works if different agencies can see and act on the same information.
Why data integration matters for STREETS integrated care program
STREETS aims to “own” a person’s journey from street outreach through detox, treatment, and housing. To do that, teams must be able to see the full story. Today, the same individual may appear in:
- An emergency department record
- A Homeless Management Information System entry
- A behavioral health clinic’s electronic health record
But these systems rarely connect. Each encounter feels like a first-time visit, even when it is part of a long pattern of instability. Integrated data changes this. It allows STREETS teams to avoid redundant assessments, reduce paperwork, and quickly identify who is at highest risk, what services they have already accessed, and where gaps remain. Instead of starting from scratch at every touchpoint, providers can build on prior interventions.
Interoperability across health, housing, and justice
For STREETS to function as designed, cross-sector data linkages are essential. This includes connecting:
- Health system EHRs with homeless response systems and addiction treatment records
- Law enforcement and court data with health and housing systems, so patterns of arrest, citations, or jail stays are visible and can trigger earlier intervention
In practice, this could take the form of a common, person-centered record updated in near real time as someone moves from outreach to detox to housing. Coordinated-entry lists or by-name dashboards can help teams track housing status and service engagement in one shared view.
Case conferencing tools are another example. Hospital navigators, housing case managers, and STREETS coordinators can review the same data and jointly decide next steps, instead of working from disconnected notes and assumptions.
Privacy, governance, and practical barriers
Interoperability must balance usefulness with privacy and trust. Behavioral health and substance use data are especially sensitive. Federal and state regulations such as HIPAA, Homeless Management Information System confidentiality rules, and 42 CFR Part 2 require strong data-sharing agreements, clear consent protocols, and appropriate safeguards.
Some communities are experimenting with “honest broker” models, where a neutral entity links datasets while protecting individual identities. Approaches like this may become important tools for STREETS implementation.
There are also practical barriers. Systems often use different data standards and definitions, for example how homelessness status is recorded in an EHR versus a housing system. Smaller community providers may lack the IT capacity or funding to implement interoperable platforms without additional support.
Interoperability as the backbone of accountability
STREETS is explicitly outcome-driven. That makes interoperability more than a technical upgrade. It becomes the backbone of care coordination and performance reporting. Care coordination dashboards can show, in one place, a person’s recent emergency department visits, housing status, treatment enrollment, and relapse history. This allows teams to adjust care plans proactively rather than waiting for another crisis.
At the program level, linking health utilization data with housing and treatment records enables more accurate measurement of long-term outcomes such as housing retention, reduced emergency visits, and fewer arrests. This moves evaluation beyond self-report and fragmented data silos.
In short, data integration and interoperability are the infrastructure that make STREETS possible. They allow outreach workers, clinicians, housing providers, and public agencies to function as one coordinated team around the same individual, rather than as disconnected actors who never see the full picture.
Technology infrastructure for scaling integrated public health programs
Scaling integrated public health programs like STREETS depends on having a strong, interoperable technology backbone. Without it, even well-designed care models break down as data becomes siloed, referrals stall, and accountability fades. At a minimum, STREETS-style programs require a connected digital ecosystem that brings health systems, behavioral health providers, housing agencies, and public health organizations into the same operational picture.
Core components of the infrastructure
A modern integrated-care stack typically includes:
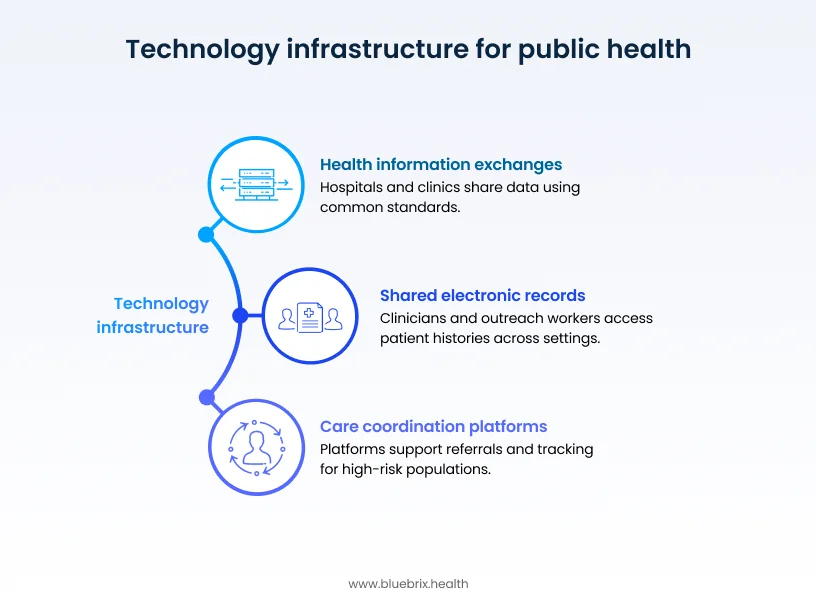
- Shared electronic records and interoperable EHRs, so clinicians, outreach workers, and case managers can see a person’s history across settings, from emergency department visits to housing placements.
- Health information exchanges (HIEs) or regional data platforms that connect hospitals, community clinics, behavioral health agencies, and homeless response systems using common standards such as FHIR and HL7.
- Care coordination and
case management platforms that support referrals, warm handoffs, follow-ups, and longitudinal tracking for high-risk populations like people experiencing homelessness and addiction.
This infrastructure must also be cloud-enabled and flexible. National or state standards need to coexist with local workflows, while new tools such as telehealth, mobile outreach apps, or AI-driven risk stratification should be able to plug in over time without disrupting care delivery.
Governance, standards, and privacy
Technology alone does not create integration. Governance does. Sustainable programs depend on shared data-sharing agreements, consent frameworks, and de-identification protocols that protect sensitive substance use and homelessness data while still allowing care teams to coordinate effectively.
Open standards and APIs are equally important. They prevent communities from being locked into proprietary systems and make it possible for different vendors and agencies to work together. This becomes critical when linking clinical care with housing, outreach, and justice system data.
The role of blueBriX
In this environment, platforms such as blueBriX can act as a central operational hub for integrated public health programs. Rather than forcing organizations to stitch together multiple disconnected tools, unified platforms can:
- Ingest and normalize data from EHRs, behavioral health systems, and Homeless Management Information Systems, creating real-time dashboards that track housing status, treatment engagement, and health system utilization.
- Support automated workflows and alerts, such as flagging when someone is discharged back to the streets or triggering a warm handoff to outreach or street medicine teams.
- Embed care coordination logic, compliance checks, and reporting templates directly into daily workflows, helping organizations meet STREETS’ outcome-driven requirements without rebuilding processes from scratch.
This turns interoperability from a technical goal into an operational reality.
Turning infrastructure into impact
At scale, the right technology foundation allows STREETS programs to move from reactive crisis management to proactive, coordinated care. Outreach workers, clinicians, housing staff, and public agencies can operate from the same data, follow the same care plans, and measure progress against shared outcomes.
In short, the infrastructure behind STREETS must be interoperable, standards-based, and governance-aware. With platforms like blueBriX serving as connective tissue, fragmented data becomes coordinated, person-centered care, making it possible to deliver on the program’s promise of long-term recovery and stability.