A resident enters your PRTF, steps down to RTC, moves to a group home, and discharges to outpatient. Four levels of care, one organization, nine months. Somewhere in those transitions, their chart fragments, two days of billing disappear, and a surveyor asks a question your EHR can’t answer in under an hour. None of this is a documentation problem. It is an EHR problem.
That sequence is the buying decision. Not the demo. Not the price. Whether your platform holds the thread across programs or drops it that’s what you’re actually choosing. This guide covers the four capabilities that decide it, the eight categories to score vendors on, and the test scenarios that surface the truth before you sign.
The 5 multi-program EHR buying problem you should not miss
Most EHR guides assume you are buying for one program type. PRTF as a standalone facility, or outpatient as a standalone clinic, or RTC as a standalone center. Real multi-program organizations are not built like that. You run PRTF beds and an RTC unit on the same campus. You have a group home down the road. You have an MST team in the community. You step residents down through your own continuum because that is what produces good outcomes and that is what your funders expect.
That structural reality changes the buying decision in five specific ways.
- Residents move, but records often do not. A young person in your care will likely move between programs at least once during their treatment arc. The EHR either treats this as a normal workflow or treats it as an exception that requires manual intervention. Most generic behavioral health systems treat it as an exception. You can tell because the moment a level of care changes, somebody on your team starts opening spreadsheets.
- Documentation standards differ per program, under one roof. PRTF requires a Certification of Need, a federally defined active treatment plan, and structured restraint and seclusion documentation. QRTP under FFPSA has its own standards. Group homes operate under state licensing rules that look nothing like PRTF Conditions of Participation. Your EHR has to produce all of it correctly, simultaneously, on the same residents.
- Billing model fragmentation is brutal. PRTF is per-diem. RTC may be per-diem at a different rate, or bundled, or carved out depending on the state. Group homes are often fee-for-service. Some payers pay capitated rates for emergency beds. Some pay hold-bed rates when a resident is temporarily at a hospital but the bed needs to be reserved. The number of organizations rebuilding per-diem claims in spreadsheets every month because the EHR cannot handle bed-day logic is much higher than vendors will admit.
- Shared staff means fractured credentialing. Your psychiatrist covers PRTF and PHP. A therapist works across the RTC and the group home. The EHR has to track which credentials apply where, which notes are co-signed by whom, and which programs each provider can document in. If it cannot, you end up managing this in a side system that drifts out of sync.
- Reporting runs in two directions. Each program reports out to state agencies under different rules. Leadership reports up across programs because that is how the organization is actually run. A platform that does one well and the other badly will frustrate someone important every quarter.
Why is this decision time-sensitive?
The buying decision is not just about your current operations. Three policy and reimbursement shifts converging in 2025 and 2026 raise the cost of staying on a misfit EHR and shorten the runway for organizations that have been deferring the decision.
- FFPSA and QRTP enforcement is no longer notional. The Family First Prevention Services Act has been in effect for several years, but state implementation timelines have stretched, and many residential organizations have been operating under transitional arrangements. Those transitional periods are closing. QRTP designation, the 30-day assessment requirement, family engagement documentation, and aftercare planning are now being audited in earnest, with title IV-E funding tied directly to compliance.
- Medicaid managed care contracts are tightening on per-diem documentation. State Medicaid agencies and the managed care organizations they contract with are moving from retrospective denials toward prospective documentation requirements. Billable days with incomplete documentation, hold-bed claims without proper authorization, and per-diem rates applied to days where the level of care was not properly justified are being scrutinized at claim submission rather than during annual audits.
- 42 CFR Part 2 alignment with HIPAA changes how SUD records flow across programs. Recent rule changes have brought 42 CFR Part 2 closer to HIPAA for treatment, payment, and operations purposes, but the controls around consent, redisclosure, and segmentation of SUD records have become more structurally demanding. Multi-program organizations with SUD treatment in part of their continuum need an EHR that handles Part 2 controls as built-in workflow.
The compound effect is that the gap between PRTF-native platforms and retrofitted behavioral health systems is widening every quarter. An evaluation deferred to 2027 is an evaluation conducted under more pressure, with more accumulated workarounds to migrate, and against a regulatory backdrop that will have moved further. The organizations making the decision deliberately in this evaluation cycle are buying themselves runway.
4 must-have capabilities for a PRTF EHR
Most EHR platforms can demo well enough to look credible. The real question is whether they hold up on the four capabilities where mediocrity equals failure. If a platform can’t show these cleanly in a structured demo, nothing else in the conversation matters.
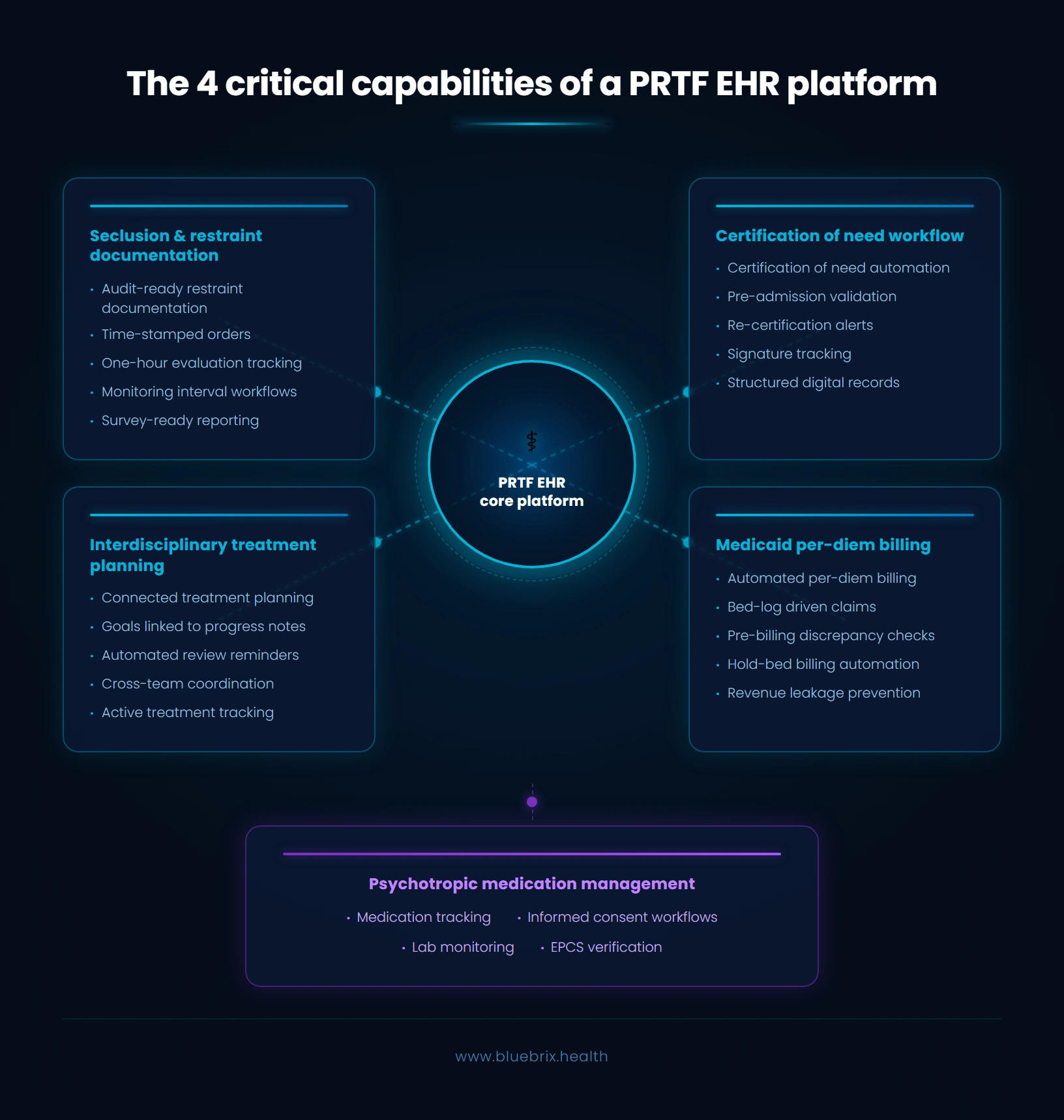
Seclusion and restraint documentation that holds up under audit
This is the single biggest survey risk for PRTF operators, and the federal requirements are unforgiving. Every episode needs a time-stamped order from a licensed practitioner within a specific window, documentation of less-restrictive interventions attempted first, the one-hour in-person evaluation, monitoring intervals during the episode, the debriefing afterward, and guardian notification.
What you should demand in a demo is a structured workflow where each of those elements is a discrete field with required-entry logic, not a free-text incident note where the staff member is expected to remember everything. You also want to see staff documenting the episode in real time on a tablet or phone, not retrospectively at a desk twenty minutes later. The morning a state surveyor asks for restraint documentation on a specific resident from three months ago, the report should produce itself in under a minute.
Certification of Need workflow with timing logic built in
The CON is the document that authorizes PRTF-level care under Medicaid. It needs the right signatures, it needs to be completed before admission, and it needs re-certification at defined intervals. A platform that handles this well surfaces the re-certification deadline before it lapses, tracks the signing team, and produces the CON as a structured record.
Interdisciplinary treatment plan with goals linked to progress notes
The federal rule requires an active treatment plan developed by an interdisciplinary team, reviewed at defined intervals, with goals tied to the reason for admission. The platform should treat the plan as connected data, not a static document. A therapist’s progress note should be able to reference a specific treatment plan goal. Treatment plan reviews should appear in clinician workflows before they’re overdue, not after.
This is one of the areas where blueBriX does something many platforms don’t: review deadlines surface seven and two days before they expire, so the clinical team acts on them inside their normal workflow rather than reacting to a compliance report after the fact.
Medicaid per-diem billing without the workarounds
Ask any PRTF billing manager what their monthly close looks like and you’ll hear about the workarounds. The spreadsheets pulled from the bed log, manual reconciliation against the EHR’s encounter data, days where the patient was there but the documentation wasn’t completed in time, hold-bed billing handled outside the system entirely because the EHR can’t model a bed without a patient assigned, capitated emergency bed contracts where the biller assigns the entire monthly payment to one patient and then manually redistributes it.
Every one of those workarounds is a revenue leak, a compliance risk, and a staff retention problem. Your billing team didn’t take this job to maintain spreadsheets. What good looks like: per-diem, hold-bed, and capitated claims generate directly from the bed log, with the bed log as the source of truth. Patient-level rate exceptions are configured on the fee sheet once, not re-entered per claim. A pre-billing scrub layer surfaces discrepancies between the bed log and the documentation before claims go out. blueBriX automates this end-to-end, so your billers review claims rather than rebuild them from scratch.
A note on the fifth capability that often gets bundled into this discussion: psychotropic medication management — informed consent for minors, AIMS screening, lab monitoring, and EPCS support for controlled substances. The requirements here are well understood and most serious behavioral health platforms handle them adequately. The four above are where platforms quietly fail.
See blueBriX in action
If your evaluation is at the point where you are tired of generic demos and want to see what a PRTF-native EHR actually does with per-diem billing, bed management, and survey-ready compliance, book a 30-minute scenario-based demo. Bring your billing lead, your clinical director, and your admissions coordinator. We build the session around your program mix.
Schedule a demo8 questions that help you to choose between PRTF EHRs
The four non-negotiables get a platform onto your shortlist. These eight questions are how you choose between the platforms that made the cut.
1. Do the clinical workflows scale across levels of care, or are they locked into one model?
This matters because most PRTF operators don’t run just a PRTF. You likely have outpatient programs, group homes, or step-down units sharing the same EHR. If the only treatment plan model in the system is the PRTF interdisciplinary plan, your outpatient and group home staff will fight it every day. If the only model is the outpatient plan, your PRTF won’t meet federal requirements.
What to look for: Treatment plan templates that are configurable per program, while assessments and history flow forward across programs without re-entry. One resident, one chart, multiple program contexts.
2. Can your direct care and milieu staff actually use it on a tablet at 2 a.m.?
This is the category most underrated by buyers and most consequential after go-live. Your direct-care staff aren’t clinicians, aren’t fast typists, and are often working overnight shifts on tablets. If the system is slow or punitive for them, two things show up in the data within ninety days: incident documentation gaps and milieu staff turnover.
In demos, watch how long it takes a staff member to enter a behavioral observation, document an incident, or complete a shift handoff. Count the clicks. Ask whether they can document a restraint while it’s happening or only afterward. If the answer is “afterward,” the platform was designed for clinicians, not for the people who actually run the milieu.
3. Can the platform produce survey-ready reports on demand, without engineering work?
PRTF surveys are the hardest test, but the platform also needs to handle RTC licensing, group home regulations, Joint Commission, CARF, and COA standards. The morning a surveyor walks in, the platform should produce on demand: a restraint and seclusion summary, a treatment plan compliance report, a medication administration variance report, an incident report by type and resolution, and the active CONs with upcoming re-certifications.
If any of those reports require a vendor ticket or a developer to build, the platform isn’t really PRTF-native, it’s a general behavioral health system with a PRTF skin.
4. How does billing behave when a resident’s level of care changes mid-stay?
Per-diems are covered in the non-negotiables. The cross-program lens is different: what happens when a resident steps down from PRTF to group home on the 14th of the month, how the system segments billing across multiple programs and payers in a single stay, and whether documentation completeness is checked before claims go out rather than after.
The truth test: can you run a report showing days billed with incomplete documentation before the claims leave the system? If the only way to find that out is a denial three weeks later, the revenue cycle is reactive by design.
5. Is reporting self-serve, or does every new question require a vendor ticket?
Two layers matter. Program-level dashboards that match how each program is regulated and what a PRTF director needs to see is not what a group home director needs to see. And organization-level rollups that let leadership see across the continuum. Both layers need to be self-serve. If every new report or filter requires a vendor ticket, your analytics function is in trouble before it starts. Ask in the demo to build a report you didn’t pre-arrange and see what happens.
6. Does the platform handle the on-site school and ancillary services, or treat them as afterthoughts?
Most PRTFs run an on-site school, and this is often where buyers get surprised post-purchase. The EHR should either house IEP information directly or integrate cleanly with the school’s system, and that data needs to travel with the resident as they move across programs. Recreational therapy, dietary, and other ancillary documentation usually live here too and they usually live badly if the vendor treated them as a checkbox.
7. Can the system track who actually has signing authority, given how often that changes?
Guardianship changes are common in this population. A resident enters in state custody, parental rights get terminated mid-stay, or a court-ordered placement shifts the picture entirely. The system needs to track who has signing authority for which decisions and route consent forms accordingly as a structured data that drives workflow. The portal experience for young people should be designed around the guardian as the primary contact, not the patient, with the flexibility to flip that as the resident ages or as legal status changes.
8. What does the data export look like if you ever leave?
This is where the IT and integration gatekeeper earns their keep. The right questions are: what’s the platform’s posture on HL7 and FHIR, what HIE integrations are live in your state, what’s the clearinghouse story for your payer mix, and the one that separates confident vendors from nervous ones like what does the data export look like if you ever leave? That last question is the truth test. Vendors who are confident about their product answer it directly. Vendors who aren’t, don’t.
For reference: blueBriX supports HL7 and FHIR natively, integrates with major clearinghouses through implementation, and gives you an open API for downstream BI and analytics. CCDA sharing is supported, and 42 CFR Part 2 controls are built in for any program where they apply.
What are the most common mistakes when buying a PRTF EHR?
A few patterns show up often enough to flag explicitly.
- The first is buying on PRTF features and discovering the RTC workflow is an afterthought. The opposite mistake is buying on outpatient ease and forcing PRTF to fit is more common but easier to spot.
- The second is underestimating direct-care staff usability. Buyers tend to over-index on what they see in their own role.
- The third is assuming “behavioral health EHR” means “PRTF-ready.” The market uses the same words for very different products.
- The fourth is letting one function drive the decision alone. The billing lead, the clinical director, and the IT gatekeeper need to agree, because each can sabotage implementation if they did not see their concerns addressed.
- The fifth is skipping the data migration and exit conversation. Get the exit terms in writing before you sign, not after.
- The sixth is treating implementation as a vendor problem rather than an organizational change problem. Even a well-built platform fails if the organization does not invest in adoption.
Picking the right EHR setup for your programs
The architectural question sits underneath the platform question. There are three honest paths.
A single unified platform across all programs suits multi-program organizations that want one patient record, one set of credentials, and one place where the data lives. Trade-off: you need a platform that genuinely handles every program well, which is rarer than vendors suggest. This is the path blueBriX was built for, with PRTF, QRTP, MST, group homes, and bridge programs running on one patient record with program-level access controls that keep PRTF staff in PRTF records and MST staff in MST records.
A PRTF-specialized EHR plus separate systems for other programs suits organizations where PRTF compliance dominates and the other programs are small or operationally independent. Trade-off: you carry the cost of integration between systems and the friction of resident transitions between them.
A best-of-breed stack with integration suits sophisticated organizations with the IT capacity to maintain it. Trade-off: integration complexity is permanent, not a one-time implementation cost.
How to tell which path fits: count the residents who move between your programs in a year. If the number is meaningful, the unified platform path is usually right. If your programs are mostly serving different populations with little crossover, the specialized-plus-separate path may work.
Why blueBriX for multi-program residential behavioral health?
Most behavioral health EHRs were built for one program type and stretched to cover the others. blueBriX was built the opposite way, designed from the start for organizations running PRTF alongside QRTP, RTC, MST, group homes, and step-down programs on a single patient record. Here is what that looks like in practice.
- One patient record across the continuum. A resident who moves from PRTF to RTC to a group home to outpatient keeps one chart, one medication history, one treatment arc.
- Per-diem billing automated from the bed log. Per-diem, hold-bed, and capitated emergency-bed claims generate directly from the bed log as the source of truth. A pre-billing scrub layer surfaces documentation gaps before claims go out, not three weeks later as denials. Billing teams review claims rather than rebuild them in spreadsheets every month.
- Survey-ready compliance built into daily workflow. Structured seclusion and restraint documentation with required-entry logic, tablet-first capture for direct-care staff documenting in real time, Certification of Need workflows with re-certification alerts at seven and two days, and treatment plan reviews that surface in clinician workflows before they lapse.
- Predictive crisis AI on the single record. Because every program runs on one patient record, behavioral patterns across milieu observations, medication changes, restraint episodes, and progress notes feed a single signal. Clinical teams see escalation risk earlier, not in a separate analytics product.
- Open by design. HL7 and FHIR supported natively, integrations with major clearinghouses, an open API for downstream BI and analytics, CCDA sharing, and 42 CFR Part 2 controls for programs where they apply.
If the framework in this guide describes the decision you are making, blueBriX is built for it.