Why your patient engagement platform evaluation may already be off track
A patient who leaves a clinic appointment steps into silence. That silence is the gap you are evaluating technology to close. If you are the Econ/Ops owner, the clinical workflow owner, or the IT/Integration Gatekeeper actively comparing patient engagement solutions and working toward a contract, this article is for you. You are at serious risk of signing for the wrong category of tool.
The vendor landscape will not correct this for you. Patient portals and patient engagement platforms are sold under the same language, often by the same vendors, with identical promises around adherence, satisfaction, and outcomes. They are structurally different instruments designed to solve structurally different problems. Portal fatigue (the documented pattern[1] of patients abandoning portals they find friction-heavy or irrelevant to between-visit needs) signals an architectural mismatch, not a UX problem. The portal was never designed for continuous between-visit engagement.
If you buy a portal expecting platform outcomes, you will close this evaluation cycle having spent budget without closing the gap that opened it. Choosing the right solution category matters more than choosing between vendors in the wrong one. Before evaluating any vendor, confirm that the solution category you are comparing can architecturally solve the specific engagement failure you are trying to fix.
Data from ASTP/ONC’s 2024 patient portal access data brief[2] confirms that while 65% of individuals nationally accessed their online medical records or patient portal at least once in 2024, usage gaps remain substantial — with lower rates among older patients, non–English-speaking populations, and patients managing specific high-burden conditions including heart failure and COPD, precisely the populations where proactive, non-portal-dependent outreach is clinically most consequential. The portal access problem is improving. The between-visit engagement problem is not.
This gap is not a new observation. HIMSS research on digital patient engagement[3] has consistently identified the distance between portal access and meaningful between-visit engagement as one of the core unresolved challenges in health system digital strategy, with portal-centric approaches falling short for the populations with the highest chronic disease burden.
Everything that follows is designed to make that distinction concrete, rapid, and defensible when you take it to the committee that has to approve it.
Before the first demo: are you evaluating the right patient engagement solution?
What kind of solution do you actually need? A three-question filter
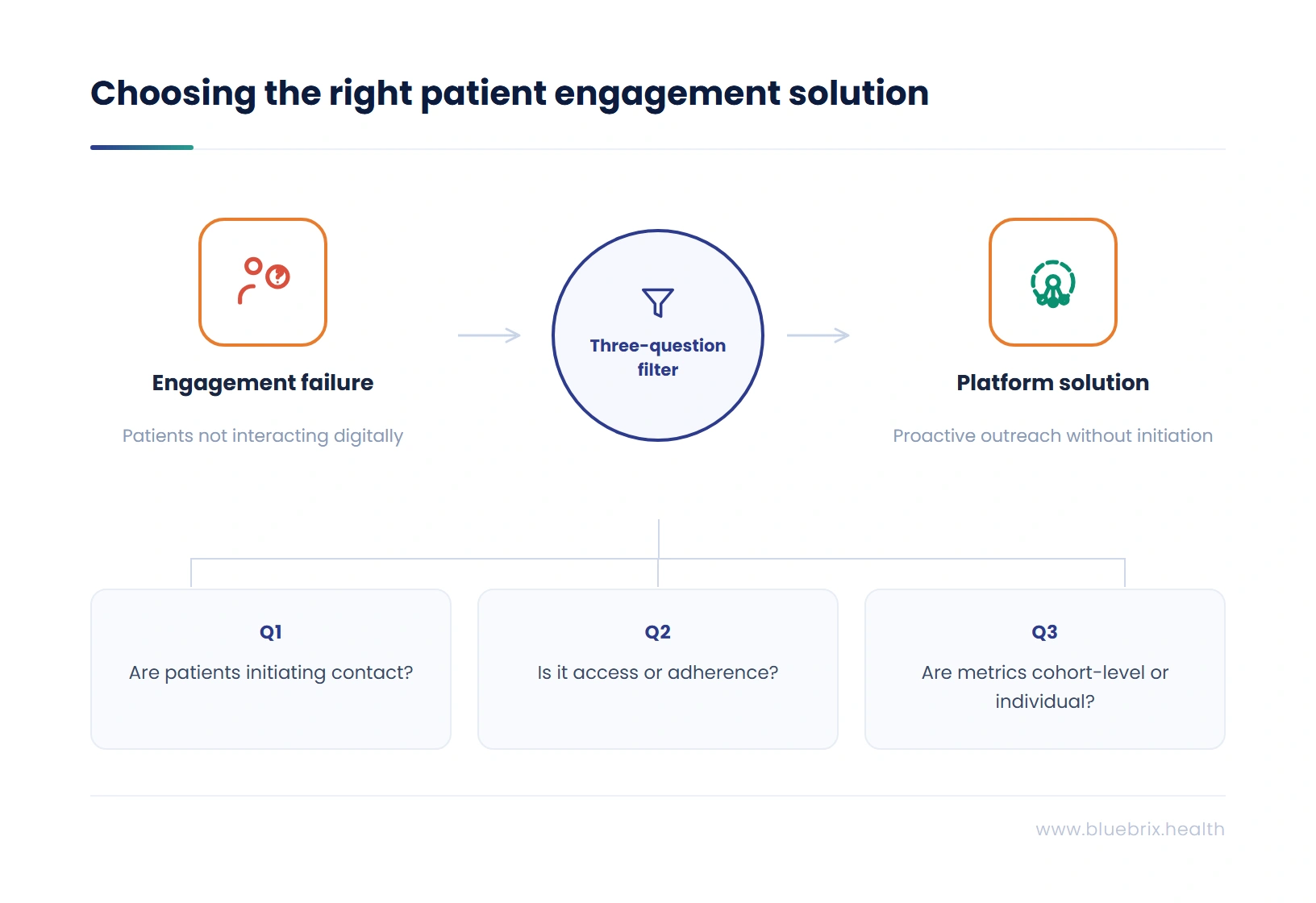
Before any vendor sits across the table, you need a fast, unambiguous test of whether the engagement failure you are trying to solve requires a portal-class solution or a platform-class solution because those two categories will look identical in a demo and perform completely differently in production.
Answer these three questions before you schedule a single demo:
- Are the patients you are failing to engage the ones already logging in, or the ones who have never initiated contact with your digital infrastructure?
- Is your core gap an access problem (patients need easier access to records) or a between-visit adherence problem requiring proactive clinical outreach that operates without patient initiation?
- Does your VBC performance depend on moving cohort-level quality metrics across a defined population, or on improving individual patient satisfaction with the digital access experience?
If your answers point to non-initiating patients, between-visit adherence, and population-level quality metrics, you are looking for a platform, not a portal, and no amount of demo time will change what a portal can architecturally deliver in that context.
When a portal is the right answer
If your answers to the three questions above point toward an access problem, where patients who are already digitally engaged simply need easier access to records, scheduling, or provider messaging, a well-implemented portal may be the appropriate solution for your current engagement need, and a platform investment is not justified by the gap you are trying to close.
Portal-class solutions are the right category when your patient population has high digital literacy and strong smartphone adoption, your primary outcome goal is patient satisfaction with record access rather than population-level care gap closure, and your organization is not yet operating under VBC contracts that require cohort-level quality metric performance.
The diagnostic questions above are designed to surface that distinction before any vendor sits across the table. Most organizations running this evaluation in a VBC environment will find their answers point to a platform. Some will not. If yours do not, the rest of this article will still give you the evaluation framework and RFP language to pressure-test whatever portal-class vendor you are considering.
How to recognize the wrong patient engagement platform before you sign: the failure signatures by persona
The three buyer personas in this evaluation are measuring the engagement problem against completely different failure consequences. A solution that satisfies one buyer’s criteria while failing another’s will not survive the internal approval process regardless of how strong it looks in a vendor scorecard.
| Persona | Portal-class failure signature | platform-class prevention |
|---|---|---|
| Econ/Ops Owner | Quality scores don’t move. Readmission rates don’t fall. Budget committee asks in 18 months why the engagement investment didn’t produce the outcome improvement it was justified against. | VBC contract metrics tracked in real time. Care gap closure velocity visible by cohort. Readmission risk identified before day 30. |
| Clinical Workflow Owner | A parallel workstream maintained alongside the EHR. Care coordinators switching systems daily. Engagement data that never enters the clinical record. | Engagement events surface inside the EHR workflow. AI-generated patient queues eliminate manual list-building. Zero system-switching for care coordinators. |
| IT/Integration Gatekeeper | An 8-week integration scoped in the sales process delivered as 9 months in production. PHI distributed across a new vendor environment not in the security review scope. | Open API, FHIR/HL7 standards, documented compliance posture. Integration maintained under contractual SLA, not the customer’s IT team. |
These are the documented failure patterns of portal-first solutions sold as platforms, and naming them before the evaluation begins is what gives the buying committee the framework to recognize them when they surface in a vendor demo.
How do patient engagement platforms and patient portals actually differ in a live evaluation?
The vendor landscape for patient engagement has converged on a single positioning strategy: every product is called a platform, every portal has added SMS reminders and a mobile app wrapper, and every demo is designed to show the product performing under conditions where the distinction between reactive and proactive engagement is invisible.
Organizations that end up with the wrong solution are not making careless decisions. They are making decisions based on a procurement process the vendor landscape has learned to navigate in its own favor. This section gives you two instruments, demo questions and RFP language, that cut through positioning and require vendors to demonstrate capability rather than describe it.
What questions should you ask in a patient engagement platform demo?
A standard vendor demo shows what the product does when everything works and the patient engages. The questions that reveal the architectural truth are the ones that expose what the system does when the patient does not engage because that is the clinical scenario where the difference between a portal-class and platform-class solution becomes both visible and consequential.
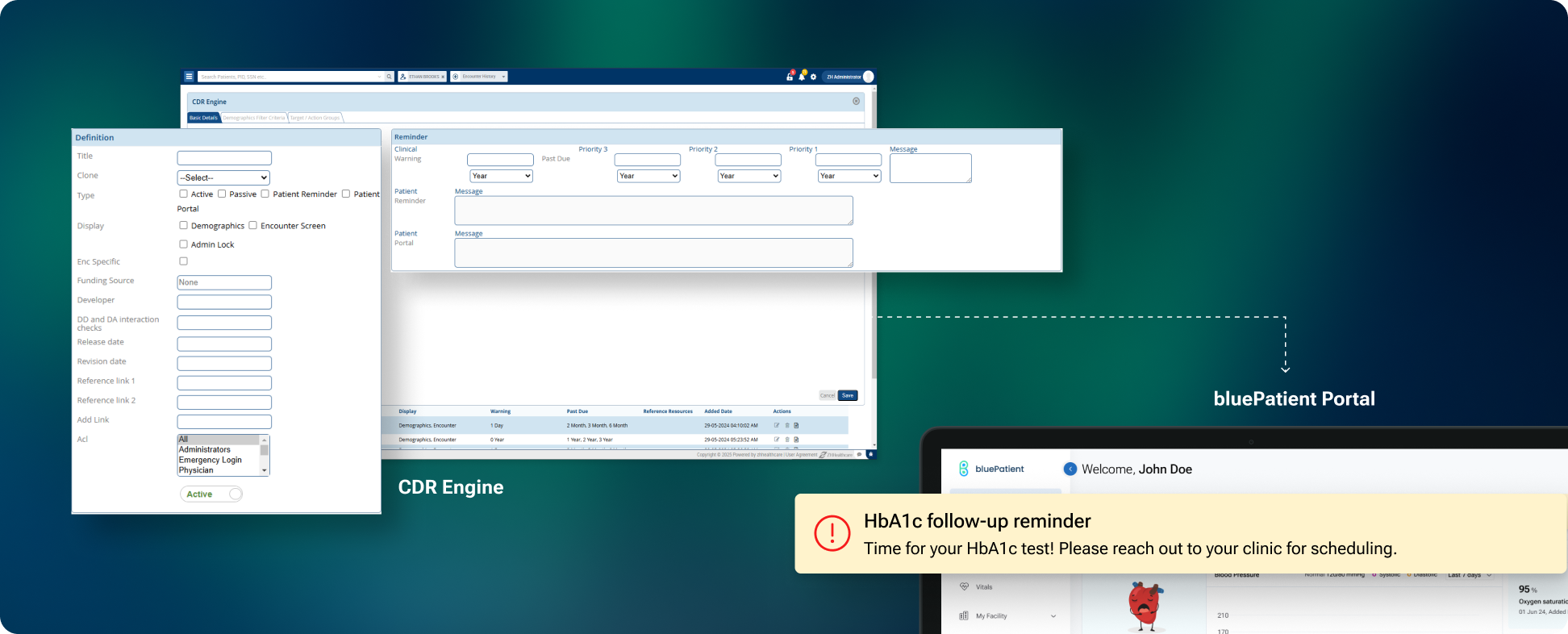
Use these questions in every demo. Require live answers in a working system, not slides, roadmap references, or follow-up calls. The blueBriX column below reflects the capabilities of EngageAI, blueBriX’s proactive patient engagement engine, which operates within the clinical governance framework your team configures.
| Evaluation question | Portal-class solution | blueBriX platform |
|---|---|---|
| Show, live, a patient with an open HbA1c care gap who has not logged in for 60 days. What does the system do automatically, without staff intervention? | ✗ Waits for patient login. No outreach generated without staff action. | ✓ EngageAI identifies the gap from EHR data and initiates outreach automatically via the patient’s preferred channel, within the clinical rules and outreach thresholds configured by your team. |
| Show, live, a patient with an open HbA1c care gap who has not logged in for 60 days. What does the system do automatically, without staff intervention? | ✗ Waits for patient login. No outreach generated without staff action. | ✓ EngageAI identifies the gap from EHR data and initiates outreach automatically via the patient’s preferred channel, within the clinical rules and outreach thresholds configured by your team. |
| When a discharged patient fails to respond to post-discharge follow-up, where does that non-response appear in the clinical workflow, not a vendor dashboard? | ✗ Appears in a separate vendor portal. Care coordinators must check a second system. | ✓ Non-response surfaces as an alert inside the EHR workflow within defined SLA windows |
| Demonstrate a clinical event in the EHR triggering an engagement action, and show the patient’s response in the clinical record, live, not a screen capture | ✗ Cannot demonstrate live bidirectional EHR integration. Integration requires custom build. | ✓ Bidirectional integration is production-ready. Patient response appears in the chart in real time. |
| Does the platform communicate via SMS without requiring the patient to download an application? | ✗ SMS available as add-on but requires app download to access care plan or history. | ✓ Full engagement via SMS, WhatsApp, and voice, with no app required. 40+ languages supported natively. |
| Show a cohort-level outreach campaign: from patient identification through outreach execution through care gap closure, with analytics in a payer-ready format. | ✗ Cohort filtering available but outreach triggered manually per patient. | ✓ Cohort logic driven by clinical data. Campaigns auto-execute. VBC ROI dashboard tracks closure velocity in real time. |
A vendor that cannot answer all five questions live, in a working system, in your EHR environment, has answered the most important evaluation question already.
What RFP language actually forces vendors to prove integration depth?
“Integrates with Epic” and “FHIR-compatible” describe a spectrum of integration depth so wide that two vendors making the identical claim may be separated by a year of IT development work and a fundamentally different production architecture. The HL7 FHIR standard underpinning these claims is required under the CMS Interoperability and Patient Access Final Rule (CMS-9115-F)[4] and reinforced by the Trusted Exchange Framework and Common Agreement (TEFCA)[5], operational since 2022, and the HTI-1 Final Rule (January 2024)[6], which updated health IT certification requirements to USCDI v3. Mandate and implementation depth, however, are not the same thing. The following RFP questions must be answered in writing, with contractual accountability, before any agreement is signed.
| Evaluation question | Portal-class risk | blueBriX platform |
|---|---|---|
| Is the EHR integration bidirectional or read-only? Which specific data objects flow in each direction? | Read-only or partial bidirectionality may be standard. Specific data objects often unlisted until implementation. | ✓ Full bidirectional integration. Data objects and directions documented in the SLA. |
| Is data synchronized in real time or overnight batch? What is the latency SLA? | Overnight batch sync is common. Real-time sync may be priced separately. | ✓ Real-time synchronization. Latency SLA contractually defined. |
| Who owns integration maintenance when the EHR upgrades its API: vendor, customer IT, or third-party partner? | Customer IT team may inherit maintenance. EHR upgrade cycles can require re-engagement of implementation partner. | ✓ Vendor owns integration maintenance. EHR upgrade compatibility maintained under the platform license. |
| Has this integration been implemented in production, not a pilot, with a customer at comparable patient volume and same EHR version? | Production references may be unavailable or at different scale or EHR version. | ✓ Production references available at comparable scale. Same EHR version confirmed before contract execution. |
| What is the data residency model for PHI in transit and at rest? What does the HIPAA audit trail look like? | PHI residency model and audit trail format may vary by configuration and require custom security review. | ✓ HIPAA-compliant architecture with full audit traceability. Compliance posture documented prior to contract. |
These are the procurement requirements whose absence from an RFP is the single most reliable predictor of post-go-live integration disputes in health technology purchasing.
What must a digital patient engagement platform demonstrate before you sign?
Does the platform act when the patient does not? Proactive outreach architecture
The single most important architectural test in any patient engagement platform evaluation is whether the system requires patient initiation to generate a clinically meaningful engagement action. If it does, it is a portal-class solution, regardless of what it is called in the vendor’s marketing materials.
A platform must demonstrate the ability to identify patients who need outreach based on clinical logic, including care gaps, risk scores, missed appointments, post-discharge timelines, and chronic disease management thresholds, and generate that outreach automatically, without staff triggering it manually, across the patient’s preferred communication channel.
The stakes are not abstract. AHRQ’s Healthcare Cost and Utilization Project[7] confirms 3.8 million 30-day all-cause adult hospital readmissions in 2018, at an average cost of $15,200 per event, with hospital readmissions costing Medicare $26 billion annually as of 2018 AHRQ baseline data. The between-visit gap is where that cost compounds invisibly, admission by preventable admission, in the absence of proactive patient engagement infrastructure.
- Proactive outreach architecture verification requires live demonstration of:
- Outreach logic configurable by the clinical team without vendor development tickets
- Care gap identification driven by clinical data from the EHR, not by portal activity
- Escalation logic that automatically changes the communication channel on non-response, within a configurable window
- An audit trail logging every outreach attempt and its outcome in a format legible in a quality review, payer performance report, or CMS audit
Does engagement data live in the EHR or in a vendor dashboard? Bidirectional integration
An engagement platform whose data lives in a proprietary vendor dashboard is not a clinical workflow tool. It is a parallel workstream that adds to care coordinator burden rather than reducing it, and it will produce exactly the adoption failure that the previous engagement technology investment produced, for the same structural reason: clinical staff will not consistently use a system that is not embedded in the workflow they already live in.
The standard for a production-grade engagement platform in a VBC environment: every clinically significant engagement event must appear inside the EHR where clinical decisions are made. This means:
- Engagement events appearing in the patient timeline inside the EHR in real time, not in a nightly batch
- Care coordinator alerts surfacing in the existing clinical workflow without requiring application switching
- Patient-reported data populating structured fields in the chart rather than a PDF attachment requiring manual transcription
The patient’s complete engagement history, including every outreach sent, every response received, and every non-response flagged, visible from inside the patient record.
If you do not require a live demonstration of this specific workflow in your specific EHR before signing, you will discover 90 days into go-live that your care coordinators are maintaining two systems simultaneously. The cause is not inadequate training. It is a platform architecture that was never designed to embed engagement data inside the clinical workflow.
Can the platform reach patients who never use a portal? Omnichannel communication
The patients who most need proactive engagement, including those managing multiple chronic conditions, those with inconsistent internet access, elderly patients without smartphones, and non-English speakers, are precisely the patients least likely to be reached through a portal login. A 2026 study published in AJMC[8] examining adults with chronic conditions confirmed lower portal use among older, non–English-speaking, and Black patients, underscoring the equity gap that portal-dependent engagement creates at population scale.
True omnichannel engagement means the platform reaches patients through the channels they actually respond to: SMS, email, voice, and WhatsApp, with logic that learns which channel a given patient responds to and routes accordingly, without requiring manual staff intervention.
| Evaluation question | Portal-class risk | blueBriX platform |
|---|---|---|
| Does the platform support SMS as a primary engagement channel without requiring the patient to download an application? | SMS may function as a notification layer only. Full engagement may require app download | ✓ SMS is a primary channel, fully functional without app. WhatsApp and voice supported for non-digital patients. |
| Does it support 40+ languages natively, not as a bolt-on or translation service? | Additional languages often via third-party service with added cost and latency | ✓ 40+ languages natively supported. Multilingual engagement is a launch requirement, not a roadmap item. |
| Does channel escalation logic operate automatically on non-response, with configurable escalation windows? | Channel escalation may require manual staff decision. Non-response logged but not automatically acted on. | ✓ Automatic channel escalation on non-response. Escalation windows configurable by clinical team. |
| Does the platform produce a single engagement record per patient across all channels? | Each channel may produce a separate log requiring manual reconciliation. | ✓ Single unified engagement timeline per patient, consolidated across all channels, audit-ready. |
A 2025 study published in Frontiers in Health Services[9] found that digital outreach interventions via text messaging were associated with improved patient engagement in underserved communities where traditional healthcare interactions are limited, reinforcing that channel design determines who gets reached. A platform that only works well for patients with smartphones, broadband, and digital fluency covers a subset of the patient population, not the full population the engagement investment was justified against. blueBriX’s patient engagement solutions are built for channel diversity across SMS, voice, WhatsApp, and 40+ languages, reaching patients regardless of device access or digital literacy.
Can the platform manage a patient population, not just individual transactions? Cohort segmentation
A platform that can only interact with patients one at a time cannot drive the population-level quality metrics that VBC contracts are measured against, cannot produce cohort-level care gap closure at the scale that moves a star rating, and cannot generate the outcome data that justifies the investment to a payer or a budget committee.
A platform genuinely built for VBC environments must demonstrate the ability to segment patient populations by clinical criteria, including chronic condition, risk score, care gap status, payer, and engagement history, and deploy targeted, condition-specific outreach to defined cohorts at scale, without manual case-by-case triggering.
Population health segmentation capability verification requires:
- Cohort logic driven by clinical data from the EHR and configurable by the clinical team without vendor development involvement
- Campaign-level analytics measuring cohort response rates and care gap closure velocity over time
- The ability to connect engagement intervention data to clinical outcome data in a format usable in a payer performance review
- The ability to run simultaneous campaigns across multiple cohorts without manual workload scaling on the care team side
Organizations that do not require a live demonstration of a cohort-level campaign, from patient identification through outreach execution through care gap closure, before signing, will consistently find that what was sold as population health capability is, in production, a manually triggered broadcast messaging tool with a cohort filter applied.
Ready to run these tests on blueBriX?
Bring these four capability tests to a live blueBriX evaluation. The blueBriX team runs structured sessions built around exactly these questions, with your clinical ops lead, IT lead, and Econ/Ops Owner in the same room. Tell us which capability gap is furthest from resolved. We will start there.
Schedule a demoWhat does the wrong patient engagement solution actually cost over 36 months?
The licensing fee is the most visible number in any engagement platform evaluation and the least complete basis for a budget decision. A fair cost comparison between a portal-class and platform-class solution requires the full 36-month picture, not the proposal number.
The right platform costs more upfront and less over time
The full 36-month cost of a platform investment must account for: licensing cost structured by provider, site, or patient volume; implementation cost including internal IT hours and any professional services not bundled in the license; ongoing configuration and administration cost; and the switching cost embedded in the decision: if the platform proves inadequate at 18 months, re-implementation costs in vendor fees, internal IT time, and organizational change management to move clinical staff from one system to another for the second time in two years.
The case for a platform over a portal is not that the platform is cheaper upfront. It is that the platform produces measurable outcome improvements in readmission reduction, care gap closure, VBC quality performance, and care coordinator capacity that a portal cannot produce at the same scale. Over 36 months, that performance difference is the financial argument.
The measurable cost of buying a portal when the problem required a platform
The financial consequence of a wrong-category purchase is measurable across the specific outcome dimensions the purchase was justified against. AHRQ’s 2018 HCUP readmissions data documents an average readmission cost of $15,200 per event, and readmissions not prevented because post-discharge outreach went to a portal the patient never opened are a directly calculable exposure against the organization’s actual readmission volume. VBC quality bonuses not earned because care gaps were not closed at population scale represent a second exposure line. A randomized clinical trial published in JAMA Network Open[10] found that automated post-discharge outreach programs were associated with reduced acute care resource use and limited manual staff involvement to patients with identified clinical needs. That staff time is labor cost that remains in the budget when the engagement tool is a portal.
Each of these is a line item, not an abstraction. The Econ/Ops Owner who builds this model into the committee presentation, rather than just reading it in preparation, is the one who can defend the platform investment against a portal proposal backed only by a lower license fee.
Why does blueBriX win the patient engagement platform trade-offs your shortlist is forcing?
For the econ/ops owner: where does blueBriX outperform on the financial model?
At decision stage, the Econ/Ops Owner is not asking what blueBriX does. They have seen the demo. They are asking why blueBriX produces better financial outcomes than the alternatives on the shortlist, and whether the performance claims survive a budget committee’s scrutiny.
The shortlist is typically forcing one of two trade-offs. The first is between a portal-forward vendor that has added platform marketing language and a purpose-built engagement platform. The portal-forward vendor will show comparable features in a demo and deliver significantly lower proactive outreach performance in production, because its underlying architecture is still patient-initiated. That architectural difference surfaces in care gap closure rates and readmission metrics within the first two quarters of deployment, exactly the metrics the Econ/Ops Owner is accountable for in a VBC contract.
The second trade-off is between an EHR-native engagement module and a dedicated platform. The EHR-native module offers integration familiarity but delivers population health capability constrained by the EHR vendor’s development roadmap, producing a cohort management tool that cannot be configured to the organization’s specific contract performance requirements without a vendor development cycle.
blueBriX addresses both trade-offs through the following production capabilities:
- A configurable clinical rules engine and low-code/no-code platform that allows the organization’s own team to configure outreach logic, cohort criteria, and engagement campaigns against VBC contract requirements without opening a vendor ticket
- Real-time analytics dashboards that track engagement scores, care deviations, CAHPS metrics, and readmission rates in one view, connecting engagement activity directly to the quality performance data the Econ/Ops Owner is accountable for.
- A direct connection between engagement intervention and VBC financial outcomes: care gap closure rates, shared savings calculations, and quality bonus trajectory visible in a single dashboard
When Arkos Health, a leader in value-based care bridging gaps between providers, patients, and payors, needed to scale population health management and care coordination, blueBriX delivered the clinical workflow configuration and real-time care coordination infrastructure that underpins their Arkos 360 platform. Read the Arkos Health case study.
For the clinical workflow owner: where does blueBriX reduce care coordinator workload that others do not?
The clinical workflow owner’s shortlist trade-off is not between features. It is between a platform that reduces clinical staff workload by embedding engagement in the workflow they already live in, and a platform that adds engagement capability in a system parallel to that workflow, creating a monitoring and reconciliation burden that negates the productivity benefit the platform was purchased to deliver.
Portal-forward vendors surface engagement data in a vendor dashboard that care coordinators must check independently of the EHR, adding a daily task to the workflow rather than removing one. EHR-native engagement modules are embedded in the EHR but constrained to the EHR’s outreach logic, meaning the care coordinator is still making manual outreach decisions for patients the system cannot automatically identify as requiring intervention.
blueBriX’s risk stratification capability segments patients by chronic condition, social risk, utilization, and VBC program, and auto-updates patient queues in real time as new clinical data flows in, surfacing the patients who need care coordinator attention without requiring manual list-building or report-running.
A randomized clinical trial published in JAMA Network Open found that automated post-discharge outreach programs were associated with scaled-up patient contact while conserving staff time for patients with identified clinical needs. Automated patient outreach built into the clinical workflow means care coordinators focus exclusively on escalations rather than routine contact attempts, reclaiming the capacity that makes the difference between a team that is reactive and one that is proactive.
Additional workflow differentiation that shows up in care coordinator workload after go-live, not in a feature comparison during the evaluation:
- Predictive insights that flag avoidable event patterns and surface care gap timers before STAR windows close
- High-risk alerts connected directly to outreach actions and configurable care plans: no manual handoff between identification and intervention.
- Protocol changes and VBC contract updates configurable in an admin console session by the organization’s own staff, without a vendor development ticket, through the no-code clinical rules engine
Vivos Therapeutics built the MyoSync patient engagement platform on blueBriX to extend digital care delivery across their patient population. Read the Vivos MyoSync case study.
For the IT/integration gatekeeper: where does blueBriX simplify the integration stack that others expand?
Every vendor on the IT/Integration Gatekeeper’s shortlist claims EHR integration and FHIR compatibility. The differentiation that matters to this buyer is not in those claims. It is in the specific production architecture decisions that determine whether the platform simplifies the organization’s data environment or adds another node to an already fragmented integration stack.
blueBriX’s open API, standards-based integration architecture supports FHIR, HL7, and custom endpoints, designed for plug-and-play interoperability with EHRs, HIEs, labs, payers, and enterprise systems including Salesforce, SAP, and business intelligence platforms. Its restful API design with extensive documentation reduces the custom integration build work that portal-forward vendors typically require of the customer’s IT team.
The integration trade-off this section resolves: the difference between a vendor whose integration is a product, maintained, documented, and under contractual SLA, and a vendor whose integration is a project that the customer’s IT team inherits, maintains, and re-executes with every EHR upgrade cycle.
| Evaluation question | Portal-Class risk | blueBriX platform |
|---|---|---|
| Integration architecture: open, documented, standards-based vs. proprietary build required? | Proprietary integration layer may require custom build per EHR instance. | ✓ Open API with FHIR, HL7, CDA support. Standards-based from the foundation. |
| Integration maintenance ownership: vendor SLA or customer IT team? | Customer IT may inherit integration maintenance after go-live. | ✓ Vendor owns integration maintenance under the platform license SLA. |
| Integration maintenance ownership: vendor SLA or customer IT team? | Customer IT may inherit integration maintenance after go-live. | ✓ Vendor owns integration maintenance under the platform license SLA. |
| HIPAA audit traceability: documented posture or built per customer? | Compliance posture may require custom security questionnaire per customer. | ✓ HIPAA-compliant architecture with full audit traceability. Documented prior to contract execution. |
| PHI data residency: defined, contractual model or unclear until production? | PHI residency model may be clarified during implementation, not pre-contract. | ✓ PHI residency model defined contractually before signature. |
The specific reference customer conversation parameters the IT/Integration Gatekeeper should require before accepting any vendor’s integration claims: same EHR, comparable patient volume, similar IT architecture. Not a pilot. Not a sandbox. A production reference, contactable directly before the contract is signed.