If you have been running Spravato sessions for any length of time, you already know that this is not a therapy you can bill on autopilot. The clinical complexity is real, the documentation requirements are strict, and the payer landscape is fragmented enough to trip up even experienced billing teams.
But here is what most guides on spravato billing miss: the organizations that consistently get paid right the first time are not just following a better checklist. They have built a fundamentally different kind of revenue cycle, one that is designed from the ground up for hybrid therapies, payer variability, and the long-tail demands of a multi-phase treatment program.
This article is written for the teams that are past the basics and ready to close the gaps that are still costing them revenue. If you are looking for a foundational overview of spravato billing codes, documentation requirements, and REMS compliance, we covered that in depth in our spravato billing and coding best practices guide. What follows here is the next layer: the advanced RCM framework that turns Spravato from a billing liability into a predictable, scalable revenue stream.
The Spravato revenue gap: why "getting the basics right" is not enough anymore
Let us start with a number that tends to get people’s attention. A single Spravato session, when fully and correctly reimbursed, brings in somewhere between $1,300 and $1,600. The drug component alone accounts for roughly $875 of that. When a claim is denied and not recovered, that is not just one lost payment. It is the cost of the drug, the clinical staff time, the administrative rework, and often the patient relationship strain that comes with billing delays. Now multiply that across a patient panel running two sessions per week during induction. The financial exposure compounds quickly, and most clinics have never formally calculated what their actual Spravato denial rate is costing them on an annualized basis.
The other dimension of the revenue gap that rarely gets discussed is silent leakage: claims that are paid, but underpaid. This happens when prolonged service codes are not captured, when observation time is not documented precisely enough to justify higher-level E/M codes, or when drug units are billed at a flat rate rather than reflecting the exact milligrams administered. None of these show up as denials. They simply reduce your reimbursement without triggering any alert.
The implication is clear: treating spravato billing as a compliance exercise rather than a revenue integrity discipline is costing most organizations more than they realize. The gap between what is being billed and what should be billed is often as large as the gap between what is billed and what is paid. With the financial stakes clearly established, the logical next question is: where exactly is the money going? For most clinics, the answer starts with the payers themselves and with how poorly understood their individual Spravato policies actually are.
How major payers actually handle Spravato and where they silently differ?
One of the most persistent myths in spravato billing is that payer rules are broadly consistent and that knowing the codes means knowing what to expect. In practice, the differences between how major payers handle Spravato are significant, specific, and rarely documented in one place.
Medicare
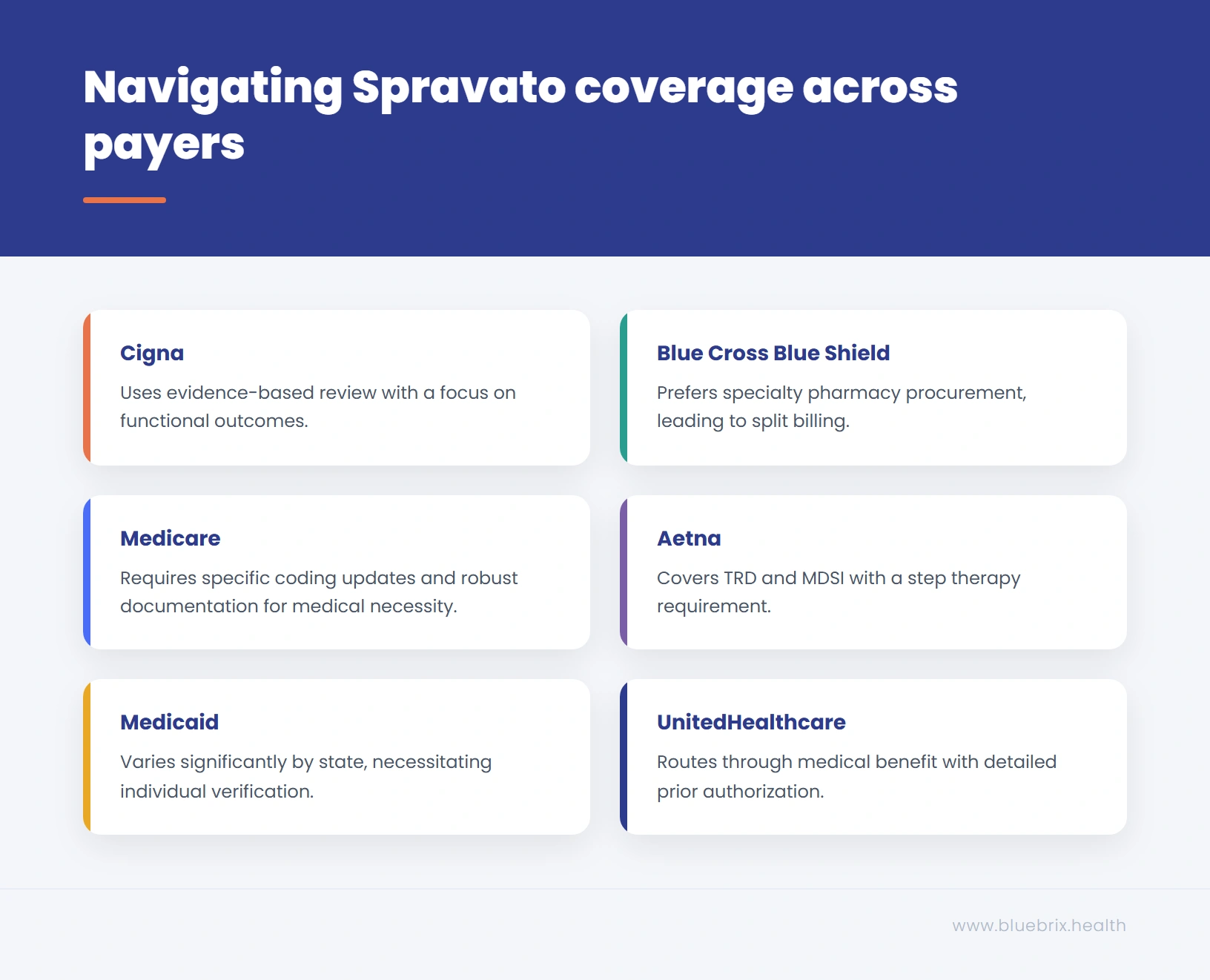
Effective January 1, 2026, CMS deleted HCPCS code S0013 and replaced it with J3013 (esketamine, nasal spray, 1 mg). G2082 and G2083 remain active for Medicare buy-and-bill. Some payers are mid-transition and may still accept J3490 as an unclassified fallback, but claims submitted with S0013 will be denied. Billing teams should update their charge masters immediately to reflect J3013. Under the buy-and-bill model, the drug is reimbursed at average sales price (ASP) plus a 6% add-on. The challenge with Medicare is not just the coding; it is the documentation threshold for medical necessity, which requires robust evidence of at least two prior antidepressant failures with documented duration and clinical response, plus a formal assessment using a validated scale such as PHQ-9 or MADRS.
Medicare also scrutinizes observation time coding heavily, and claims that include G2212 (prolonged office visits) without precise start and stop times in the clinical notes are among the most commonly flagged. CPT codes 99354 and 99355 were deleted effective January 1, 2023. The correct codes are 99417 (for commercial payers, billed per each additional 15 minutes beyond the primary service time for 99215) and G2212 (for Medicare). Submitting claims with the deleted codes will result in automatic rejections.
Medicaid
Medicaid coverage for Spravato varies significantly by state, which makes it the most unpredictable payer category for multi-state behavioral health organizations. Some state Medicaid programs have approved Spravato coverage with specific prior authorization criteria; others have issued non-coverage determinations or restricted it to specific diagnoses. The critical point here is that you should not assume Medicaid coverage based on state proximity or historical patterns. Each state program must be verified individually, and authorization criteria can change with minimal notice.
UnitedHealthcare
UnitedHealthcare routes Spravato through the medical benefit for most commercial plans and requires prior authorization through their specialty program. Their PA criteria are notably detailed, including specific requirements for the prescribing provider’s credentials, documentation of the REMS enrollment, and in some cases an attestation that the patient has been informed of the therapy’s risk profile. UnitedHealthcare is also one of the more aggressive payers when it comes to maintenance phase re-authorization, often requiring updated clinical documentation demonstrating continued response at the six-month mark.
Aetna
Aetna’s coverage policy for Spravato has been updated several times and currently covers it for both TRD and major depressive disorder with acute suicidal ideation (MDSI) under medical necessity criteria. One area where Aetna commonly generates denials is the step therapy requirement: their policy may require documentation that the patient has trialed specific antidepressant combinations, not just any two medications. Billing teams that submit generic “two failed antidepressants” documentation without specifying the drugs, doses, and duration often face clinical review requests that delay reimbursement by weeks.
Blue Cross Blue Shield
BCBS plans vary considerably by region given the federated nature of the network, but the common thread across most BCBS affiliates is a strong preference for specialty pharmacy procurement over buy-and-bill. This means the drug component is often handled through pharmacy benefits while the administration and observation services are billed under medical benefits, creating the split-billing workflow that generates the highest rate of claim coordination errors. BCBS plans are also among the more likely to require peer-to-peer review when initial PA is denied, and having a structured peer-to-peer protocol ready is a meaningful operational advantage.
Cigna
Cigna covers Spravato under the medical benefit for most plans and uses an evidence-based medical necessity review process. One distinctive element of Cigna’s approach is their requirement for ongoing functional outcome documentation: they want to see not just that the patient received treatment, but that the treatment is producing measurable clinical improvement. Billing teams that rely solely on session notes without standardized outcome measures are more likely to face re-authorization challenges at the maintenance phase.
Understanding how payers behave tells you what they need. But whether your claims consistently give them what they need depends on a different part of the workflow entirely: your REMS documentation pipeline, and how cleanly it connects to your billing process.
The REMS-to-billing pipeline, where compliance gaps become claim denials
REMS is discussed in most spravato billing content as a background requirement: enroll, comply, move on. What that framing misses is that the REMS program is not just a regulatory safeguard. It is the primary data source for a significant portion of what your billing claims need to prove. When a payer reviews a Spravato claim, they are not just checking that the right codes are present. They are asking: was this therapy administered in a compliant, supervised setting, by a qualified provider, to a patient who met the clinical criteria? The answers to those questions live in your REMS records, and if those records do not translate cleanly into your billing documentation, the claim fails regardless of how accurate the coding is.
What REMS data maps to claim requirements
Every REMS session log contains several data points that have direct billing implications. The patient’s REMS enrollment status confirms treatment eligibility and must be active at the time of each session. The provider certification confirms the prescribing clinician’s authority to administer Spravato, which some payers verify independently. The facility certification confirms the REMS-certified status of the clinic, which is required for medical necessity documentation. The session-level documentation, including the two-hour observation log, is what validates the prolonged service codes that drive a significant portion of the session’s reimbursement value. When any of these data points are missing, inconsistent, or not properly transcribed into the billing record, the claim is vulnerable, even if the CPT and HCPCS codes are perfect.
The lapsed enrollment problem
One of the most consistently underestimated REMS-related billing risks is patient enrollment lapse. REMS enrollment for both patients and providers has expiration requirements, and in a busy clinic environment, renewals can slip. When a session is administered during a lapsed enrollment window, it does not just create a compliance issue. It creates a billing problem: any claim submitted for that session is technically not supported by an active REMS authorization, which gives payers grounds for denial or clawback. The solution is not just better tracking. It is building REMS renewal verification into the pre-session billing checklist as a hard stop, the same way eligibility verification works. If the REMS enrollment cannot be confirmed active before the session begins, the billing team should flag it before the clinical team proceeds.
Tracing denials back to their actual origin
This is where the REMS-to-billing connection has its most practical implication. When Spravato claims are denied for reasons coded as “insufficient documentation” or “medical necessity not established,” billing teams naturally look at their clinical notes and coding first. But a significant proportion of those denials actually originate in one of three upstream REMS failures: expired provider certification, incomplete session-level observation logging, or a documentation gap between what is recorded in the REMS portal and what is transcribed into the EHR. Closing that gap requires a workflow where REMS records and clinical documentation are reconciled before claim submission, not after a denial arrives. Organizations that build that reconciliation step into their pre-billing process typically see their “documentation-related” denial rate drop materially within a single billing cycle.
Treat REMS data as a billing source document. Every session that generates a claim should have a corresponding REMS log review as part of the charge capture process. With the REMS pipeline addressed, the next major pressure point in the Spravato revenue cycle is the prior authorization process itself, which is far more complex and active than most billing teams have workflows to handle.
The prior authorization lifecycle: what actually happens after you hit submit
Most billing guides treat prior authorization as a task: submit the request, wait for approval, proceed with treatment. The reality of Spravato PA is considerably more dynamic, and organizations that understand the full lifecycle of a PA request are far better positioned to protect their reimbursement at every stage.
Auto-approval versus clinical review: what determines the path
Not all PA requests go to the same place. When a PA submission meets every element of the payer’s clinical criteria, is accompanied by complete documentation, and is submitted by a credentialed provider with a clean prior authorization history, it is more likely to route toward administrative or auto-approval. When any element is missing or ambiguous, including documentation format, diagnosis specificity, or treatment history detail, it triggers a clinical review queue, where it may sit for days or weeks before a decision is made.
Understanding what triggers clinical review for each payer and structuring your PA submissions to proactively address those triggers is one of the highest-value skills a spravato billing team can develop. It is the difference between a five-day turnaround and a three-week delay.
The peer-to-peer review: how to prepare and what to expect
When an initial PA is denied, most payers offer a peer-to-peer (P2P) review pathway, where the treating clinician speaks directly with the payer’s medical reviewer. For Spravato, P2P reviews are not uncommon, particularly when the patient’s treatment history is complex or when the payer’s criteria are stricter than the FDA’s approved indications. The clinics that consistently succeed in P2P reviews share two things.
- They prepare a structured clinical summary before the call that covers diagnosis, failed treatment trials with specific details, and the clinical rationale for Spravato; and they treat the call as a clinical conversation, not a confrontation.
- Payer medical reviewers are typically psychiatrists or clinical pharmacists. They respond to clinical evidence and professional peer dialogue, and a well-prepared P2P call often converts a denial into an approval within 24 to 48 hours.
Step therapy requirements and how to navigate them
Several major payers, most notably Aetna and some BCBS affiliates, apply step therapy requirements to Spravato that go beyond the FDA’s general criterion of two failed antidepressants. These requirements may specify particular drug classes, combination therapies, or augmentation strategies that must be documented as having been attempted. When these requirements are not clearly addressed in the PA submission, the result is either an automatic denial or a clinical review request for additional information.
The most effective way to manage step therapy requirements is to maintain a current, payer-specific step therapy matrix for Spravato that is accessible to both the clinical team during treatment planning and the billing team during PA preparation. When the treatment history is documented with step therapy criteria in mind from the beginning, PA submissions are materially stronger and require fewer supplemental requests.
The induction-to-maintenance authorization gap
One of the most reliably problematic transitions in the Spravato PA lifecycle is the move from induction to maintenance. PA approvals for Spravato induction are typically issued for a defined period, often 30 to 90 days, with specific session frequency parameters. When the patient transitions to maintenance dosing, which has a different frequency and in many cases different clinical justification requirements, a new authorization is needed. And in many clinics, that re-authorization is not initiated early enough.
The result is a gap: sessions are administered during the maintenance phase while the new PA is pending, and claims for those sessions are held or denied. The financial impact can be significant, and it is entirely preventable with a PA expiration tracking workflow that triggers re-authorization requests 30 days before the current approval expires.
Managing the PA lifecycle well during induction is achievable with discipline and good tracking. But the maintenance phase is where that discipline is most often allowed to slip, and where the revenue consequences are felt most acutely over time.
Maintenance phase billing: the long-tail revenue problem most clinics underestimate
The induction phase of Spravato therapy gets the most attention in billing guides, training programs, and payer policy documents. It makes sense: induction involves the highest session frequency, the steepest learning curve, and the most immediate revenue at stake. But the maintenance phase is where Spravato’s long-term financial value either compounds or quietly erodes.
How billing requirements shift in the maintenance phase?
During induction, session frequency is clearly defined by the FDA-approved schedule (twice weekly for four weeks), which makes billing relatively predictable once the PA is in place. During maintenance, the frequency drops to once weekly, then once every one to two weeks, and the clinical justification for continued therapy must evolve to reflect the patient’s current status rather than their initial eligibility criteria.
This shift has direct billing implications. The medical necessity documentation that supported induction, centered on the patient’s diagnosis and failed treatment history, is no longer sufficient on its own. Maintenance-phase claims need to demonstrate ongoing clinical response, continued need for supervised administration, and the absence of adverse events that would contraindicate continued therapy. Clinics that carry their induction-phase documentation templates into the maintenance phase without updating them are building claims on a foundation that payers will increasingly challenge over time.
Re-authorization cycles and the documentation trap
Maintenance phase re-authorization introduces a documentation trap that catches many clinics off guard. The initial authorization was built around the patient’s baseline clinical picture. The re-authorization needs to tell a different story: one of measurable improvement, or in some cases, stabilization that justifies continued treatment even without dramatic symptom reduction.
This requires standardized outcome measurement as a routine part of every maintenance session, not just the periodic clinical review. Payers like Cigna and UnitedHealthcare are increasingly specific about wanting outcome data in re-authorization requests, and organizations that have been collecting PHQ-9 or MADRS scores at every session are in a dramatically stronger position than those that have not.
The coding drift problem
Another maintenance-phase revenue risk that rarely gets named explicitly is coding drift: the gradual misalignment that develops between the codes being submitted and the clinical reality of the session. In maintenance, sessions are shorter, the observation period is the same but the E/M complexity may be different, and the prescribing dynamics may have shifted as the patient’s condition stabilizes. Billing teams that apply induction-phase coding patterns to maintenance sessions without periodic review are likely either undercoding (missing reimbursable service elements) or overcoding (claiming complexity that is no longer supported by the notes), both of which create financial and compliance risk.
A quarterly coding audit of a representative sample of maintenance sessions is one of the most cost-effective revenue integrity practices a Spravato program can implement. It takes minimal time and routinely uncovers patterns worth correcting.
Maintenance phase complexity is real and manageable with the right workflows. But it does not affect all care settings equally. The billing rules, modifier requirements, and payer relationships for Spravato vary meaningfully depending on where the therapy is administered, and those differences create both risks and opportunities that many organizations have not yet mapped.
How spravato billing differs across group practices, FQHCs, and hospital-based clinics?
Most spravato billing content is written with a single-site independent practice in mind. But the behavioral health organizations evaluating or operating Spravato programs are increasingly diverse in their structure, and the billing rules change meaningfully depending on the care setting.
Independent and group practices
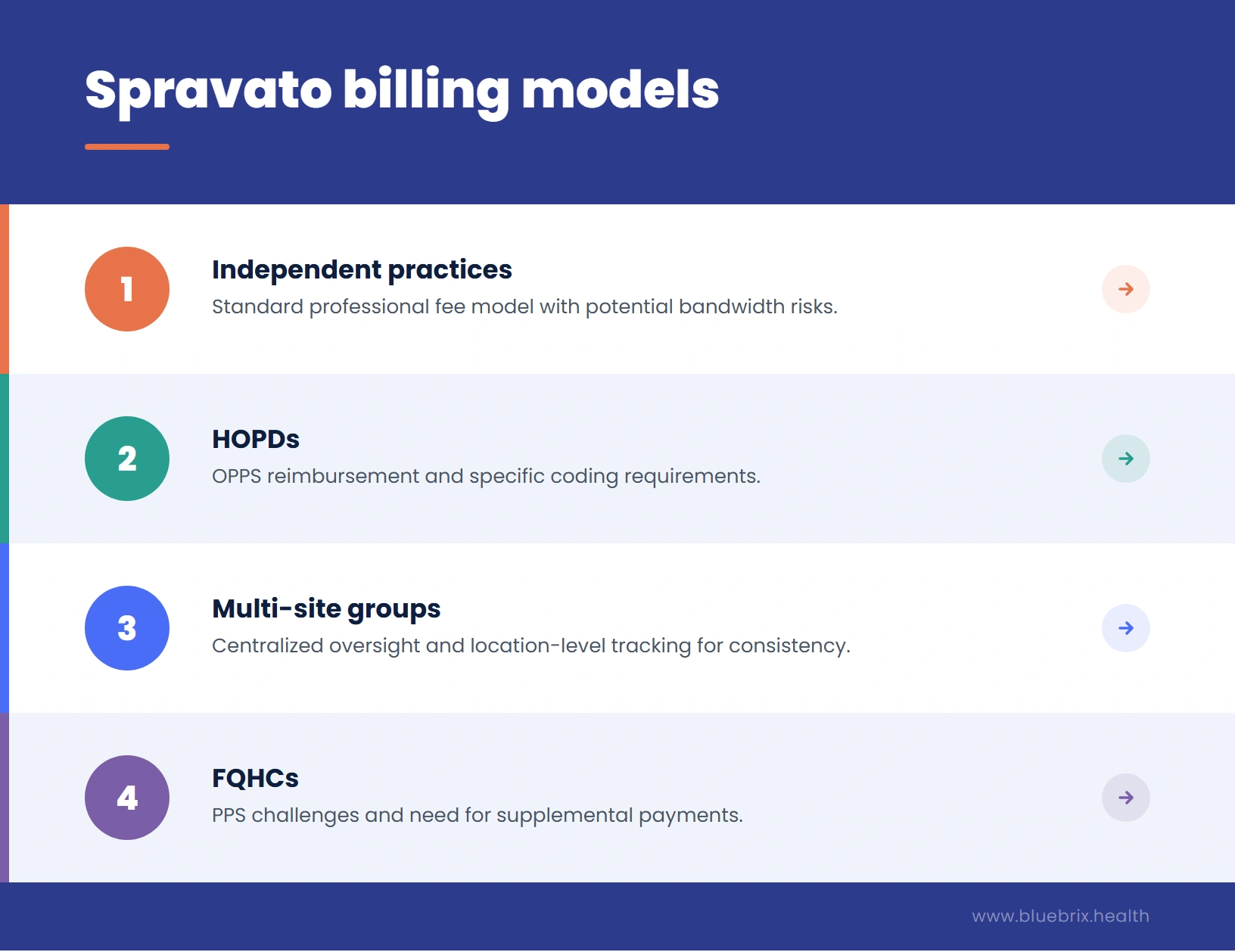
For independent and small group practices, spravato billing follows the standard professional fee model. The clinic bills using the physician’s NPI, codes are submitted on a CMS-1500 form, and the buy-and-bill or assignment of benefits model is chosen based on the practice’s preferred procurement approach and payer requirements. The primary risk in this setting is the absence of dedicated billing infrastructure: in smaller practices, the same staff member who schedules patients is often also managing PA requests and claim submissions, which creates bandwidth and accuracy risks.
Multi-site group practices
Multi-site organizations face a compounding version of the single-site challenges, with the added complexity of maintaining coding consistency and payer rule compliance across locations that may be in different states, served by different payer mixes, and staffed by providers with different credentialing profiles. For multi-site groups, the highest-value investment is typically in centralized billing oversight with standardized Spravato-specific protocols that apply across all locations, combined with location-level performance tracking that can identify outlier sites before their denial rates become systemic.
Federally qualified health centers (FQHCs)
FQHCs operate under a prospective payment system (PPS) for Medicaid, which means they receive an all-inclusive per-visit rate rather than fee-for-service reimbursement for Medicaid patients. This creates a significant complication for spravato billing: the drug cost, which is the largest component of a Spravato session’s reimbursement value, may not be adequately covered under the PPS rate. FQHCs need to verify whether their state Medicaid program has established a separate drug supplemental payment mechanism for Spravato, or whether the therapy can be billed under the medical benefit outside the PPS rate for certain payers. This is an area where getting specialist guidance before launching a Spravato program is essential, because the reimbursement model assumptions that work in a fee-for-service setting may not translate to the FQHC context.
Hospital outpatient departments (HOPDs)
For hospital-based outpatient clinics, Spravato services are reimbursed under the Medicare Outpatient Prospective Payment System (OPPS), which assigns a specific Ambulatory Payment Classification (APC) to the service. The reimbursement rates under OPPS are different from the professional fee schedule, and the coding and billing process uses a UB-04 claim form rather than a CMS-1500. Hospital billing teams that are accustomed to standard outpatient encounter billing may not have experience with the specific HCPCS drug codes or the observation service requirements that Spravato introduces, and the revenue integrity risks in this setting are often related to incomplete charge capture rather than coding errors by itself.
Regardless of care setting, the quality of the billing outcome ultimately depends on whether the technology and workflow infrastructure in place can actually support Spravato’s hybrid demands. For many organizations, that is where the next honest assessment needs to happen.
Is your tech stack Spravato-ready?
One of the most uncomfortable truths in Spravato RCM is that many clinics are running a complex, hybrid-benefit therapy through billing infrastructure that was never designed for it. The result is not always obvious. Claims still go out. Some get paid. But the error rate is structural, baked into the system rather than the result of individual mistakes, and it will not improve with training alone.
A self-audit for billing and RCM leaders
Use the checklist below to assess your current tech stack, workflow design, and billing processes. It will help you identify the gaps most likely contributing to Spravato revenue leakage, from missed documentation and authorization issues to disconnected scheduling, inventory, and claims workflows.
Download hereBuilding your internal spravato billing playbook: roles, checkpoints, and escalation paths
A mature spravato billing operation is not just a collection of good practices. It is a structured workflow where every role is clearly defined, every handoff is explicit, and every failure mode has a documented response. Most clinics have the individual pieces; what they lack is the architecture that connects them.
Role definition: who owns what
The first step in building a reliable spravato billing playbook is being explicit about role ownership across the clinical and administrative teams. In many clinics, ownership is implied rather than assigned, which means that when something falls through the cracks, no one is clearly accountable for catching it.
A functional spravato billing workflow typically requires clear ownership across five roles: the prescribing clinician, who owns medical necessity documentation and clinical notes; the clinical support staff, who own real-time observation logging and REMS session documentation; the billing coordinator, who owns charge capture, code selection, and pre-submission review; the authorization specialist, who owns the PA lifecycle from initial submission through re-authorization; and the RCM analyst or manager, who owns denial tracking, performance reporting, and escalation management.
Pre-session, mid-session, and post-session checkpoints
The most effective spravato billing playbooks build checkpoints into the workflow at three distinct moments rather than relying on a single pre-submission review.
- Before the session begins, the workflow should verify active REMS enrollment, confirm PA status and remaining authorized sessions, run real-time eligibility verification, and confirm that the clinical notes template for the session is set up to capture all billable elements including observation time and outcome scores.
- During the session, clinical staff should be logging in real time: administration time, dosage administered, observation start time, vitals at regular intervals, and any adverse events with their management. This is not just a compliance requirement; it is the evidentiary foundation for every time-based code in the claim.
- After the session, the billing coordinator should reconcile the clinical notes with the REMS session log, confirm that all codes are aligned with the documentation, verify that the drug units match the administered dosage, and flag any elements that need clinician clarification before the claim is submitted.
Escalation paths: what happens when something goes wrong
A well-designed escalation path is what separates billing teams that recover from denials quickly from those that let them age into write-offs. For Spravato specifically, the escalation framework should address three common failure modes: clinical documentation gaps that require provider input before a claim can be submitted or appealed; PA denials that require a peer-to-peer review; and technical billing errors that require payer contact and claim correction. Each of these should have a documented owner, a defined response timeline, and a clear threshold for escalating further up the management chain. The goal is to ensure that every failure is handled systematically rather than ad hoc.
Performance tracking: what to measure
The metrics that matter most for a spravato billing operation are not the same as those for general medical billing. First-pass claim rate by session phase (induction vs. maintenance) matters more than aggregate first-pass rate, because the failure modes are different. Days in AR for Spravato claims tracked separately from the general AR aging gives you a more accurate picture of where the bottlenecks are. PA approval rate and average PA turnaround time are leading indicators of claim performance, not lagging ones. And reimbursement per session, tracked against expected reimbursement, surfaces underpayment patterns that denial rates miss entirely.
With the full operational picture now in view, including financial stakes, payer intelligence, REMS pipeline, PA lifecycle, maintenance phase, care setting nuances, tech requirements, and internal workflow, the question that every reader arrives at is the same one: should we build this capability internally, or partner with someone who already has it running?
Future-ready spravato RCM starts here
The organizations that are winning in Spravato revenue integrity right now are the ones that recognized early that this therapy required a different kind of RCM approach, and made the decision to build on an existing foundation rather than start from scratch. Your Spravato program deserves a revenue cycle that keeps up with it. Book a free demo and see how blueBriX handles Spravato RCM end to end.
Schedule a demo