You have built something worth growing. Your caseload is up, your referral pipeline is healthy, maybe you have added a provider or two in the past year. And somewhere in the middle of all that momentum, billing quietly became the thing that is slowing everything else down.
More sessions mean more claims. More providers mean more credentialing. More payers mean more prior authorizations, more rules, more denial letters to chase. And at some point, the question stops being ‘are we growing?’ and starts being ‘can our billing operation actually keep up?’
The reflexive answer most practices land on is to hire. Another biller, a dedicated coder, someone to own the denial queue. But that answer gets expensive fast, and it rarely fixes the underlying problem. The practices that scale efficiently are not the ones with the biggest billing departments, they are the ones that figured out how to stop letting billing work grow in proportion to patient volume.
The billing bottleneck that grows with you
Behavioral health billing has a particular kind of complexity that does not get easier as you scale. And a lot of practice leaders only realize how deep the problem runs once the cracks start showing up in cash flow.
Unlike most medical specialties, almost everything in behavioral health billing is time-based. A 45-minute session maps to a different CPT code than a 60-minute one. Group therapy is coded differently from individual. Telehealth carries its own modifiers. Add in the fact that every payer interprets these codes slightly differently, prior authorization windows expire and need renewals, and documentation standards vary depending on whether you are billing Medicaid, a commercial plan, or Medicare, and you start to see how a single billing error is rarely just one error. It is a pattern waiting to repeat.
What this looks like in practice:
A group practice in the Midwest added three new therapists over 18 months. Patient volume grew by 40%. But their billing team was the same size it had been at six providers. Nobody noticed that one of the new therapists had been consistently using the wrong time-based code for 53-minute sessions, billing 90834 instead of 90837 for four months. By the time it surfaced in an A/R review, the practice had left roughly $18,000 in reimbursement on the table, and resubmission windows with two payers had already closed.[1]
Where the revenue actually disappears
The financial cost of a poorly managed revenue cycle is not always visible on a single line item. It shows up across a few different categories:
- Claim denials from incorrect coding, missing prior auth, or documentation that does not meet payer requirements.
- Revenue leakage from under-coding sessions or failing to bill eligible services, particularly common as provider rosters grow and oversight thins.
- Extended A/R aging from denials that sit unworked because the team is already at capacity.
- Write-offs from claims that age past the filing deadline because follow-up fell through the cracks.
Industry data puts revenue lost to billing inefficiencies at up to 20% of collectible revenue for behavioral health practices. For a practice billing $2 million annually, that is up to $400,000 left on the table. [2]
How you know you have hit the tipping point
Not every practice is in crisis, but most growing practices hit a threshold where their current setup is no longer sustainable. Some of the clearest signals:
- Your clean claim rate has dropped below 90%, meaning more than 1 in 10 claims need manual intervention before payment [3]
- A/R days are pushing past 40, with a backlog of denials older than 60 days that nobody is actively working
- You have added providers but billing turnaround has not kept up or has gotten slower
- Your billing team is spending most of their time reacting to problems rather than preventing them
- You cannot get a real-time read on your revenue cycle without pulling a manual report
The billing bottleneck is not just a cash flow problem. It is a capacity problem, every hour your admin team spends firefighting billing is an hour not spent on intake, scheduling, and patient experience.
The headcount trap: why hiring isn’t the answer
When revenue cycle performance starts to slip, the instinct is to add people. It feels logical that if there is more work than your current team can handle, you hire more people. But billing is not a linear problem, and headcount is not a linear solution.

What a billing hire actually costs?
The sticker price of a billing hire is the salary. The real cost is something else. When you factor in benefits, onboarding, training, the learning curve specific to behavioral health coding (which is steep), and ongoing management overhead, the fully loaded cost of a billing FTE typically runs 1.25 to 1.4 times their base salary.[4] And that is a recurring cost, regardless of whether your revenue cycle is performing well or not.
A scenario worth recognizing:
A mid-size outpatient mental health practice hired a second full-time biller after their denial rate climbed past 15%. Six months later, the denial rate was 13%, just a modest improvement. But they had added roughly $65,000 in annual payroll and still had no visibility into why denials were happening upstream. The new hire was good at reworking claims. What the practice actually needed was a system that stopped generating bad claims in the first place.
More importantly: a new hire does not fix a broken process. If claims are being denied because of upstream errors in scheduling, eligibility verification, or documentation, adding someone to work the denial queue does not solve that. It just gives you someone to clean up the mess faster. The mess keeps coming. More people, same denial rate
Here is something worth sitting with: denial prevention is not really a function of how many billers you have. Most denials originate before a claim is ever submitted as in how a session was scheduled, whether eligibility was verified, whether the clinical note met the payer’s documentation threshold, whether the right code was applied. By the time someone is working a denial, the root cause is already two or three weeks in the past.
Practices that hire their way through denial problems tend to get good at rework. They get fast at resubmitting claims and writing appeals. What they do not get is a lower denial rate. For that, you need process change; which means either better systems, better expertise, or both.
The consistency problem at scale
Behavioral health billing depends on doing the same thing the same way, every time. The same session type coded consistently across every provider, every payer, every week. Manual processes performed by multiple people introduce variation and in billing, variation is expensive.
A common scenario in multi-provider practices:
A practice with eight therapists and two billing staff discovers during a payer audit that telehealth sessions billed by three of their providers have been missing the required place-of-service modifier for six months. The sessions were delivered correctly. The clinical notes were complete. But the billing workflow had no automated check for the modifier, and nobody caught it until the audit flagged $34,000 in potential recoupment. The problem was not a shortage of billing staff. It was a lack of standardized, automated rules.
People get sick. People leave. People develop their own shortcuts. In high-volume practices, that inconsistency compounds into material revenue risk and significant audit exposure. A system that enforces rules automatically does not have bad days.
Two paths to simplifying billing without scaling your team
Once you accept that the answer is not more headcount, two real alternatives emerge. They are not mutually exclusive, and a lot of high-performing practices end up using both. But they start from different places and fit different stages of growth.
Path A: Automate in-house with an integrated RCM platform
The first option keeps billing ownership inside your organization, but replaces manual workflows with a purpose-built technology platform. A well-configured RCM system handles the repetitive, rule-based parts of billing automatically: eligibility verification at scheduling, claim building from clinical notes, submission, payment posting, and denial tracking. Your team is still involved, but they are doing oversight and exception management, not data entry and manual follow-up.
This path tends to work well for practices that want to maintain direct control of their revenue cycle, have staff who can manage a tech-enabled workflow, and are operating at a scale where internal billing oversight makes sense. The critical requirement is that the platform has to be built specifically for behavioral health and not adapted from a general medical billing system. Generic platforms do not handle time-based coding, behavioral health authorization workflows, or payer variability in the way the specialty actually demands.
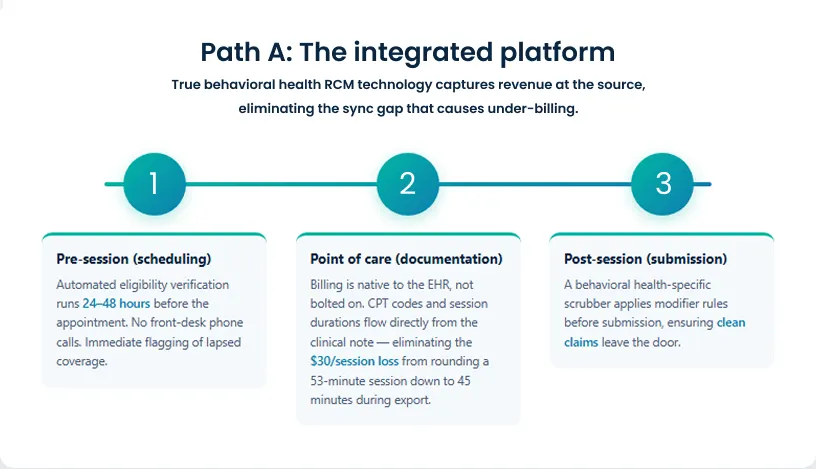
What this looks like day to day
Instead of a front desk coordinator manually calling to verify insurance before each appointment, the platform runs an eligibility check automatically when the session is scheduled and flags any coverage issues before the patient walks in the door. Instead of a therapist finishing a session and their notes being re-entered into a separate billing system, the CPT code and billing details are generated directly from the clinical documentation. The biller reviews exceptions, not every claim.
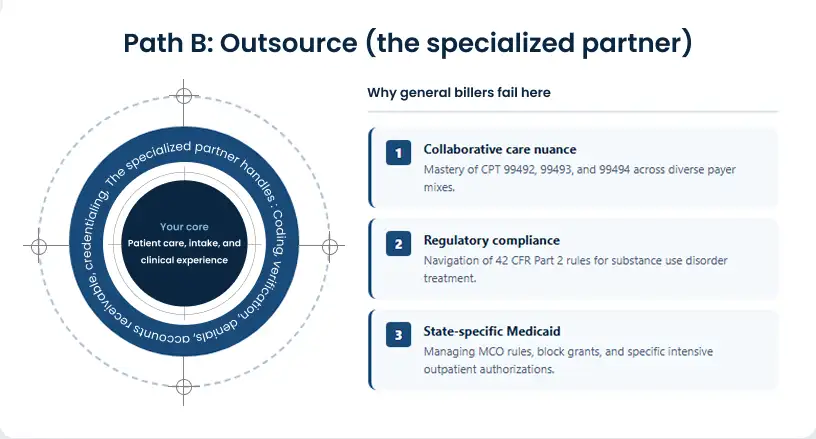
Path B: Outsource to a specialized RCM services partner
The second option transfers execution to an external team of billing specialists. Your internal staff handles the things that require human touch and local knowledge like scheduling, patient communication, intake and the RCM service provider handles everything downstream: coding, claim submission, denial management, A/R follow-up, credentialing, prior authorizations, and financial reporting.
This works best for practices that are growing faster than their admin infrastructure can keep up with, have experienced recurring revenue cycle problems that internal changes have not fixed, or simply want to remove billing as a management distraction entirely. It is also the right fit when behavioral health billing expertise is the actual gap, not just bandwidth, but specialized knowledge.
When this path fits best
A psychiatrist running a solo practice that has grown to include two associate providers finds herself spending three to four hours every Friday afternoon reviewing claims, following up on prior authorizations, and chasing payer portals. She is not a billing specialist; she is a clinician doing billing because nobody else is. Outsourcing the revenue cycle to a specialized partner does not just recover those Friday afternoons. It puts the billing function in the hands of people who do this full time, which shows up in faster reimbursements and fewer denials.
Why many practices end up choosing both
The most scalable configuration is actually a combination of the two: an integrated RCM platform that automates the process and provides real-time visibility, layered with a specialized services team that handles the complex, high-judgment work like denial appeals, payer negotiations, credentialing, and compliance oversight.
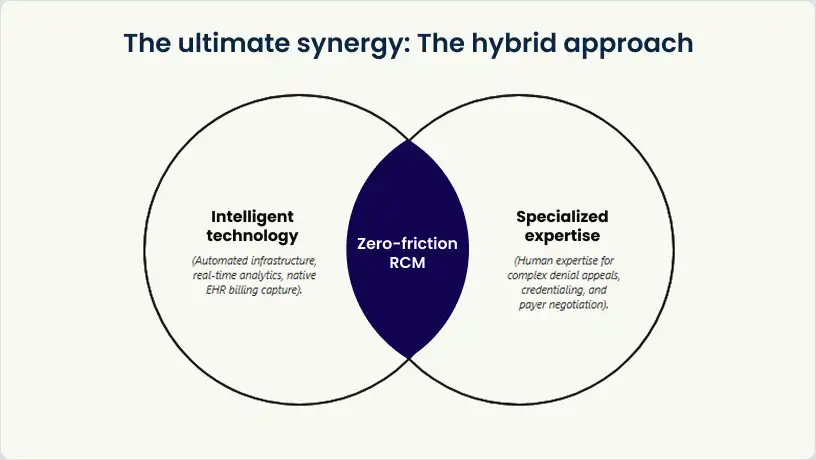
Think of it this way: the platform gives you the infrastructure, and the services partner gives you the expertise. Together, they cover both the capacity problem and the knowledge problem without proportional growth in internal headcount.
The practices that scale billing efficiently are not the ones with the biggest admin teams. They are the ones that stopped treating billing as a staffing problem.
What to look for in an RCM platform built for behavioral health
The platform evaluation is where a lot of practices get tripped up, because the market is crowded with tools that claim to handle behavioral health billing but were really built for primary care or surgical specialties. The differences matter and they show up in your denial rate, your documentation rework, and the amount of manual intervention your team still has to do even after implementation. Here is what actually separates a purpose-built behavioral health billing platform from a general-purpose workaround.
Billing built into the EHR, not bolted on
The single biggest source of behavioral health billing errors is the gap between clinical documentation and claim submission. When the EHR and billing system are two different products syncing through an integration, data gets lost, delayed, and mistranslated; especially with time-based coding, where a difference of eight minutes can mean a different CPT code and a materially different reimbursement.
Why this gap is expensive:
A therapist documents a 53-minute session in the EHR. The note is thorough and accurate. But the billing integration only syncs once a day, and during the export the session duration is rounded down to 45 minutes. The claim goes out with CPT 90834 instead of 90837; a difference of roughly $30 per session. Across 20 therapists each seeing 6 clients per day, that kind of systematic under-billing adds up to tens of thousands of dollars in annual revenue loss, all from a sync gap that a native-billing system would have prevented entirely.
A truly integrated platform captures billing data at the point of clinical documentation and flows it directly into claims without manual re-entry. No exports, no copy-paste, no re-keying session details into a separate billing screen.
Automated eligibility verification before the session, not after
Most denials for behavioral health services do not happen because of complex coding disputes. They happen because eligibility was not confirmed, an authorization had lapsed, or the patient’s coverage changed between scheduling and the appointment.
A situation most front desks will recognize:
A patient schedules a therapy session two weeks out. At the time of booking, their insurance is active and their authorization is valid. By the time the appointment rolls around, they have changed jobs and their coverage has lapsed, but nobody checks again at check-in. The session is delivered, the claim is submitted, and three weeks later it comes back denied. The practice now has to track down the patient, figure out their new coverage, and decide whether to resubmit or write it off. A platform that runs an eligibility check at the time of scheduling and again 24 to 48 hours before the appointment catches this before it becomes a problem.
Claims scrubbing with behavioral health rules
Every billing platform has some form of claims scrubbing, the automated checks that catch errors before submission. The difference is the rule set. A behavioral health-specific scrubber knows that a 45-minute therapy session cannot be billed with the same modifier as a 60-minute one. It knows which payers require specific documentation attached to specific codes. It catches modifier errors, time-based coding mismatches, and payer-specific requirements that a generic scrubber simply does not have rules for. The result is a higher clean claim rate before a human ever touches the claim.
Real-time visibility into what is actually happening
Practice leaders should not have to wait for a monthly billing report to know whether their revenue cycle is healthy. The right platform gives you a live dashboard: clean claim rate, A/R aging by payer, denial trends, days to payment, outstanding authorizations.
What good visibility looks like in practice:
A practice administrator opens her dashboard on a Tuesday morning and sees that claims submitted to one commercial payer have had a spike in denials over the past two weeks; all citing the same missing modifier. She flags it immediately, the coding error gets corrected, and the affected claims are resubmitted the same day. Without real-time reporting, this pattern might not have surfaced until the monthly A/R review three weeks later, with some claims already aging past optimal resubmission windows.
Built to scale, not just to work at your current size
A platform that handles your current 8 providers needs to handle 25 without requiring a system replacement. That means multi-location support, multi-payer flexibility, support for diverse program types IOP, group therapy, telehealth, collaborative care models and configurable billing rules that can be tailored as your payer mix evolves. If a platform cannot clearly show you how it handles growth, that is a gap that will surface at the worst possible time.
How blueBriX approaches this
blueBriX’s billing platform is built directly inside the EHR not as a separate product or third-party integration. Billing rules trigger at the point of scheduling, clinical notes sync to claims in real time, and the platform applies behavioral-health-specific scrubbing rules before any claim goes out. Eligibility verification runs automatically at scheduling. ERAs post directly to patient accounts. The analytics layer gives practice leaders a real-time view of their revenue cycle denial rates, A/R aging, payer mix, and RCM performance without waiting on a report. And the platform is designed from the ground up to support the full range of behavioral health program types and payer configurations, at any scale.
What to look for in an outsourced RCM partner for behavioral health
Choosing an RCM services partner is a more consequential decision than choosing a software platform. You are not just licensing a tool you are transferring execution responsibility for a function that directly determines your cash flow. The wrong partner introduces more risk than it removes. Here is how to think through the evaluation.
Behavioral health specialization is not optional
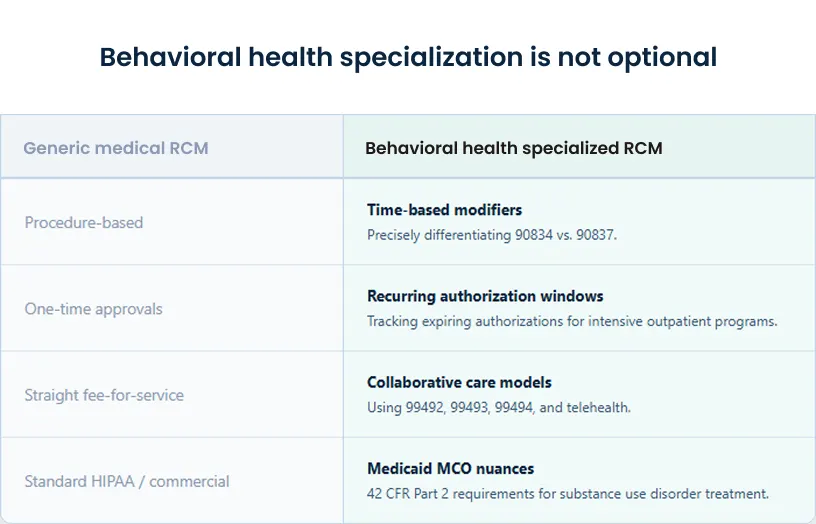
General medical billing services can process claims competently. What they consistently get wrong in behavioral health is the nuance: the difference between billing 90837 and 90834, the documentation requirements for a collaborative care model claim, 42 CFR Part 2 confidentiality rules for substance use disorder treatment, the parity compliance considerations that affect how commercial plans handle mental health claims. A partner without genuine behavioral health depth will have a learning curve and your practice pays for it in denied claims and delayed reimbursements.[5][6]
During an RCM services evaluation, ask the prospective partner to walk you through how they would handle billing for a Collaborative Care Model program. Ask how they manage CPT codes 99492, 99493, and 99494 across your payer mix, and what documentation they require from your clinical team to support those claims.[7] If the answer is vague or requires a callback, that tells you something important about whether behavioral health is a core practice or a sales expansion.
When evaluating a prospective partner, the right questions are direct ones: What share of your client base is behavioral health providers? Who on your team has hands-on behavioral health billing experience. Make sure you not just ask about general medical billing. How do you stay current with CPT updates, telehealth policy changes, and payer-specific behavioral health requirements? Vague answers are informative.
Questions worth asking every prospective RCM service provider
- What is your current clean claim rate, and how do you measure and report it?
- Walk me through your denial management process from first denial to resolution.
- What is your average time-to-payment from claim submission?
- How do you handle provider credentialing and payer enrollment for new hires?
- What does financial reporting look like and how much real-time visibility will we have?
- How do you manage prior authorization workflows, and what is your authorization tracking process?
- What does the transition look like? How do you handle data migration and the go-live period without disrupting cash flow?
Transparency should be a baseline expectation, not a differentiator
A good RCM service provider does not operate as a black box. You should have access to your own revenue cycle performance data at any point and not just when a monthly report arrives. If a prospective partner cannot show you, during the sales conversation, exactly what reporting and visibility looks like post-implementation, that is a signal worth taking seriously.
What a transparent RCM relationship looks like
A practice director whose team recently outsourced billing describes it this way: ‘I used to dread the monthly billing call because it was always a post-mortem. Now I can pull up the dashboard any morning and see exactly what was submitted, what paid, what is outstanding, and what is being worked. If something looks off, I flag it in real time and I don’t wait three weeks to find out.’ That level of access should not be a premium feature. It should be the default.
What the engagement model should look like
A strong RCM services engagement starts before any claims are touched. It begins with an audit of your current state, billing workflows, payer contracts, outstanding A/R, common denial patterns and so the partner understands exactly where your revenue cycle is losing money before designing the solution. Onboarding should be phased and supported, with a clear plan for data migration, staff transition, and go-live that does not create a gap in cash flow.
End-to-end scope matters too. Fragmented RCM services where one vendor handles coding, another handles denials, and your internal team handles credentialing will create handoff problems that cost you money. The most effective model is a single partner who owns the full cycle from eligibility verification to final payment.
How blueBriX approaches this
blueBriX’s managed RCM services cover the full revenue cycle from medical coding, insurance verification, prior authorization, charge capture, claim submission, denial management, payment posting, A/R follow-up, credentialing, to financial reporting. Every engagement starts with a free assessment of your current billing processes to identify exactly where revenue is being lost before any changes are made. The services team brings over 20 years of hands-on RCM experience and specializes in the behavioral health coding and documentation standards that determine reimbursement outcomes. Critically, blueBriX’s services run on the same integrated platform so clients get both the execution expertise and the technology infrastructure, with real-time visibility into their revenue cycle at all times.
Real outcomes: what ‘simplified billing’ actually looks like in practice
It is worth being specific about what the right setup is. Whether it is platform, services, or both. Not in general terms, but in the numbers that move and the day-to-day experience of running a practice where billing is no longer the thing that keeps you up at night.
The metrics that tell the story

When your revenue cycle is working well, these numbers reflect it:
- Clean claim rate at 95% or above. Below that, you are spending significant admin time on rework. Every point below 95% is a claim that had to be touched twice or more before it is paid.
- Days in A/R below 35. Extended A/R is a symptom. It means claims are sitting unanswered, denials are not being worked, or your follow-up process has gaps that are compounding over time.[8]
- Denial rate below 5%. The behavioral health industry average runs significantly higher. Getting below 5% requires upstream fixes eligibility, documentation, and coding accuracy.[9]
- Net collection rate at 96–98%. This is how much of your collectible revenue you are actually collecting. Gaps here often trace back to write-offs that did not have to happen.
What it feels like when billing is no longer the problem
The numbers matter, but so does the operational experience. When billing is working, clinical staff are not being pulled into documentation re-dos. Front desk staff are not fielding insurance calls that should have been resolved at scheduling. Practice managers are not compiling A/R reports manually or fielding questions from providers about unpaid claims.
What the shift looks like for a practice manager
Before: Monday mornings start with a stack of denial notices to sort through, a list of authorizations expiring this week that nobody has renewed yet, and a provider asking why a claim from six weeks ago still has not paid. The day is reactive before it has even started.
After: The dashboard shows three claims flagged for review, two authorization renewals due by Thursday, and a payer that has been slow to process all visible before the first patient arrives. The work is still there, but it is manageable, visible, and proactive.
That recovered time and attention flows back into what actually drives practice growth: intake capacity, provider retention, referral relationships, and patient experience. For many practice leaders, this is the more meaningful outcome not just better KPIs, but a fundamentally different way of running the organization.
Choosing the right fit: platform, service, or both
The right answer depends on three things: your current scale, your internal capabilities, and how much of the billing function you want to own versus hand off. Here is a practical framework for thinking it through.
Matching the model to your stage
- Solo and small practices (1–5 providers): The priority here is getting billing right without building a billing department. An integrated RCM platform that automates eligibility, claims, and payment posting eliminates the most common sources of revenue leakage without significant admin investment. Outsourced RCM services are also a strong fit particularly for clinician-owners who are spending hours each week on billing they never trained for and do not want to manage.
- Mid-size growing practices (6–20 providers): This is the stage where billing complexity most often outpaces existing capacity. You likely have some billing infrastructure in place, but it is showing strain. The hybrid model integrated platform for automation and visibility, supported by outsourced expertise for denial management, credentialing, and complex A/R is typically the most effective configuration here. It preserves oversight without requiring you to keep building the internal team.
- Multi-site organizations (20+ providers, multiple locations): At this stage, billing complexity is structural. Varied payer mixes across locations, multiple program types, multi-location credentialing needs, and value-based care contracts all require a system designed to handle complexity at volume. A fully integrated platform with enterprise-grade analytics, combined with a full-cycle RCM services partner, is the configuration that supports growth without creating billing chaos.
What transition actually looks like
One of the most common reasons practice leaders delay an RCM decision is fear of disruption. Mid-flight changes to billing processes carry real risk if not managed carefully nobody wants a gap in claims submissions while switching systems or onboarding a new partner. That concern is legitimate.
But it is worth weighing against the alternative. Every month your practice runs on a billing setup that is underperforming is a month of compounding revenue leakage, growing denial backlogs, and admin overhead that does not go away on its own.
What a managed transition typically involves
A well-run onboarding starts with a current-state audit. Data migration is handled end-to-end, including patient records and billing history. Claims submissions continue without a gap during go-live. And for the first 30 to 60 days, there is a dedicated implementation contact whose job is to make sure nothing falls through the cracks during the transition. The question to ask any prospective partner or platform is not ‘can you migrate us?’ It is ‘what does your go-live process look like, and what happens if something goes wrong?
The question is not whether you can afford to change your billing setup. It is whether you can afford to keep running on the one you have.
Ready to see what your revenue cycle could look like?
blueBriX works with behavioral health practices at every stage of growth — as a technology platform, a managed RCM services partner, or both. Start with a free RCM assessment to see exactly where your revenue cycle is losing money. Book a free consultation now.
Book a free consultation now