What are ASAM criteria and why do they govern your operations?
The American Society of Addiction Medicine (ASAM) has published the national standard for SUD treatment decisions since 1991. The ASAM Criteria define how providers should assess patients, determine appropriate levels of care, make continued-stay decisions, and plan transitions and discharge[1]
They matter operationally for three reasons.
- More than 30 states require licensed SUD providers to use ASAM criteria as the clinical basis for treatment decisions.
- Every major commercial payer — UnitedHealthcare, Anthem/Elevance, Cigna/Evernorth, HCSC Blue Cross Blue Shield plans — uses ASAM as the medical necessity standard for prior authorization and concurrent review.
- ASAM level-of-care designations map directly to the billing codes used to claim for SUD services. When the documented clinical justification does not support the ASAM level being billed, claims face denial or recoupment.
For behavioral health organizations that treat substance use disorders, ASAM is not a clinical reference document. It is the operating framework for admissions, treatment planning, authorization management, and revenue cycle.
How ASAM criteria work: the six assessment dimensions
ASAM uses a multidimensional assessment model. Rather than basing level-of-care decisions on diagnosis alone, clinicians assess the patient across six dimensions[2] and weigh the combined picture to determine appropriate placement.
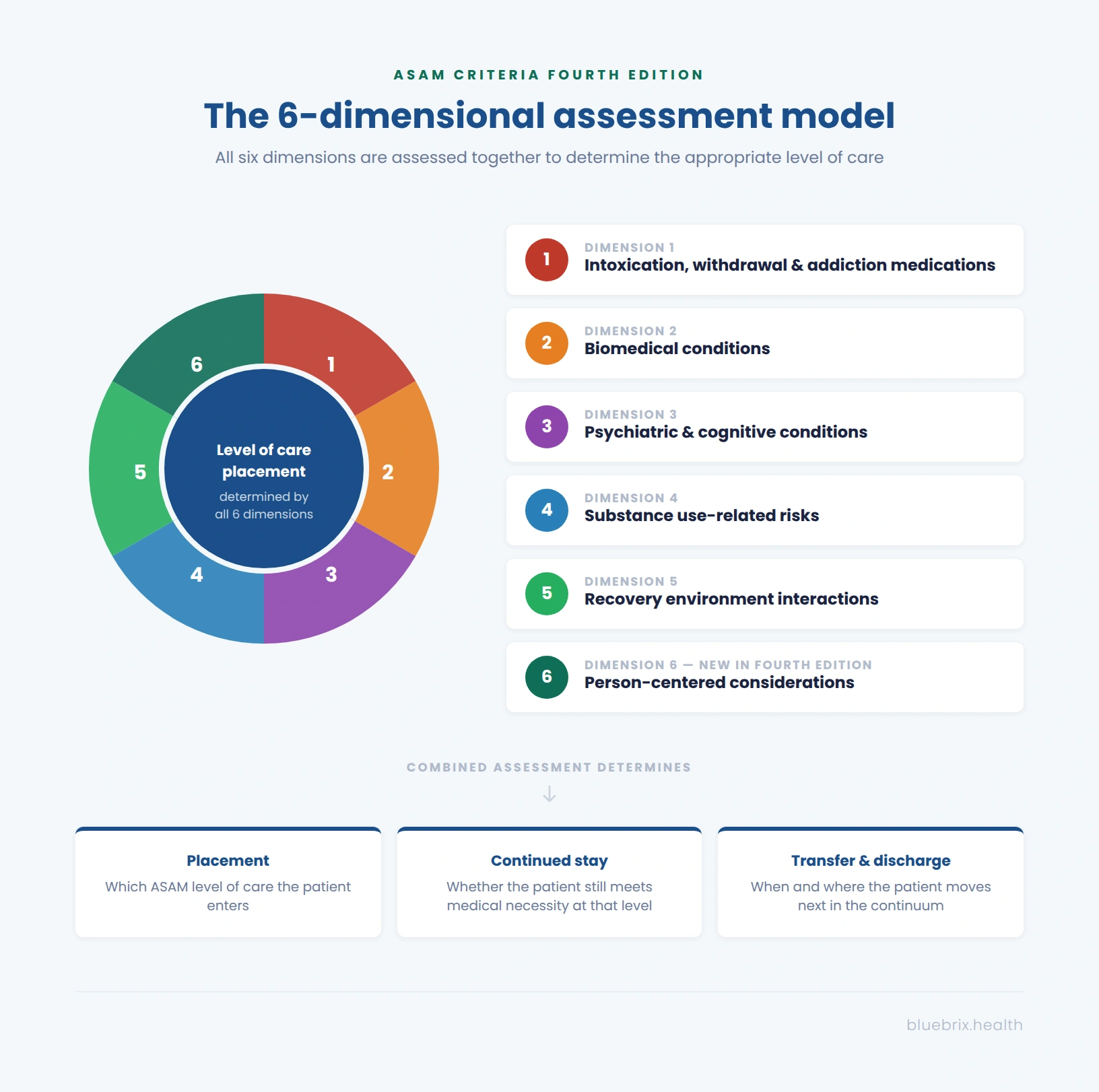
The six dimensions in the current Fourth Edition are:
- Dimension 1 — Intoxication, withdrawal, and addiction medications: acute substance use and withdrawal risk, and the patient’s current medication needs.
- Dimension 2 — Biomedical conditions: physical health status, chronic or acute medical conditions that affect treatment setting or intensity.
- Dimension 3 — Psychiatric and cognitive conditions: co-occurring mental health diagnoses, cognitive functioning, and psychiatric stability.
- Dimension 4 — Substance use-related risks: patterns of use, relapse history, and functional impairment attributable to substance use.
- Dimension 5 — Recovery environment interactions: the patient’s home, social, and community environment and whether it supports or undermines recovery.
- Dimension 6 — Person-centered considerations: patient preferences, motivation, barriers to care, and social determinants of health. Added in the Fourth Edition using a shared decision-making framework.
Each dimension contributes to the level-of-care recommendation. A patient with stable Dimensions 1 through 3 but a high-risk recovery environment (Dimension 5) may need residential care not because of medical severity, but because their home environment makes lower-intensity settings clinically unsuitable. Payers expect to see this reasoning documented explicitly — not just a diagnosis and a level.
ASAM levels of care: what each level means
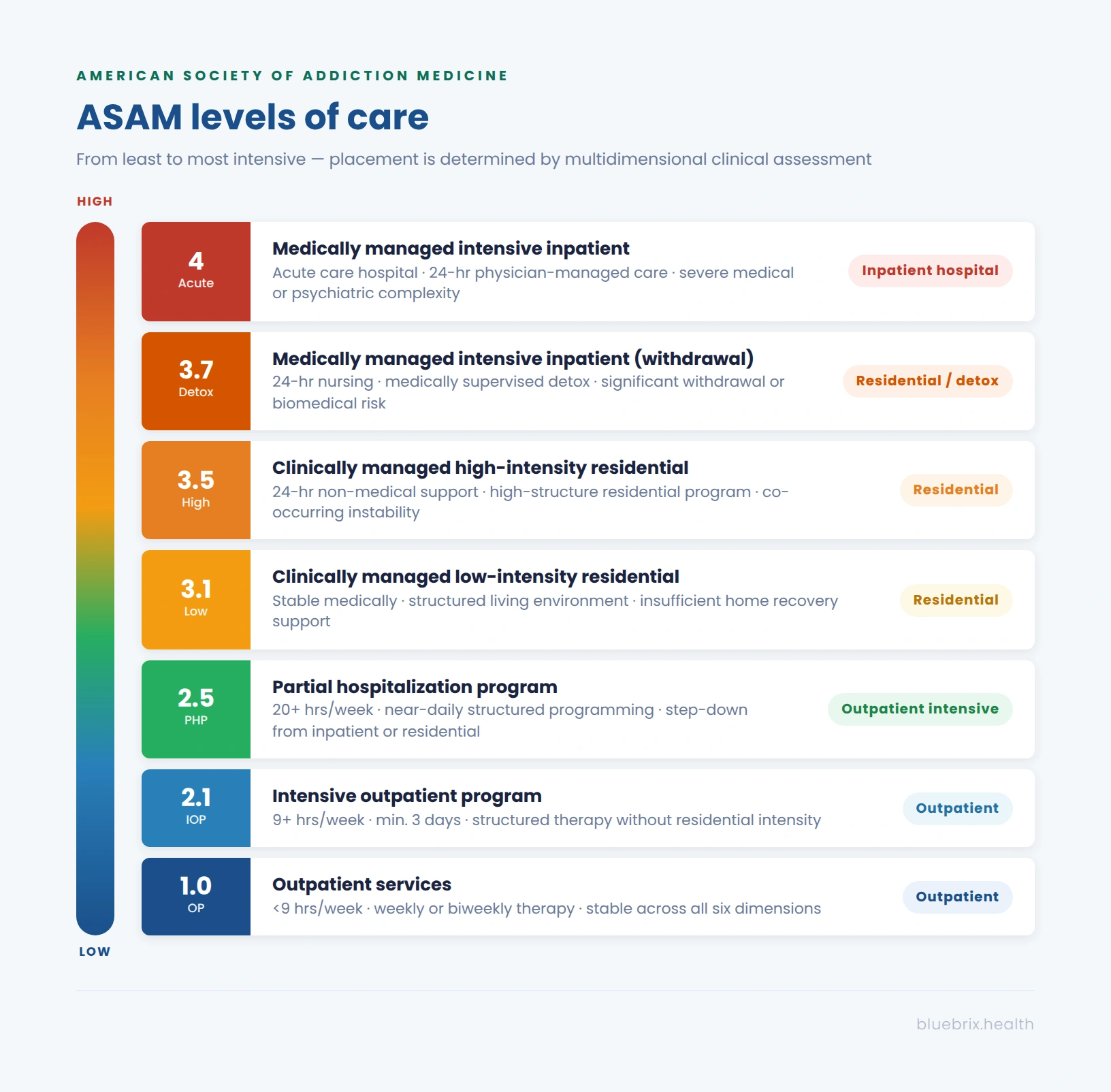
ASAM defines six broad levels of care, each with defined service characteristics, staffing requirements, and clinical criteria. [3]
Level 0.5 — Early intervention
Early intervention is not technically part of the specialty addiction treatment continuum under the Fourth Edition (see below), but it remains a licensed service level in many states. It targets individuals who show signs of problematic use but do not yet meet the diagnostic threshold for a moderate or severe SUD. Services focus on education, brief intervention, and motivational engagement.
Level 1.0 — Outpatient services
Standard outpatient treatment provides fewer than 9 hours of service per week. It is appropriate for patients with stable medical, psychiatric, and recovery environment status who can maintain progress with weekly or biweekly structured therapy. This level is rarely subject to prior authorization by major payers but requires a documented clinical assessment supporting the placement.
Level 2.1 — Intensive outpatient program (IOP)
IOP provides at least 9 hours of structured treatment per week across a minimum of 3 days. It is appropriate for patients who need more structure than standard outpatient therapy but do not require residential or partial hospitalization intensity. IOP is one of the most common levels of care in SUD treatment and one of the most closely reviewed by payers. Prior authorization is required by virtually all major commercial payers, and concurrent review is typically required every 5 to 10 sessions. Billing code: H0015 (SUD-focused, per diem) or S9480 (mental health IOP).
Level 2.5 — Partial hospitalization program (PHP)
PHP provides 20 or more hours of structured treatment per week across five days. It is appropriate as a step-down from inpatient or residential care for patients who have achieved medical stability but still need near-daily structured monitoring. Initial authorization requires documentation that the patient would require inpatient hospitalization without PHP-level care. Concurrent review is typically required every 5 to 7 days. Billing codes: S9484 or H0035, depending on the payer contract.
Level 3 — Residential treatment
Residential encompasses three sub-levels: Level 3.1 (clinically managed low-intensity), Level 3.3 (clinically managed population-specific), and Level 3.5 (clinically managed high-intensity). The appropriate sub-level depends on the patient’s medical and psychiatric complexity and the intensity of clinical oversight required. Billing codes: H0018 (short-term residential, per diem) and H0019 (long-term residential, per diem). H0017 was introduced in 2024 for programs of 30 days or fewer, though payer adoption varies.
Level 3.7 — Medically managed intensive inpatient (detox)
Level 3.7 is the most intensive residential level, providing 24-hour medically managed care for patients with significant withdrawal risk, acute biomedical comorbidity, or serious psychiatric instability. The Fourth Edition clarified that Level 3.7 is appropriate not only for withdrawal management but also for managing acute medical and psychiatric conditions across Dimensions 1 through 3. Concurrent review cadence is typically every 3 to 5 days for major payers.
Level 4 — Medically managed intensive inpatient (acute care)
Level 4 is reserved under the Fourth Edition for acute care general hospitals only. The Fourth Edition introduced a separate Level 4 Psych designation for freestanding psychiatric hospitals treating patients with co-occurring SUD, with updated codes to distinguish this from general acute medical inpatient care.
What the Fourth Edition changed: a brief overview
ASAM released the Fourth Edition in October 2023 — the first major update in a decade, developed with a formal evidence review methodology and published in partnership with the Hazelden Betty Ford Foundation[4].For behavioral health organizations, four changes have direct operational implications.
- Dimension 4 was removed [5]. as a standalone level-of-care driver. The Third Edition’s Dimension 4 (Readiness to Change) no longer generates its own independent placement signal. Readiness to change is now integrated into clinical judgment across all dimensions rather than being assessed separately.
- A new Dimension 6 was added. Person-centered considerations covering barriers to care, patient preferences, motivation, and social determinants of health, is now a required part of the multidimensional assessment [6]. It uses a shared decision-making framework: the clinician and patient work together to identify which level of care the patient is willing and able to engage with. Payers using the Fourth Edition expect to see this dimension documented in the treatment plan and concurrent review.
- Level 0.5 was removed from the specialty addiction treatment continuum. Early intervention services are no longer a distinct specialty level. In states like Illinois, they remain authorized under a Level 1.0 license.[7].
- A chronic care model replaced the episodic treatment framework. The Fourth Edition organizes the entire continuum around the understanding that SUD is a chronic condition requiring ongoing management, not an acute episode with a defined end point. Recovery support services, harm reduction, and post-discharge monitoring are now built into the standards at every level of care — not just at discharge planning.
Payer adoption is already underway. Optum Behavioral Health (United Healthcare) began applying the Fourth Edition to commercial health plans in November 2023.[8]HCSC Blue Cross Blue Shield plans covering Illinois, Texas, Oklahoma, New Mexico, and Montana moved to the Fourth Edition for adult SUD treatment on January 1, 2025. [9] Kentucky and Illinois have formally adopted it for Medicaid, effective July 1, 2025. [10]Colorado[11] and Oregon [12]have set July 2027 adoption dates. Washington has set January 2028 [13].
What this means for your EHR and documentation workflows
ASAM criteria create a documentation obligation at every stage of the treatment episode — intake assessment, prior authorization, treatment planning, concurrent review, level-of-care transitions, and discharge. The clinical reasoning captured across the six dimensions is not just a clinical record; it is the authorization justification, the billing support, and the audit trail.
Most general-purpose EHR platforms were not built with ASAM levels of care as a core workflow concept. Clinical staff end up adapting generic templates to ASAM documentation requirements, with no mechanism in the platform to flag incomplete dimensional documentation, approaching concurrent review deadlines, or level-of-care changes that need to be logged against an active authorization.
blueBriX is built for behavioral health from the ground up. Its program management, referral, treatment planning, and AI orchestration layers are designed to work together — and for SUD programs, they configure into an end-to-end ASAM-aligned workflow with minimal setup, available to demonstrate in a live session.
The referral engine can be configured to route patients based on documented ASAM scores assigned during the encounter. When a clinician assigns an ASAM score at intake, the platform uses that score to identify and direct the patient to the appropriate program — detox, residential, IOP, or PHP — rather than relying on a manual handoff that lives outside the system.
The Program Management Engine defines the rules for each program type. For ASAM-aligned implementations, each level of care is set up as a distinct program with its own enrollment criteria, care team configuration, authorization requirements, and billing strategy — per diem for residential and IOP, fee-for-service where applicable — so the clinical and billing logic for each ASAM level is built into the program itself, not managed in a spreadsheet alongside it.
The Treatment Plan Builder links treatment plans to the specific program and subprogram a patient is enrolled in. Goals and interventions are tied to the program-level clinical framework rather than floating as generic objectives, which means the treatment plan can be structured to reflect the dimensional needs driving the authorization — the connection payers look for when reviewing concurrent stay.
The AI orchestration layer operates on a human-in-the-loop model throughout: AI suggests, the platform validates, the clinician decides. For ASAM workflows, this means clinical decision support and task management can surface documentation gaps, upcoming review deadlines, and level-of-care transition prompts within the care team’s existing workflow — before they become authorization problems.
If ASAM-aligned workflows are a priority for your program, we can show you exactly what that looks like.
See how ASAM-aligned workflows work in practice
If your program is operating on a general EHR or a platform that was not built for behavioral health, the documentation gap between what you’re recording and what payers now expect — especially under the Fourth Edition — is worth assessing before your next contract renewal or payer audit. Request a workflow review. Our team will walk through your current documentation practices against ASAM Fourth Edition standards and your payer mix and show you specifically what a compliant, denial-resistant workflow looks like inside blueBriX.
Request a demo