The medication administration record: why it's under more pressure than ever
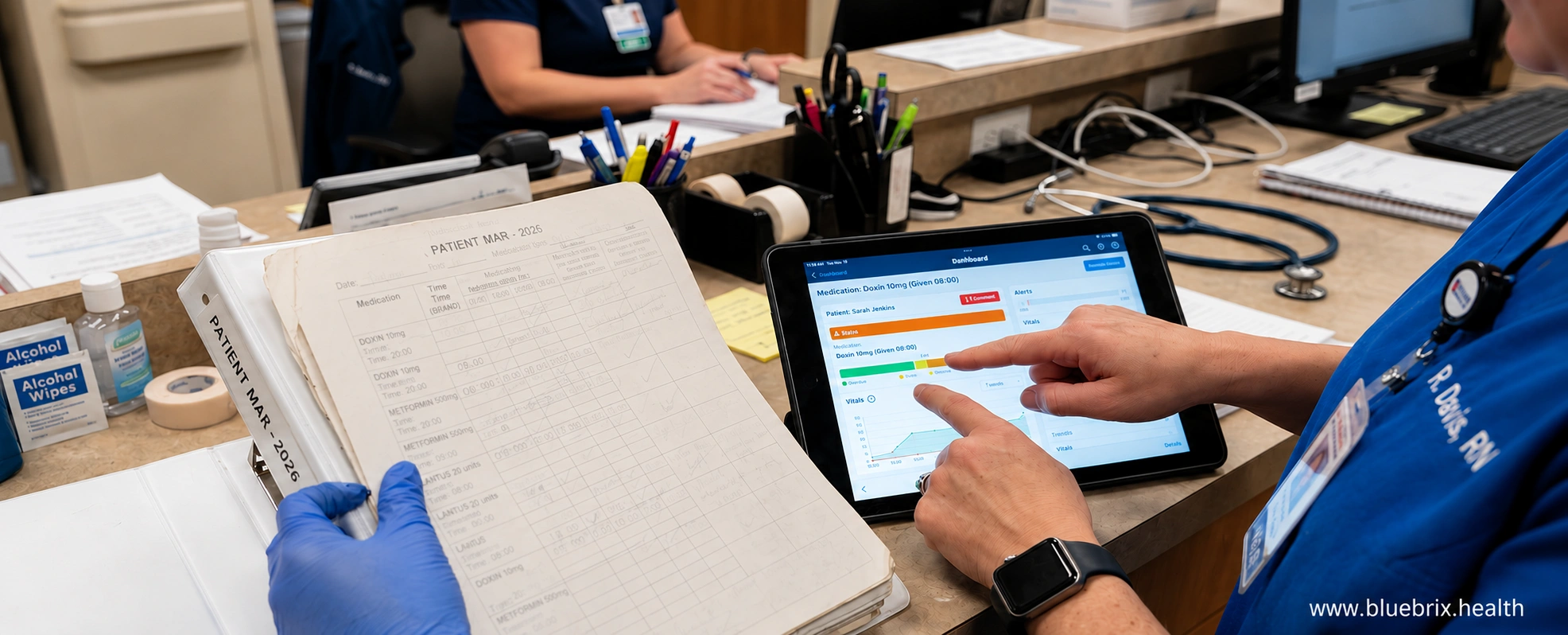
Medication administration is one of the most high-stakes workflows in any clinical setting. And for a large number of facilities across the US, it still runs on paper.
Paper MARs get the job done until they don’t. A missing signature, an illegible entry, a refill that fell through the cracks between shifts, a renewal that expired without anyone catching it. These are the everyday realities of a paper-based system operating inside a clinical environment that demands precision.
The risks are real, well-documented, and growing as staffing pressures increase, regulatory scrutiny tightens, and the margin for documentation error narrows.
What’s less often examined is the deeper question sitting underneath all of it: when a paper MAR fails, who actually owns that failure?
This blog unpacks that question, walks through the real risks living inside paper-based medication administration, and explores what facilities are doing to get ahead of it. blueBriX has worked closely with clinical teams navigating exactly this shift, and what we’ve seen on the ground shapes much of what follows.
To understand why this matters now more than ever, it helps to look at what the regulatory environment is demanding from facilities today.
Why the window for paper-based MAR is closing
CMS has already raised the bar on long-term care documentation. In 2025, revised surveyor guidance took effect across nursing homes and other LTC settings, with stronger expectations around nursing services, medication regimen review, and psychotropic medication documentation. That means surveyors are now looking at medication records through a stricter lens than they were a year ago.
For facilities still using paper MARs, the problem is not that paper is automatically noncompliant. The problem is that paper depends entirely on manual effort. Every dose, change, review, follow-up, and signature has to be entered correctly, kept current, and defended later if questioned. That creates more room for missed documentation, delayed updates, and inconsistencies that can become survey findings.
The pressure is also increasing from other directions. Medication-related citations remain a major compliance concern, and the survey process is increasingly focused on whether the record clearly shows that medications were appropriate, reviewed, and monitored. At the same time, broader healthcare documentation is moving toward electronic, auditable systems that leave less to memory and less to reconstruction after the fact.
For LTC administrators, the takeaway is simple: the regulatory environment is getting less forgiving, not more. A paper MAR may still be usable, but it is becoming harder to defend because it does not automatically produce the level of detail, traceability, and real-time visibility that current compliance expectations demand.
But regulation is only part of the picture. The more immediate problem is what happens inside the workflow itself, on every shift, across every resident record, every day.
The real challenges inside a paper-based MAR
The risks inside a paper-based medication administration system are not always dramatic or visible. Most of them are quiet, recurring, and structural. Here is what they actually look like on the ground.

Medication errors
This is where the upstream failures land. An illegible entry that was misread, a previously administered dose that was not signed and therefore assumed to be missed, or a discontinued medication that was not clearly crossed off; each of these creates the conditions for a medication error.
What makes paper particularly vulnerable here is that the record and the error exist in the same physical object. There is no independent system log, no timestamp from a separate platform, and no audit trail that is separate from the document itself. The only account of what happened is the MAR, and if the MAR is flawed, the account of the error is flawed with it.
Duplicate dosing, omitted doses, wrong medication, or the wrong route are not hypothetical risks in paper-based settings. They are documented outcomes tied directly to documentation failures.
Delayed medication administration
In a paper-based system, a nurse managing multiple residents has no prompt when a dose is due, no alert when a window is approaching, and no way to distinguish at a glance what has been given from what is still pending. Tracking medication timing depends entirely on memory and a handwritten record.
During a high-pressure shift, that is not enough. An unsigned entry leaves the next nurse unable to tell whether a dose was given and not documented, or simply not given. A PRN medication gets administered twice because the first entry was not immediately visible. A critical dose gets missed with no system to flag the omission.
These are failures of a system that gives providers no real-time support for tracking medication administration as it actually happens.
The prescription-to-administration gap
What a physician orders and what physically arrives at the bedside are not always the same thing. A provider orders 30mg of a medication. No 30mg tablet exists. The pharmacist fulfills it using two separate pill cards. The order was right, the dispensing was right but if the MAR only reflects what was prescribed, the nurse sees “30mg” and nothing more. No indication of two cards. No notation on how the dose was physically constructed. That space between the prescription and the administered dose is where quiet errors originate.
When the information chain breaks between prescribing and administration, the nurse at the end of the shift is left filling in the blanks and that is not a safe place to leave a clinical decision.
Communication collapse — missed renewals and refills
This is the most underappreciated risk in paper-based medication administration, and it is also the most preventable with the right system.
Medication orders have expiration dates. Controlled substances require renewal within strict windows. PRN medications need periodic clinical review. Refills require coordination between the facility, the prescriber, and the pharmacy. In a paper system, all of that coordination depends on human memory, verbal handoffs, phone calls, and manual tracking.
There is no automated alert when an order is approaching expiration. No system flag when a medication supply is running low. No integrated view that shows the nurse, the pharmacist, and the prescriber the same real-time picture at the same time.
What happens in practice: a nurse reaches the last dose and assumes the refill was ordered. A physician’s order expired three days ago and the renewal request was lost in a shift change. A controlled substance window lapses over a weekend when the prescriber is unreachable. A patient goes without a critical medication not because anyone decided to stop it, but because the communication chain that paper depends on quietly broke down.
These challenges do not always show up together, and they do not always escalate in the same way. But they share a common root: a paper-based system that was never designed to handle the documentation demands of modern medication administration. Each one represents a gap that clinical teams are left to manage manually, and that surveyors and attorneys are trained to find.
Illegible handwritten notes
Everything in a paper MAR starts with a handwritten entry. Handwriting under clinical pressure, whether during a busy shift, across a twelve-hour rotation, or at the end of a double, is not reliable. Drug names get abbreviated differently by different nurses. Doses get written in ways that read as two different numbers depending on who is reading them. Routes get assumed rather than clearly noted.
The problem is not the nurse. The problem is that paper offers no correction layer. An illegible entry sits in the record exactly as it was written, and the next person to act on it works from their interpretation, not the original intent.
A common example: a handwritten entry for “10 units” of insulin misread as “20 units” during a rushed shift handoff. There is nothing in the paper system to catch that before it reaches the patient.
Missing reviews and signatures
A signature on a MAR is the only documented proof that a medication was reviewed and administered. When it is missing, the clinical record reflects that the medication was not given, regardless of what actually happened.
In a paper environment, these critical gaps in reviews and signatures accumulate without any visibility. There is no alert when an entry is left unsigned or when a required clinical review is bypassed. No report surfaces the gap at the end of a shift, and there is no dashboard showing which entries are incomplete. The binder sits at the nurses’ station and the gap sits inside it, invisible until someone specifically looks.
By the time a surveyor or an auditor looks, there may be dozens of missing reviews or unsigned entries across a thirty-day period. Each one is a documentation deficiency. Each one is indefensible without a system that can corroborate what actually happened.
These challenges exist across clinical settings. But in behavioral health environments, the documentation stakes are layered with additional legal and clinical complexity that deserves its own attention.
MAR: the legal implications in behavioral health
In behavioral health, the Medication Administration Record (MAR) carries a weight that standard clinical settings rarely experience. Here, the MAR isn’t just a log of pills—it is the primary legal document for patient stability and rights.
The “unnecessary medication” defense
Under CMS F758, psychotropic medications must be tied to a specific diagnosed condition and documented in the resident’s clinical record. Surveyors look for evidence of the behavior or symptom being treated, the rationale for the medication, and whether behavioral interventions were tried or were clinically inappropriate. In a paper MAR system, if a PRN dose is signed off without clear context, the record may appear incomplete and can raise concerns about unnecessary medication use.
Side-effect monitoring and liability
High-risk psychotropic medications require ongoing monitoring for adverse effects such as involuntary movements and metabolic changes. In long-term care, the medication record should be connected to clinical follow-up so the facility can show not only that the drug was administered, but also that its effects were being watched over time. That means the MAR should not stand alone; it should be supported by assessment notes, monitoring results, and timely clinical review.
For example, if a resident is receiving an antipsychotic, the facility should be tracking for movement-related side effects such as tremors, stiffness, or tardive dyskinesia, often using tools like AIMS. If a resident is on a second-generation antipsychotic, the team may also need to monitor weight, blood sugar, and lipids because these medications can affect metabolism. When that monitoring is not documented clearly, the facility may have trouble proving that the medication was used safely and appropriately.
The consent and compliance trap
In some states and behavioral health settings, psychotropic medications require current informed consent. If a drug is given after that consent has expired, the MAR may show the dose was administered, but the facility may still be out of compliance because the legal authorization was no longer valid. In that sense, the MAR must line up with the consent record in real time.
For instance, if a resident is given risperidone for agitation, the facility may need a valid consent form on file before giving it.
Now let’s look at what these documentation gaps actually cost a facility when they surface outside the clinical workflow.
How MAR failures affect revenue
Documentation failures in medication administration rarely stay contained to the clinical workflow. They have a way of surfacing exactly where facilities can least afford them in survey outcomes, courtrooms, staffing budgets, and reimbursement reports.
Survey outcomes and star ratings
Medication management deficiencies consistently rank among the most frequently cited F-tag violations during CMS surveys. And the damage doesn’t stop at a corrective action plan.
Every citation feeds directly into a facility’s five-star quality rating, a number that prospective residents, their families, and referring physicians all look at. A lower rating reshapes public perception, shrinks referral volume, and ultimately puts occupancy at risk. In an industry where census is the foundation of revenue, a ratings drop triggered by a documentation gap isn’t a compliance issue. It’s a business crisis that starts with a missing signature.
Litigation exposure
Medication errors are one of the leading sources of malpractice claims in long-term care. When a claim is filed, the MAR is the defense.
A paper record with illegible entries, unsigned doses, or unexplained gaps tells a story in court. Not the one you want told. Plaintiff attorneys know how to read a MAR, and so do juries. What follows isn’t just a lost case; its legal fees, settlement costs, and insurance premiums that quietly climb year over year. The paper record that seemed manageable in the moment becomes extraordinarily expensive in hindsight.
Operational inefficiency
Consider what actually happens during a shift when a paper MAR has a discrepancy. A nurse stops direct care to investigate an unsigned dose. A charge nurse spends time reconciling entries before the next administration window. A coordinator chases down a medication renewal that should have flagged automatically.
Multiply that across a week, a month, a quarter and the labor costs are significant. The trouble with paper-based administrative overhead is that it normalizes quickly. Staff adapt to the friction, build workarounds, and absorb the inefficiency as routine. It disappears from view, right up until someone does the math and realizes how much clinical time is being spent managing a records problem instead of patients.
The risk here isn’t theoretical. It has a dollar figure attached to it in survey citations, in legal exposure, in lost census, and in reimbursement penalties. What often gets treated as a workflow inconvenience is, in practice, one of the more consequential operational vulnerabilities a facility carries.
Understanding the risk is the first step. The more useful question is what the right documentation system actually looks like when it is working the way it should.
MAR documentation best practices: what a complete record actually looks like
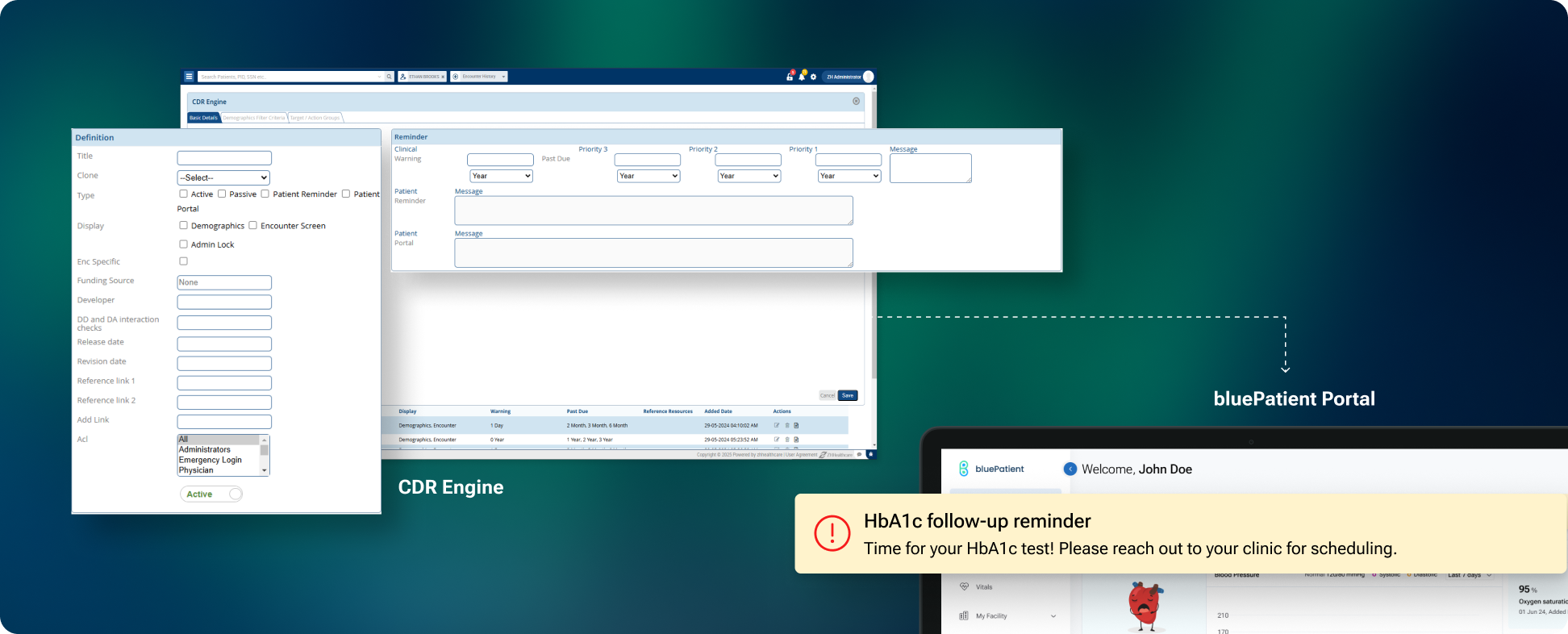
Facilities that have moved away from paper are replacing a passive document with an active system. A modern EHR does not treat the MAR as a standalone form. It treats it as a live, connected workflow that captures the right information from the right people at the right time and makes it available to everyone who needs it.
Here is what complete, defensible MAR documentation looks like inside a capable EHR system.
Every entry captures who, what, when, and how
A properly structured MAR entry records the medication name, dose, and route along with the exact date and time of administration. Not an approximate time slot. An actual timestamp. For time-sensitive medications, this distinction is clinically and legally significant.
Administrator identity is always on record
Every entry is tied to the individual who administered the medication. Not a shift, not a unit, but a specific named and credentialed staff member. This creates accountability that a handwritten initial on a paper form simply cannot provide.
Verification is documented, not assumed
Who reviewed the order before administration? Who verified the dose? In a complete documentation system, the verification step is a recorded action. This protects the nurse, the facility, and the integrity of the record.
Pharmacist instructions are embedded, not separate
Dispensing notes, administration instructions, and pharmacist guidance live inside the medication record, not in a separate binder, a sticky note, or a verbal handoff that may or may not be passed on accurately.
Renewal and expiration alerts are automatic
Every medication order has an expiration date. When that date is getting close, the nurse gets an alert. That triggers the renewal request to the prescriber. Once the prescriber approves, the pharmacy receives the updated order and prepares the medication. Each step moves automatically to the next with no phone calls, no manual follow-ups, no information getting lost between shifts.
Real-time status across every shift
At any point during a shift, a supervisor or administrator can see exactly which medications have been administered, which are pending, and which have been missed or delayed. There is no waiting until the end of a shift to find gaps. No reconstructing a timeline after the fact.
A complete audit trail, always ready
Every action taken on a medication record including administration, verification, modification, and renewal is logged with a timestamp and a user identity. When a surveyor walks in or a legal question is raised, the documentation is complete, organized, and instantly accessible.
Behavioral justification is captured, not assumed
For psychotropic PRN medications, the system captures the clinical context behind every administration, including the behaviors observed, the interventions attempted before the medication was given, and the justification for its use. This is what surveyors are looking for under F-Tag 758. A paper MAR captures the dose. A proper system captures the reasoning behind it.
Side-effect monitoring is connected to the medication record
For high-risk medications that require ongoing monitoring, the system links the administration record directly to the required assessments. When a medication that requires AIMS tracking or metabolic monitoring is documented as administered, the corresponding assessment is prompted within the same workflow. Clinical observations are recorded against the medication, not in a separate folder. This means the connection between what was given and how the patient responded is always visible in one place, not pieced together across multiple documents.
Consent validity is tracked alongside administration
When informed consent for a psychotropic medication is approaching expiration, the system flags it before the next administration. In behavioral health settings where consent is a legal prerequisite, a lapsed consent turns a documented administration into a documented violation. Paper has no mechanism to prevent that. A structured system does.
Taken together, these capabilities represent what modern medication administration documentation should look like across any care setting.