The decision is made; now comes the harder part
The contract is signed and the strategy work is done. What replaces it is operational. A panel of attributed beneficiaries shows up needing active care management. Quality measures start scoring against clinical work that must be documented as it happens, not reconstructed after the fact. Care transitions begin generating the high-cost utilization the contract was meant to prevent. The performance period does not wait for the infrastructure to catch up.
Part 1 of this series gave behavioral health leadership teams a framework for choosing between ACO LEAD and MSSP: benchmarking mechanics, risk adjustment methodology, eligibility thresholds, and the financial logic that makes LEAD’s non-rebasing structure particularly compelling for SMI and SUD panels. If you have not read it, start there.
Part 2 picks up where Part 1 ends. Most behavioral health-aligned organizations that underperform in their first year under value-based contracting do not underperform because they chose the wrong model. They underperform because they underestimated the distance between where their systems are today and what value-based care demands from day one. The model you chose determines your financial architecture; the infrastructure you build determines whether you perform within it.
What “infrastructure readiness” actually means under LEAD and MSSP
For organizations entering ACO LEAD, January 1, 2027 is a hard go-live. The implementation period from September through December 2026 is for alignment activities, beneficiary attribution review, governance setup, payer coordination, and care team orientation. It is not for infrastructure build. By the time the implementation period opens, the platform decisions have to be settled, the integration work has to be underway, and the configuration work has to be scoped. A unified patient record connecting behavioral health and physical health data, behavioral health-weighted risk stratification, point-of-care quality capture, and closed-loop care coordination workflows all have to be operational at PY1 day one. Anything still being built after January 1 is being built under live performance pressure, against a benchmark that is already being measured and a quality scorecard that is already accumulating.
For organizations already in MSSP, the timeline pressure is different but the infrastructure agenda is the same. MSSP’s rebasing logic means every year of strong performance raises the benchmark that future agreement periods are measured against, which makes performance improvement structurally harder over time, not easier. APP Plus quality reporting has been mandatory since PY2025, so retrospective quality capture is no longer viable as an operating model. And every quarter spent on incomplete care coordination or under-configured risk stratification is a quarter of avoidable cost that flows directly through to the shared savings calculation. The infrastructure agenda for an MSSP strengthener mirrors the agenda for a LEAD entrant; the urgency is different but not lower.
What follows are the four infrastructure capabilities that determine whether either path generates shared savings, the failure mode that breaks each one when it is missing, and the order in which to build them.
A unified longitudinal patient record and care team workbench
Under LEAD or MSSP, the foundational requirement is a single view of every patient: behavioral health encounters, physical health data, SDOH information, care team activity, and quality gap status, in one place, updated in real time, and accessible to every role on the care team that needs it. This is not an integration project that can be deferred to year two. Every downstream capability, risk stratification, quality capture, care coordination, revenue cycle, depends on the patient record being complete and current on day one of the performance period. The same record also has to function as the care team’s shared workbench, because data unification without workflow unification just creates a better-looking version of the same handoff failures.
When the record is fragmented, the failure mode is consistent and expensive. Care coordinators document care after the fact because they cannot see across systems while it is happening. Quality gaps surface in quarterly reports rather than at the point of care, where they could still be closed. Care transitions, the highest-risk moments in behavioral health populations, fall between roles because no one role owns the complete view. Referrals go untracked. Post-discharge windows close without follow-up. Care team capacity is the operational constraint that decides whether a value-based program is scalable, and capacity is destroyed when coordinators spend hours stitching together information from three systems instead of managing patients. In a behavioral health-aligned panel, fragmentation is not an operational inconvenience; it is the mechanism by which shared savings are lost.
blueBriX is built around a unified longitudinal patient record that is FHIR-native, HL7-compatible, and API-first. Clinical documentation, care coordination, billing, and patient engagement operate from the same data layer, which means a care coordinator looking at a patient record sees clinical history, outstanding quality gaps, care plan status, SDOH flags, and recent transitions in a single view rather than across three systems with three separate logins. The same platform provides a unified care team workbench where clinicians, social workers, care coordinators, and community health workers collaborate directly, with tasks, notes, referrals, and updates shared contextually across roles. The platform monitors referral completion, flags non-compliant transitions, and surfaces at-risk patients to coordinators before readmission windows close, all from the same shared record.
For the IT evaluator and the COO: The integration question that matters is not whether the platform can connect to your EHR; it is whether the integration runs on standard FHIR and HL7 protocols your existing team can support, and whether the unified record translates into a unified workflow that actually changes how care teams work. blueBriX operates as a layered solution on top of Epic, Athena, and Salesforce using open APIs, so the existing EHR investment is preserved. The care team workbench then converts the shared record into the productivity gain that decides whether the program scales at the panel size the contract assumes, or stalls at the staffing budget the organization actually has.
Risk stratification configured for behavioral health-specific signals
Both LEAD and MSSP use a risk-adjusted benchmark to determine shared savings, and the underlying CMS-HCC methodology differs in one critical way: LEAD applies concurrent HCC risk adjustment to its High Needs population segment, updating mid-year as patient acuity shifts, while MSSP relies on prospective HCC throughout. But CMS-HCC sets the benchmark; it does not tell the organization which patients on the panel to engage this week. That is a separate layer of work, and it is where most behavioral health-aligned ACOs lose ground. The stratification logic an organization runs internally to drive its own care management decisions has to surface the right patients before the cost event, not after — and whether that logic works for a behavioral health-heavy panel depends on whether it has been weighted for behavioral health complexity or borrowed wholesale from a chronic-disease primary-care template.
When stratification is borrowed from a primary-care model, the failure mode is silent. The patients flagged for care management are the ones whose HbA1c is creeping up or whose blood pressure has spiked, while the patients whose psychiatric symptom acuity has been trending up for six weeks, whose SUD treatment adherence has just slipped, or whose housing situation just destabilized remain invisible until the ED visit or the readmission has already happened. Care management resources reach the wrong patients on the wrong cadence, and the high-cost utilization the model was supposed to prevent occurs on schedule.
blueBriX’s risk stratification combines EHR, claims, behavioral, and social data into whole-person risk scores rather than single-domain indicators, and the Intelligence engine applies machine-learning models that flag patients likely to experience adverse events within the next 30, 60, or 90 days. The model is configurable to the organization’s specific clinical profile, which matters because a panel with high SMI or SUD volume does not perform the same as a panel of primary-care patients with chronic disease, and the stratification logic should not pretend otherwise.
For the CMO: The patients who drive cost in a behavioral health-heavy panel are not the patients a chronic-disease-weighted model surfaces. Without behavioral health-weighted stratification, the right care management resources reach the wrong patients, and the patients you most need to engage stay invisible until the crisis event has already produced the cost.
Point-of-care quality capture embedded in clinical workflows
Quality scoring directly affects the shared savings calculation under both LEAD and MSSP, but the timing and the measure sets differ enough that the build cannot be deferred. MSSP’s APP Plus quality reporting requirement has been mandatory since PY2025, which means MSSP participants are already obligated to report all required measures and cannot rely on partial coverage. LEAD’s quality measure set is a subset of MSSP’s, aligned to underserved and behavioral health populations, with a phased reporting structure that runs through PY10. In both cases, the measures need to be captured at the point of care, as a byproduct of clinical documentation, not abstracted from clinical notes days or weeks later by quality analysts working under submission pressure.
Retrospective capture systematically underrepresents actual clinical performance. A PHQ-9 administered during the visit but recorded only in a free-text note will not surface in the quality measure pipeline. A C-SSRS conducted verbally without structured documentation will not count toward suicide risk screening compliance even though the clinical work was done. The gap between care actually delivered and care that scores is closed at the point of documentation, not at submission time.
blueBriX embeds quality measure capture directly in clinical encounter workflows, with a library of more than 200 pre-built assessments including PHQ-9, GAD-7, C-SSRS, CAGE, MDQ, and SDOH tools. The platform is built to support CMS and Medicare reporting requirements, with operational, quality, and value-based measures captured as care is delivered, so reporting is complete, traceable, and submission-ready rather than compiled under deadline.
For the Compliance and Quality Lead: Retrospective capture systematically underrepresents actual clinical performance, which means the quality score driving your shared savings calculation understates the care your clinicians are actually delivering. Embedding capture in the encounter workflow is the only way to close the gap between care delivered and care that scores.
Revenue cycle built for hybrid FFS-plus-risk economics
Value-based care does not replace fee-for-service billing; it runs in parallel with it. Under LEAD or MSSP, the same coding gap that costs you a fee-for-service claim also distorts your risk-adjusted benchmark. Denials that look like a billing operations problem are simultaneously inflating the cost baseline you will be measured against. Coding completeness, denial prevention, and support for hybrid billing arrangements are not separate from ACO performance; they are embedded in it.
When the revenue cycle is treated as a back-office function disconnected from clinical documentation, two failures compound. Direct revenue is lost to denials that could have been prevented with cleaner coding at the encounter. And the risk-adjustment data flowing to CMS understates the actual clinical complexity of the panel, which means the benchmark the organization is measured against is lower than it should be, and the shared savings opportunity that should have existed never materializes. For behavioral health-aligned organizations, where unspecified diagnoses and undercoded SDOH factors are common, this gap is structural rather than incidental.
blueBriX’s RCM capabilities support fee-for-service, capitation, per diem, and value-based billing arrangements simultaneously, with automation for prior authorizations, claims processing, and denials management. The platform connects clinical activity, payer rules, billing, and collections so revenue status is visible in real time. Because the RCM and care coordination modules operate from the same unified data layer, the clinical documentation that drives care coordination also feeds billing and coding workflows, rather than requiring separate data entry across disconnected systems.
For the CFO: A platform where clinical documentation, coding, and billing operate from one data layer means the CFO sees revenue cycle performance and benchmark implications in the same view, not in separate reports reconciled at quarter end.
Sequencing the build: what comes first
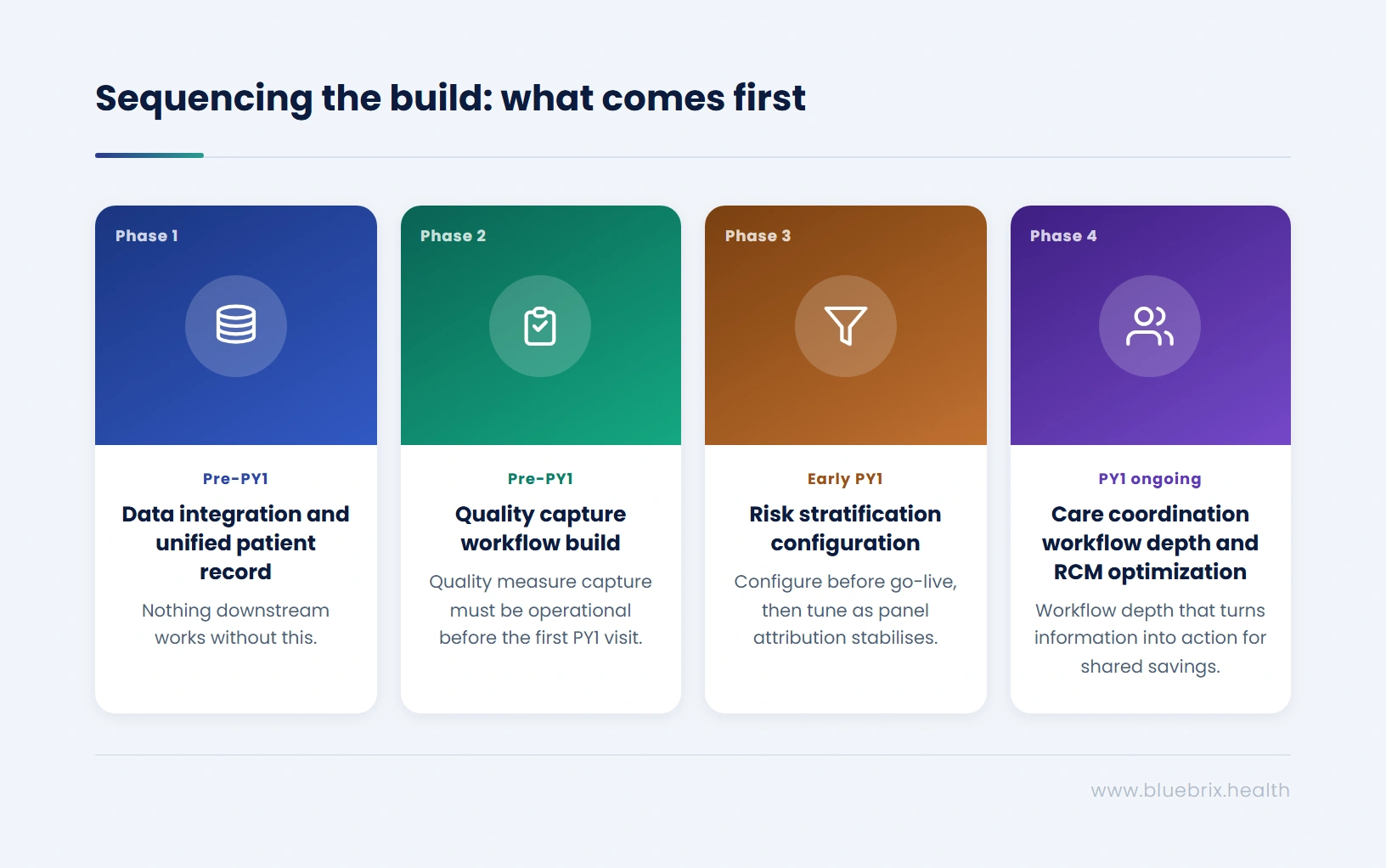
Recognizing the capabilities is the easy part. Sequencing them correctly is what separates organizations that arrive at PY1 ready from organizations that arrive at PY1 still building. Each capability depends on the one before it; skipping the sequence is the single most common reason go-live underperforms.
Phase 1, pre-PY1: Data integration and unified patient record. Nothing downstream works without this. Risk stratification cannot run on partial data, quality capture cannot embed in workflows the platform cannot see, and care coordination cannot close loops it cannot track. This is the longest-lead-time piece of work and the one most worth front-loading. For organizations layering blueBriX on top of an existing EHR, a first VBC workflow with a pre-validated partner agent is typically live within four to eight weeks of contract signature, assuming FHIR-based connectivity and contract-rule configuration are completed upfront.
Phase 2, pre-PY1: Quality capture workflow build. Quality scoring begins the moment the performance period begins. Encounter workflows, assessment libraries, and quality measure capture have to be operational before the first PY1 visit, not configured after it. For MSSP organizations subject to APP Plus, this work is already overdue if it has not started; for LEAD entrants, it is the second-shortest-lead-time piece of work after data integration and should be running in parallel.
Phase 3, early PY1: Risk stratification configuration. Stratification refines as the panel attribution stabilizes in the first quarter of PY1. Configure it before go-live, then tune it as attribution data and the first cycle of utilization data come in. This is iterative work; the goal is a stratification model that is directionally correct on day one and progressively more accurate by the end of the first quarter.
Phase 4, PY1 ongoing: Care coordination workflow depth and RCM optimization. Once data, quality capture, and stratification are in place, the build shifts to the workflow depth that turns information into action: referral tracking, transitions of care, RCM integration, denial prevention, and the closed-loop coordination that converts risk-adjusted benchmarks into shared savings. ACO-readiness benchmarking for a full multi-capability configuration typically runs 60 to 90 days from initiation, layered on top of the Phase 1 foundation. The 4-to-8-week and 60-to-90-day timelines are not competing; they describe different scopes of the same build.
The blueBriX advantage
Three things separate the blueBriX approach from a feature-by-feature comparison with point solutions.
A single data foundation, not point solutions stitched together. Risk stratification, quality capture, care coordination, and RCM all operate from the same unified longitudinal patient record. The clinical documentation that informs a care plan also feeds the quality measure pipeline and the billing workflow, without separate data entry, separate logins, or reconciliation overhead. The compound effect matters more than any individual feature: every capability gets sharper as the others improve, because they are all reading from and writing to the same source of truth.
Configured to the behavioral health-specific clinical profile, not a primary-care model retrofitted. The risk stratification logic, the assessment library, the care coordination programs, and the quality measures are all built for panels where SMI, SUD, and SDOH-driven complexity are the dominant clinical signals, not edge cases at the end of a chronic-disease workflow. That orientation is what makes the difference between surfacing the right at-risk patients and surfacing the patients whose blood pressure is creeping up while the patients in crisis remain invisible.
Designed for the FFS-to-risk transition, not either-or. The RCM module handles fee-for-service, capitation, per diem, and value-based arrangements simultaneously, which matters because most behavioral health organizations entering LEAD or MSSP are not stopping FFS billing; they are running it in parallel for the duration of the transition. Treating the transition as a phased migration rather than a hard cutover is what keeps revenue stable while the value-based contracting matures.
Start the Infrastructure Conversation Before the Performance Clock Does
Whether you’re entering ACO LEAD in 2027, already in MSSP, or still working through the choice in Part 1, the infrastructure work is the same, and the window is narrower than it looks.
Connect with the blueBriX team to walk through where your organization stands and what the build sequence looks like from here. Bring your toughest workflow challenge, the goal is to show you how the platform handles it in practice, not in a slide deck.
Request a demo