Why does your EHR choice matter for FFPSA/QRTP compliance in 2026?
FFPSA/QRTP compliance failures are not edge cases; they are the normal operating cost of running a residential behavioral health program on an EHR that was not built for it. Here is what that cost looks like in practice: a child in QRTP placement for 90 days, with a QI assessment completed on day 33, generates zero Title IV-E reimbursement for the entire stay. Not the four late days. The entire episode. And the clock starts at the date of placement, not the date the program decides to initiate the assessment. That is not a billing error. That is an organizational financial event, and it happens quietly, with no denial, no appeal, and no recovery path.
FFPSA has been law since 2018. For most operators, it arrived as a policy memo and a new column on a spreadsheet. Years of phased implementation allowed organizations to manage new requirements through manual tracking and additional admin headcount. That window has closed. Across multiple states, Medicaid agencies have moved to tighten utilization management requirements for both QRTP and PRTF programs, and where that shift has taken hold, the documentation standard and audit posture have changed with it. The financial exposure for documentation failures is no longer theoretical; it is being realized in recouped federal reimbursements and in placement episodes that become entirely unbillable.
For the Compliance and Quality Owner: the pressure is in the chart. Every 30-day assessment window is a countdown. Every court review is a federal eligibility decision. Every note that does not trace back to a diagnosis, a treatment goal, and an authorized service is audit exposure sitting in the medical record.
For the Econ/Ops Owner: the pressure is in the remittance advice. Missed deadlines do not generate correctable denials. They generate forfeitures.
EHR selection in 2026 is a compliance strategy. The wrong system costs more in lost federal revenue, audit exposure, and clinical staff turnover than any implementation project will. The rest of this article delivers the framework to evaluate the right one.
Why is multi-program architecture the first thing to evaluate in a residential behavioral health EHR?
Most residential behavioral health operators are not running a single program. They are running a portfolio, and that portfolio creates a documentation and billing architecture problem that most EHRs were never designed to solve.
A single organization may simultaneously house title IV-E-funded QRTP residents and Medicaid-funded PRTF residents, MST-enrolled youth, and group home placements, often with the same clinical staff, sometimes with the same young person moving between program types within one episode of care. Each program carries different billing logic, different documentation standards, and different federal eligibility requirements.
Generic EHRs treat a “patient” as a single billing entity. That architecture breaks down when the same young person transitions from PRTF to QRTP, or when an organization is billing per-diem for a PRTF resident while simultaneously tracking QRTP assessment deadlines for a child in the next room. Staff compensate with parallel records, separate spreadsheets, and documentation fragmentation that turns a federal audit into a multi-day paper reconciliation exercise. A purpose-built psychiatric residential EHR solves this at the architecture level, not through workarounds.
The foundational evaluation question: Can a single patient record hold multiple concurrent program enrollments with separate billing logic, separate documentation workflows, and enforced access rules, without workarounds?
PRTF vs. QRTP authorization pathways are structurally different. PRTF requires medical necessity certified by an independent multidisciplinary team and recertified every 30 days. QRTP requires assessed need determined by an independent Qualified Individual using the CANS, on a 60-day court review cycle. An EHR that cannot distinguish these at the workflow level will generate compliance failures at scale.
Program-level access control must be configurable in an admin console, not through vendor tickets. A systematic review of access control solutions in EHR systems (ScienceDirect, 2024) identifies role-based access control as the foundational authorization mechanism for HIPAA compliance and accreditation readiness, because it creates the audit trail that surveyors and regulators require. PRTF staff seeing only PRTF records, MST staff seeing only MST records, with a psychiatrist shared across programs logging in once – this is an explicit requirement under CARF, The Joint Commission, and COA accreditation standards, not a permissions preference.
What are the two FFPSA/QRTP deadlines that carry the most financial risk?
The 30-day assessment cliff
Federal law is unambiguous: if the independent QI assessment is not completed within 30 days of QRTP placement, there is no Title IV-E reimbursement for any portion of that episode. Not the overdue days. The entire episode. This cannot be appealed or remediated after the fact.
The Qualified Individual must be independent, not employed by or affiliated with the residential program. They must be trained and certified to administer a validated functional assessment tool. Their findings must return to the EHR as structured clinical data, not a PDF attachment, so CANS scores flow directly into the treatment plan.
Most organizations track this in spreadsheets. The 30-day window closes before the QI assignment is confirmed. By the time anyone notices, the forfeiture is permanent.
What makes the failure invisible: The assessment deadline does not surface in the billing module. It does not send an alert. It sits in a spreadsheet that someone updates when they remember to, flagged when a supervisor thinks to check it, and missed when the caseworker tracking it is on leave.
The 60-day court review
Within 60 days of QRTP placement, the juvenile court must make three findings: that the child’s needs cannot be met in a foster family home, that the QRTP is the least restrictive appropriate setting, and that the placement is consistent with the permanency goal. These are judicial determinations; the court needs the QI assessment data and treatment plan documentation organized and court-ready.
Texas: Within 10 calendar days of QRTP placement, DFPS must send notice to all legal parties and file a motion requesting a hearing. That hearing must be set within 45 calendar days of initial placement. Any written objection to the QI assessment must reach the court within 7 calendar days of the assessment being submitted. The court has until day 60 to issue its placement ruling. At every subsequent status review and permanency hearing, the court must approve or disapprove continued QRTP placement, with required documentation filed 10 days before each scheduled hearing. (Source: DFPS Court Process for Texas QRTP Pilot Program.)
Minnesota: Court review of QRTP placements requires a specific state form: the Qualified Residential Treatment Program Placement Addendum to the Report to the Court (DHS-8249), filed with the standard Report to Court (DHS-8248). This addendum is a structured documentation requirement — not simply a narrative update — and the data it requires must come from the clinical record in structured form, not assembled manually at the time of filing. (Source: Minnesota DHS Child Foster Care forms directory.)
Michigan: Under MCL 722.123a, the court must approve or disapprove QRTP placement at every dispositional review hearing and every permanency planning hearing for as long as the child remains in placement. There is no time-limited review window after initial approval; the ongoing approval obligation continues through the full placement episode. For children placed in a QRTP for more than 12 consecutive months or 18 nonconsecutive months, MDHHS must additionally obtain signed departmental director approval for continued placement. (Source: Michigan Legislature, MCL 722.123a; Michigan SCAO JJB 2025-002.)
Ohio: The Ohio Supreme Court’s QRTP Toolkit establishes that the level of care assessment must be submitted to the court prior to the hearing and the hearing must be held within 60 days of placement. Ohio recommends that all QRTP hearings be conducted by judicial officers only — not review boards — and that family and permanency team members be permitted to attend. (Source: Ohio Supreme Court Children and Families Commission QRTP Toolkit.)
The goal of deadline management in a residential EHR is not a reminder system. It is a workflow that makes the missed deadline operationally difficult to achieve. Required documentation fields cannot be bypassed. The chart does not advance without what the regulation requires. This is compliance enforcement built into the clinical workflow, not compliance tracking added on top of it.
For compliance and quality leaders: if your current EHR cannot show you a live countdown to the next QI assessment deadline, cannot enforce mandatory documentation fields before a note is saved, and cannot generate a court-ready report from structured data rather than a case manager’s manual assembly – those are audit gaps, not software preferences.
What does QRTP documentation standards actually require from clinical staff?
QRTP standards require that clinical and nursing staff availability be documented in real time against the trauma-informed treatment model being implemented, not batched at the end of a shift. Batch charting is no longer a defensible audit posture, consistent with updated utilisation management standards under CMS Informational Bulletin guidance and the documentation expectations enforced during federal QRTP compliance reviews. Behavioral health providers that have moved to integrated, real-time documentation workflows have reported a 20% reduction in administrative workload and 40% faster patient intakes, as documented in blueBriX’s Laurel Life implementation case study and Blackbird Health case study.
Every note must trace back to a specific diagnosis, a treatment goal, and an authorized service, the “golden thread.” Without mandatory field validation and role-based note form auto-loading, that thread is only as reliable as a night-shift technician’s memory at 11 PM.
Role-based note-form auto-loading, where the correct form appears when the right provider opens a chart, is what makes contemporaneous documentation sustainable at scale without adding burden to every encounter. AHIMA’s Clinical Documentation Integrity guidance establishes that incomplete or inaccurate records directly compromise reimbursement accuracy, quality reporting, and audit outcomes – and that hospitals with strong clinical documentation programmes earn significantly more through reimbursements (Black Book Market Research, 2016). Mandatory field validation that turns the chart into an audit-ready record by construction, not by review, is what operationalises that reduction.
How should a PRTF handle family outreach and guardian consent under FFPSA?
FFPSA mandates regular, documented family outreach, and unsuccessful contact attempts must be documented as thoroughly as successful ones. The burden of proof falls entirely on the agency. The HHS Children’s Bureau has established that meaningful family engagement under FFPSA is a documented, interactive process at every stage of the placement – and that Title IV-E eligibility is tied to the agency’s ability to demonstrate it (ACF Capacity Building Center for States, 2021). Every contact attempt, answered or not, timestamped in the medical record – that is the standard of proof the regulation requires.
Generic patient portals were designed for adult patients managing their own care. For a minor in residential placement, this architecture is wrong by design. The legal guardian, whether a biological parent, foster parent, child welfare agency, or court, is the primary contact for all consent, communication, and signature routing. A patient portal adapted after sale for minors produces a workaround that fails audit because it does not generate the clean signature chain FFPSA requires.
A compliant guardian-first workflow
- Sends digital consent forms to the legal guardian before the family arrives, not as a 40-page packet on admission day
- Routes CFT meeting documentation to all required participants with configurable multi-party signature sequencing
- Captures every outreach attempt, answered or not, timestamped in the medical record
- Notifies guardians automatically on key clinical events
- Supports guardian e-signatures via email, SMS, or portal
Most EHRs will tell you they support FFPSA compliance.
Few can show you a live workflow where the 30-day countdown starts at admission, the guardian receives a consent form before the family walks in, and the court-ready report generates from structured data rather than a case manager’s last-minute assembly. If you are evaluating whether your current platform can actually do this, or trying to understand where the gaps are before an audit surfaces them, that is exactly the conversation blueBriX is built for.
See how it works for your specific program mix.
Can an EHR predict a crisis before it becomes an incident report?
Incident reports are reactive documents; they describe what happened after the event. The mandatory reporting burden for restraint and seclusion, AWOL, elopement, and abuse/neglect is substantial, but it is a lagging indicator. By the time the report is written, the clinical event has occurred.
A 2025 meta-analysis in BMC Medical Informatics found that AI-based early warning models significantly reduced in-hospital and 30-day mortality rates across prospectively validated clinical settings. In psychiatric settings specifically, research published in JMIR Mental Health (2026) introduced a deep-learning model trained on longitudinal psychiatric EMR data that anticipates adverse events in 24-hour windows – catching deterioration before it reaches the incident log. Predictive crisis AI applies this same principle within the residential record. Reading clinical notes to track how a patient’s documented behaviour trends over time is how gradual deterioration is caught before it surfaces in the incident log: a patient described as engaged two weeks ago and described as withdrawn and irritable today has a trajectory in the documentation before it reaches a critical event.
What distinguishes useful predictive AI from generic note-drafting tools is explainability. Every risk score must be traceable: what was documented, when, by whom. Clinical leadership must be able to set thresholds for their specific population, because the risk profile of an acute PRTF census is different from a trauma-focused QRTP program. The AI must be governable after go-live, not locked to vendor release cycles. For a Compliance and Quality Owner, this governance dimension is what transforms a predictive tool from a liability into an accreditation asset: when a surveyor asks how the program identifies deteriorating patients before a critical incident, the answer is a documented, configurable, auditable clinical process – not a black-box algorithm. The AI output is clinically explainable, the decision thresholds are set by the program’s own clinical leadership, and the flag-to-action chain is visible in the medical record.
What does patient engagement look like in a PRTF or QRTP setting?
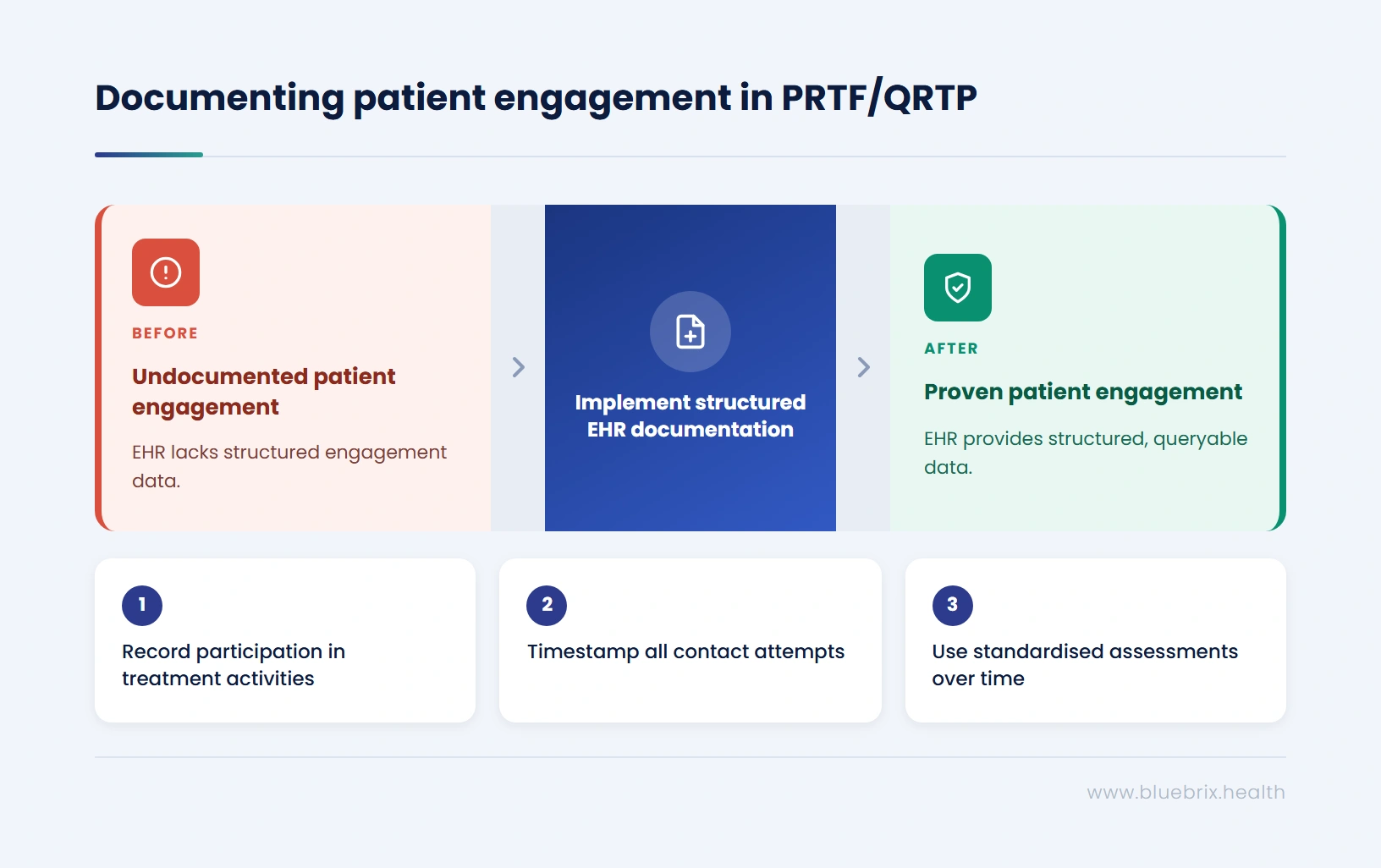
For a Clinical Director, the question is not whether their program engages patients; it is whether the EHR can prove it. For a Documentation and Compliance lead, the engagement record is the evidence that the certified trauma-informed treatment model is being delivered, not just described in a policy document. Both are reading the same chart. Both need the same structured data.
In a PRTF or QRTP, patient engagement is not about appointment reminders or portal logins. It has three dimensions that the EHR must document and produce as structured evidence:
1. In-facility therapeutic engagement: Participation in group therapy, individual sessions, skill-building programming, and other treatment model components must be documented in the chart, not in a separate activity log. Auditors review this to confirm the trauma-informed care model is being delivered, not just described in a policy document. If participation data cannot be queried from the clinical record, it cannot be included in court reports or authorization renewals.
2. Family and guardian engagement: FFPSA requires that every contact attempt with biological family, foster parents, or fictive kin, answered or not, is timestamped and documented in the medical record. The burden of proof is on the agency, not the family. This extends to discharge: connecting the patient and guardian to outpatient services and community supports before the discharge event, documented in the chart, carries direct clinical and financial implications for continued authorization and post-placement outcomes.
3. Treatment response tracking: The American Psychiatric Association’s resource document on Measurement-Based Care establishes that routine use of standardised assessment tools allows both clinician and patient to track symptom burden over time and correlates directly with treatment decisions and care transitions. Longitudinal tracking and visual insights — PHQ-9 trends across 90 days, CAFAS trajectories, CGAS scores at admission versus week 8 — are the clinical argument for continued QRTP placement. An assessor cannot work from a PDF. A judicial officer cannot draw findings from a document folder.
How does residential behavioral health billing differ, and where does revenue get lost?
Per-diem, hold-bed, and capitated billing from the bed log
Residential behavioral health billing does not work like outpatient billing. Per-diem rates bundle room, board, supervision, and clinical services into a single daily rate. Hold-bed billing requires claiming reimbursement for a reserved bed before a patient is assigned. Capitated arrangements require distributing a flat monthly payment across a population without generating individual claims per patient.
An EHR built for outpatient encounter billing forces residential billing teams to manually reconstruct claims from census records every month, a process that introduces errors, delays cash flow, and creates the discrepancies that trigger denials. Purpose-built revenue cycle management for residential programs starts from the bed log, not from manual reconstruction.
Prior authorization expiry: the top preventable revenue loss
A systematic review published in The American Journal of Medicine (2026) found that prior authorization delays are associated with disease exacerbation, preventable hospitalization, and worse patient outcomes, with behavioral health among the specialties where these harms were documented, making prior auth expiry warnings inside the clinical workflow not just a billing safeguard but a clinical one.
The core problem is architectural: prior authorization status lives in the billing module. The treatment plan lives in the EHR. The two do not communicate. The clinician writing the daily note on day 28 of a 30-day authorization has no visibility into expiry. By the time the biller catches it, the stay has extended past the authorization and those days are not recoverable.
The pre-billing scrub
Between claim generation and submission sits the pre-billing scrub: an automated check of every claim against the clinical and administrative record before it leaves the system. Does the bed log match the claim? Is documentation complete? Is the authorization current for this date? Are there code discrepancies? Industry data shows that automated pre-submission claim scrubbing consistently reduces denial rates by 15–25% and pushes first-pass acceptance rates above 95% (Experian Health State of Claims, 2025; business.com RCM benchmarks, 2026).
Claims that fail the scrub surface on the biller’s queue for correction before submission, not as a denial after the fact. Prevention is cheaper than rework at every stage of the revenue cycle.
What reporting does residential leadership actually need day to day?
An operations manager opening their dashboard at 7 AM needs to know which beds are available, which notes from the night shift are incomplete, and whether any authorizations expire this week. A CFO pulling a board report needs average length of stay by payer, denial rates by program, and A/R trends over the last quarter. These are not the same question, and an EHR that conflates them fails both readers.
Operational dashboards: what leadership needs in real time
Operational dashboards answer the question of what is happening right now. They are not reports; they are live views that support intraday decisions. The census that an admissions coordinator uses to place a patient and the census that drives per-diem billing must be the same number, generated from the same source. When dashboards unify scheduling, billing, and documentation into a single live view, the results are measurable: blueBriX’s own client, Laurel Life’s case study recorded a 20% increase in appointment utilisation and a 15% reduction in operational costs after consolidating these workflows. Real-time operational and compliance dashboards built on a single record are what make that consolidation possible.
Real-time operational visibility covers five domains:
- Bed census and utilization: Occupied, on hold, available, by unit, program, and level of care. Same-day discharge and admission events update the map immediately.
- Documentation compliance rates: Percentage of required documentation complete, by program and clinician. What a Director of Clinical Services reviews in morning rounds to identify where follow-up is needed before the day shift ends.
- Financial performance indicators: Clean claim rate, denial rate by payer, authorization utilization, days in A/R by payer class.
- Staffing and incident metrics: Overtime by unit, incident rates by type, restraint and seclusion events with mandatory reporting status.
- Referral pipeline: Active referrals by stage. Where files are stalling at authorization, guardian consent, or clinical review. Average time from referral to admission by payer and program.
Utilization reporting: running the program, not just proving compliance
Utilization reporting is the operational counterpart to compliance reporting. Where compliance reports answer “are we meeting regulatory obligations?” utilization reports answer “are we using capacity effectively and is revenue aligned with cost?”
Key utilization metrics for residential operators: bed occupancy by unit and level of care, average length of stay by program type and payer, authorization utilization rates, days denied versus days overturned on appeal, and concurrent review success rates by payer.
These are not only financial metrics. An unusually short average length of stay in a QRTP program may signal that court reviews are generating placements that are not clinically appropriate. A high denial rate for a specific payer may indicate that medical necessity documentation does not meet that payer’s standard. Organizations that use utilization data to manage their programs, rather than discovering its implications only in an audit finding, sustain both clinical quality and financial performance over time.
Which EHR capabilities are non-negotiable for FFPSA/QRTP operators?
Each capability below represents a category where the wrong EHR produces compliance exposure, revenue loss, or both. Rather than presenting these as abstract requirements, each is paired with what blueBriX specifically does, so your evaluation is grounded in platform behavior, not vendor claims.
| Sl No | Capability | What Failure Looks Like | blueBriX |
|---|---|---|---|
| 1 | Multiple program types on one patient record with separate billing logic | New intake required at every program transition; parallel records; fragmented documentation | Native: PRTF, QRTP, MST, group home, BHUC on one chart; history travels with the patient |
| 2 | Program-level RBAC configurable in admin console | Duplicate accounts; shared credentials; access gaps caught at accreditation survey | Admin console configured by agency staff, no vendor tickets, no development cycle |
| 3 | Configuration-first form and workflow builder | Every state rule change becomes a vendor development ticket and a wait | No-code form builder controlled by agency admin; state-specific templates built internally |
| 4 | HL7/FHIR interoperability for state HIE and Medicaid | QI assessment scores enter as PDF scans; eligibility checks are manual; HIE data does not flow | Standard: CCDA, open API, batch eligibility, EPCS, PDMP at point of prescribing |
| 5 | Automated 30-day and 60-day compliance countdowns with escalating alerts | Spreadsheet tracking; deadline missed when tracking staff is on leave; permanent forfeiture | Countdown begins at admission; 7-day and 2-day escalating alerts; supervisor compliance dashboard |
| 6 | Mandatory field validation preventing incomplete documentation saves | Golden thread breaks at the note level; audit finds incomplete records after the fact | Configurable by program and note type; incomplete documentation cannot be saved |
| 7 | Treatment plan review cycle alerts (7 and 2 days before expiry) | Review cycle missed; authorization gap; unbillable days before anyone notices | Built into clinical task queue and compliance dashboard; linked to authorization status |
| 8 | Prior auth expiry warnings inside the clinical workflow | Clinician writing notes has no auth visibility; lapse compounds before billing catches it | Linked to treatment plan; visible to clinician and supervisor in the clinical record |
| 9 | Per-diem and hold-bed claim auto-generation from bed log | Monthly manual reconstruction from census; errors; unbilled days discovered at month-end | All billing models auto-generate from bed log; billers review, not rebuild |
| 10 | Patient-level rate exception handling without per-claim re-entry | Rate exceptions forgotten or re-entered incorrectly per claim; billing errors compound | Configured once on fee sheet; auto-applied to every subsequent claim |
| 11 | Pre-billing scrub before claim submission | Errors discovered post-denial; rework cycle per claim; revenue delayed and reduced | Every discrepancy surfaced to biller queue before submission; corrections logged with timestamp |
| 12 | Integrated utilization review and authorization management | UR coordinator toggles between payer portal and EHR; handoffs produce errors and delays | Single screen: auth status, payer correspondence, clinical record, denial management all in one place |
Your billing model is losing money your current system cannot recover
For operations and finance leaders: the revenue that goes unrecovered from prior authorization lapses, unbilled hold-bed days, and manual census reconciliation errors is measurable. So is the cost of staying on a system that cannot close those gaps. Book a 30-minute demo built around your billing model and revenue recovery priorities.
What to ask in a demo
The capability checklist is an evaluation tool; use it in a vendor demo, not just as a reading exercise. For each capability, ask the vendor to demonstrate it live, in a scenario that reflects your actual programs. Do not accept slides or described workflows as answers to these questions.
Specific signals to watch for: If a vendor says their system “supports FFPSA compliance” but cannot show you an automated countdown timer that begins at admission, that is a compliance tracking claim, not a compliance enforcement claim. If a vendor says they handle multi-program access control but the demonstration requires toggling between user accounts, the architecture is not what they described. If per-diem billing requires a manual step to generate from the census, the bed log and the billing module are not connected.
Implementation: 60-90 days to go-live
Once a vendor has demonstrated all 12 capabilities against your real programs, the next question is straightforward: what does switching actually look like, and what is the cutover risk? The most common reason residential operators defer EHR replacement is not cost; it is the prospect of a disruptive transition during a compliance-intensive period. The answer to that concern is structured sequencing and embedded support, not a delayed decision.
blueBriX follows a structured 12-week implementation in three phases. Over 12 weeks, blueBriX moves agencies from discovery and workflow mapping to no-code configuration, then into parallel training, selective data migration, integration, testing, go-live, and stabilization. The process is designed to keep staff productive, preserve clinical continuity, and avoid custom development cycles.
Module sequencing is decided with the agency’s team based on operational priorities. The 60-to-90-day timeline is confirmed before contract signature, not estimated afterward. For operators concerned about census continuity during the transition window, blueBriX addresses this directly through three built-in safeguards: dual-system parallel operation during the active migration period, so no clinical record exists only in the outgoing system; a historical data archive with full search access post-go-live, so prior placement documentation remains available to clinical and compliance staff; and an active record migration protocol that prioritises current residents in the first migration wave, so the records staff use daily are live in blueBriX before legacy system access is reduced.