You delivered the care. The claim paid. You moved on.
Then the remittance came in short by $10,000, $40,000, sometimes $300,000, referencing claims from two years ago that nobody on your team remembers.
This is not a denial. Denials you can manage. They show up the next morning, you work them, fix them, resubmit. This is a recoupment. By the time it lands on your desk the documentation is archived, the clinical team has moved on, and the payment has long since been absorbed into your numbers.
And the lookback window is longer than most teams budget for. Three, four, sometimes six years of paid revenue sitting inside that window. That is not a billing problem. That is a balance sheet risk hiding in plain sight.
Getting paid is only half the job. Staying paid is the other half.
In this blog we break down exactly where that revenue is at risk, which audit triggers are most likely to affect your organization, and how blueBriX builds the infrastructure to make audits a non-event.
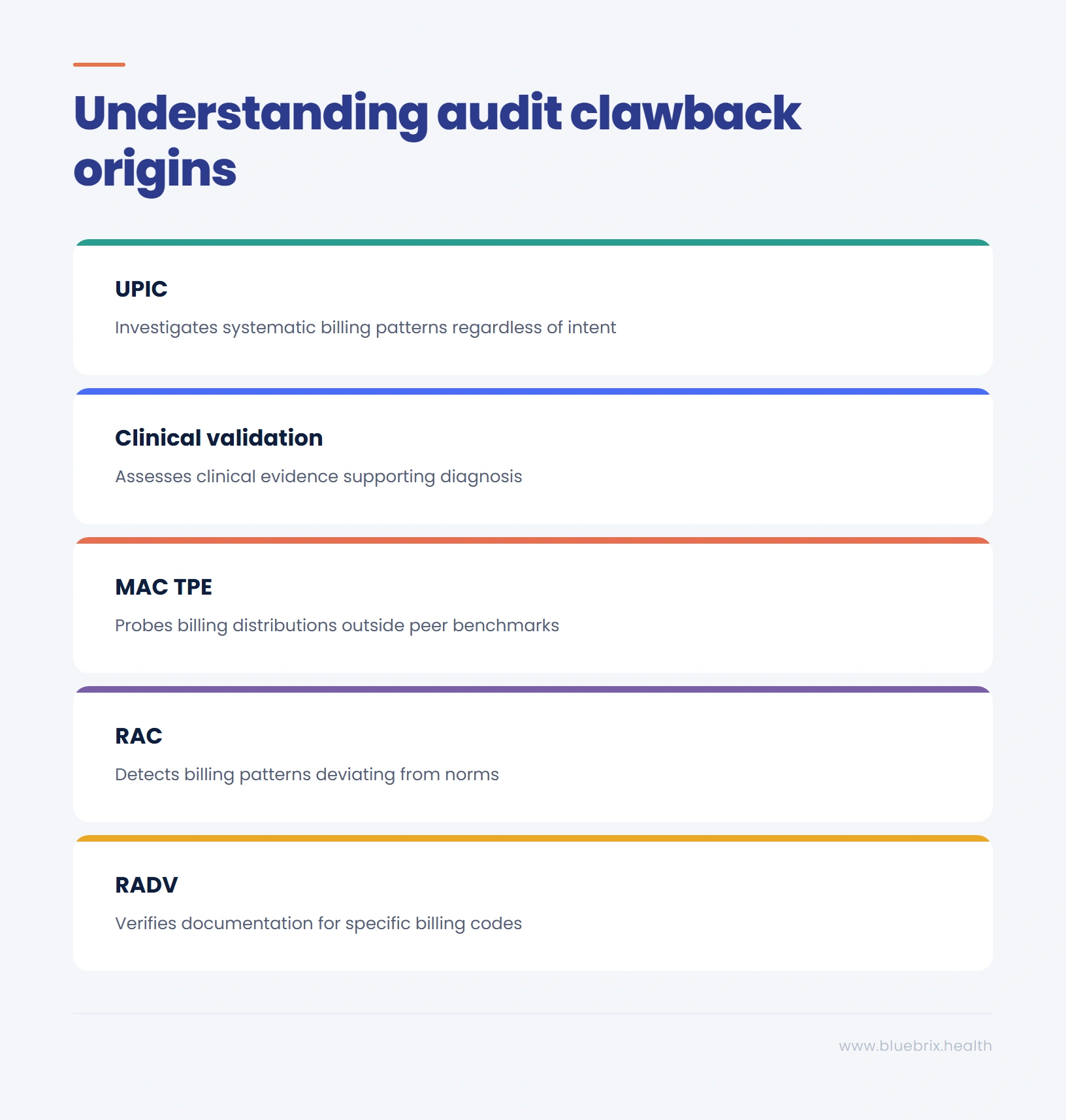
Mapping the threat: every clawback has an audit parent
One of the most important things to understand about retrospective recoupments is that they are not random. Every clawback originates from a specific audit type, and every audit type is looking for a specific class of error. When you know the source, you can close the gap before the auditor ever arrives.
RADV: When an HCC code cannot survive a chart pull
RADV (Risk Adjustment Data Validation) auditors are not questioning whether the diagnosis was clinically correct. They are asking something narrower: is there a signed note, from a face-to-face visit, where this condition was actively addressed and documented specifically enough to match the billing code?
Where revenue typically becomes recoverable:
- No active management documented: A condition that appears in the record as background context rather than something monitored, evaluated, or tied to a clinical decision during that visit. That is where the code reverses and the payment disappears.
- Missing or incomplete physician note: A signed note from a face-to-face visit is non-negotiable. If the signature is missing, the date is absent, or the note is too vague to link the condition to the visit, the code has no foundation to stand on.
- Diagnosis not specific enough: The documented diagnosis does not match the specificity required by the billing code. A general reference to a condition is not the same as a documented, addressable diagnosis.
With RADV now expanded to cover all 550+ Medicare Advantage plans annually and audits running for payment years 2018 through 2024, the exposure has grown significantly. The documentation rules have not changed. The reach has.
RAC: when a legitimate billing pattern looks like a statistical anomaly
The trigger is rarely a single claim. It is a distribution. An inpatient admission rate slightly above regional peers. A procedure volume edging past a statistical threshold. A code appearing regularly in your billing history that CMS has already flagged nationally.
Where revenue typically becomes recoverable:
- Admission status: A patient admitted inpatient where the clinical picture on paper could have supported observation status. The reimbursement gap between those two designations is significant and it is one of the first places RAC (Recovery Audit Contractors) contractors look.
- Missing clinical reasoning: A physician note that documents what happened but not why that level of care was necessary. The signs, the risks, the decision behind the admission without those the note cannot defend the claim.
- Missing physician order: A procedure billed correctly with no signed physician order in the record. The care happened, the billing was accurate, but without the authorization trail the claim has no foundation.
- Unbundling: Services billed separately that should have been grouped under a single code. RAC contractors know every unbundling pattern and look for it specifically.
- Code and note mismatch: A diagnosis or procedure code that does not line up with what the physician actually documented. Even a small inconsistency between the code and the note is enough for the claim to become recoverable.
MAC TPE: when your billing distribution crosses a threshold
MAC TPE (Targeted Probe and Educate) probes are not triggered by something going wrong. They are triggered by something looking different.
If your Level 5 visit rate, procedure frequency, or diagnosis distribution sits outside regional peer benchmarks even marginally, the MAC’s systems flag it automatically. No complaint, no tip. Just a pattern that crossed a threshold.
What the probe typically surfaces:
- Level mismatch: A note billed at Level 5 where the documented complexity reads closer to Level 3. The billing reflected the care delivered but the documentation did not capture it at the level needed to support that billing code.
- Copy-paste documentation: Notes that look identical across multiple encounters regardless of what actually happened on each day. When every note tells the same story a reviewer cannot distinguish one encounter from another. That is when documentation loses its ability to defend the billing.
- Time not recorded: Time-based billing where the time spent was never documented in the note. Without it in the record the higher level simply cannot be supported.
And what makes TPE particularly serious is the escalation path:
- High error rate in round one leads to round two.
- Persistent findings trigger prepayment review.
- Every future claim gets held manually before any money is released. Cash flow stops.
Clinical validation audits: when the clinical story does not match the claim
A physician or nurse hired by the payer reads your record and asks one question. Does the clinical picture like vitals, labs, treatment decisions, and narrative tell the story of a patient who warranted this diagnosis?
The coding can be technically correct. The paperwork perfectly in order. What gets scrutinized is whether the record, read as a clinical document, supports the diagnosis being billed.
Where this creates exposure:
- Conflicting clinical evidence: A high-value diagnosis billed where the clinical evidence points in a different direction. Sepsis documented alongside near-normal vitals, no identified infection source, no evidence of organ stress. The treating physician’s judgment may have been sound but if the record does not carry that story the diagnosis gets reversed.
- Condition not actively managed: A condition present in the chart that was not engaged during that encounter. If it was not monitored, evaluated, or treated during that specific visit it does not qualify for billing on that claim.
- Missing supporting evidence: A physician note referencing a test result or consultant finding that is not present in the record being reviewed. If the auditor cannot see it, it does not exist for the purposes of that audit.
These are high-value codes by definition. A single Sepsis reversal can represent several thousand dollars on one claim.
UPIC: when the pattern looks systematic regardless of intent
UPIC (Unified Program Integrity Contractor) investigations are a different category entirely. These are not documentation reviews or billing level assessments. They are pattern investigations with the authority to freeze all incoming Medicare and Medicaid payments from day one while the review runs.
Intent does not create the exposure here. Billing patterns that look systematic do, regardless of how they got there.
Profiles that attract UPIC attention:
- Inherited billing history: A billing history shaped by a previous coding company whose practices were aggressive. The organization had no visibility into those decisions. But the pattern is in the data and it is what the investigator sees.
- Code concentration: A claim distribution heavily concentrated in one high-value code. The care was legitimate. But that level of concentration looks like a pattern worth investigating.
- Connected entity risk: An association with a referral source or supplier that comes under investigation. The relationship was appropriate. But when connected entities get scrutinized, everyone in the network does too.
A UPIC finding does not resolve as a repayment negotiation. It can result in full exclusion from Medicare and Medicaid. For most practices that is not a financial setback. It is an existential one.
Each of these audits lands differently. But they share one common thread, the financial consequence grows significantly the longer the documentation gap goes undetected.
The scale most teams have not calculated
Most organizations know recoupments are painful when they arrive. What is less visible is how far a single documentation pattern can reach when an auditor starts doing the math.
RAC and MAC TPE contractors do not review every claim. They pull a sample, calculate the error rate, and extrapolate across your entire billing universe for the full lookback period. A 16% error rate on a code range where you billed $2.1 million over three years becomes a $336,000 demand letter. One pattern. Three years. One code range.
By the time that calculation is running the window to do anything about it has already closed.
That is the problem with reactive compliance. It addresses the finding, not the gap that created it. The only way to stop absorbing recoupments is to stop creating the conditions that invite them. That is exactly what blueBriX is built to do.
The blueBriX solution: making audits non-events
The difference between an organization that moves through an audit cleanly and one that does not comes down to one thing. Whether the documentation was built to survive scrutiny at the moment of care, not in response to a demand letter.
When an audit notice arrives at a reactive organization the scramble begins. Staff pulled off normal work. Consultants engaged. Records reconstructed from memory.
When an audit notice arrives at a blueBriX-powered organization the response is different. Every chart in the sample pulls clean because the documentation was built correctly the first time.
How blueBriX closes each gap:
Documentation completeness at the point of care
blueBriX builds the check into the moment of care. When a diagnosis is recorded the rule engine works through a specific set of validations before the chart can move forward:
- Provider authentication: Every note is checked for physician signature, date, and time of encounter. For procedures, the system verifies that a signed physician order is present before the claim moves forward.
- Clinical reasoning: The system checks that the note captures not just what was done but why. A clear clinical narrative connecting the patient’s condition to the decision made during that visit is required.
- Active management: Every diagnosis is validated against MEAT criteria. A diagnosis that does not meet MEAT criteria for that visit cannot move to a claim. This is one of the most consistent findings across RADV and Clinical Validation audits.
- Supporting clinical evidence: Labs, vitals, and any consultant findings referenced in the note must be present in the record. If the auditor cannot see it, it does not exist.
- Diagnosis specificity: Every diagnosis is checked for coding accuracy and specificity. The code must match exactly what the physician documented, no gaps, no mismatches.
- High-value diagnosis criteria: For diagnoses that carry elevated audit risk the engine applies condition-specific checks. Sepsis requires documented evidence of infection source, SIRS criteria, and organ stress. Malnutrition requires a dietitian note. High-complexity MDD requires a narrative that supports that level of complexity.
Billing pattern intelligence
blueBriX continuously benchmarks your billing distribution against national and regional norms by specialty, by code range, and by payer. The moment your patterns start drifting toward outlier territory the system surfaces it in your workflow. Your team sees it, understands it, and can course correct before it crosses the threshold that triggers a MAC TPE probe. You are not discovering the problem from a demand letter three years later. You are managing it in real time, before it becomes one.
Stop revenue risk before it becomes a demand letter
The audit is coming. The question is whether your documentation is ready for it.Stop living under the 3-year shadow. Let blueBriX build your audit defense into your daily clinical workflow before the demand letter arrives.Schedule your Revenue Risk Assessment today.
Book your assessment