The bill arrives after the contract is signed
Organizations typically spend $31,710 more per year on their EHR than originally budgeted[1]. That figure represents observed variance in healthcare IT project costs — the gap between what organizations plan for and what they actually spend. It does not represent negligence or unusual complexity. It represents what happens when an EHR budget is built around a vendor quote rather than a total cost of ownership model.
The vendor quote covers the subscription fee. It rarely covers the full scope of implementation, data migration, training, workflow redesign, third-party integrations, compliance configuration, ongoing maintenance escalations, and the productivity revenue lost during go-live. For behavioral health organizations, add 42 CFR Part 2 consent management infrastructure, CCBHC documentation requirements, and USCDI v3 interoperability compliance — none of which a general-purpose EHR vendor will surface in a sales conversation.
Total Cost of Ownership (TCO) in an EHR system is the full lifecycle cost of owning and operating the platform — every dollar spent from contract signing through year ten, not just the line items on the vendor invoice. EHR implementation costs vary significantly by organization size, deployment model, and scope. Industry analyses consistently show that planning, personnel, configuration, and data migration costs dwarf the software license fee — and that first-year total spend routinely exceeds initial vendor estimates. The most reliable way to understand your organization’s exposure is to require vendors to produce a full five-year TCO proposal before contract signing, not a subscription quote.
blueBriX behavioral health EHR and AI orchestration platform is built for the organizations most affected by the problem this article addresses: behavioral health providers, CCBHC-certified programs, psychiatric residential treatment facilities, and value-based care organizations whose cost structures are more complex than the average EHR sales process accounts for.
This article breaks down every component of EHR TCO, identifies where behavioral health organizations are most frequently surprised, explains how pricing model design determines long-term cost, and explains how blueBriX approaches pricing to remove financial uncertainty from a decision organizations live with for a decade.
What does EHR total cost of ownership actually include?
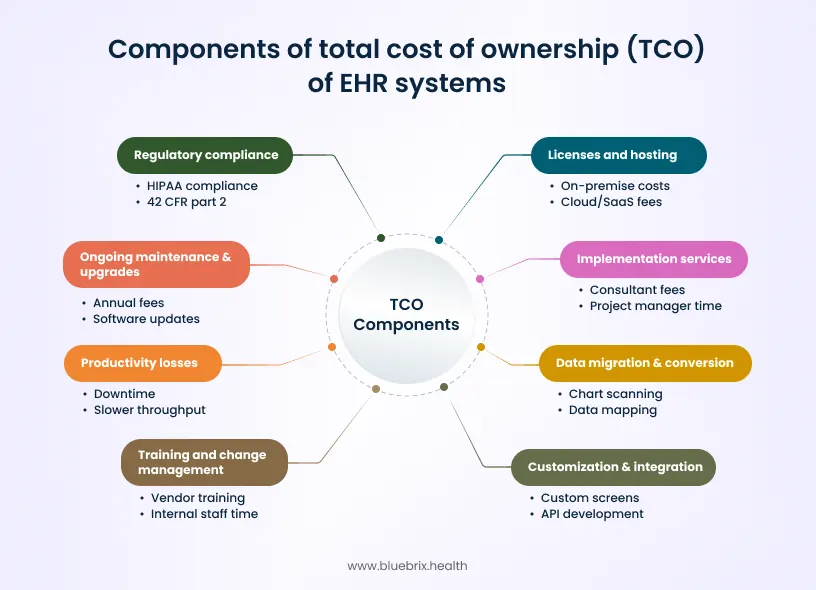
Most EHR cost conversations start and end with the subscription fee. The more accurate model breaks TCO into six categories, four of which do not appear on a standard vendor proposal.
1. Licensing and hosting
Cloud-based EHR subscriptions typically run $200–$700 per provider per month[3] for software alone, with monthly costs scaling higher for larger organizations depending on user count and functionality. On-premise deployments add server infrastructure, network equipment, power, and dedicated IT staff — costs that cloud models bundle into the subscription but offset with higher ongoing fees.
The hosting decision shapes five-year cost in ways that are not obvious at the point of purchase. Cloud EHRs carry lower upfront exposure but higher long-term subscription accumulation. On-premise systems carry higher capital cost but lower recurring fees. The right choice depends on the organization’s cash position, IT staffing model, and how long it intends to hold the platform.
2. Implementation services
Implementation is where most EHR projects first encounter unexpected pressure — and where most fall short. According to KLAS Research’s EHR implementations 2025 report[4], only 38% of organizations say their recent EHR implementation hit the mark, with 40% of healthcare leaders reporting significant misses and a further 22% reporting average results with room for improvement. Crucially, 75% of organizations that experience a poor implementation continue to report low EHR satisfaction two or more years later — meaning implementation failure is not a short-term disruption but a long-term operational drag. The costs behind those misses — scope overruns, remedial training, productivity losses, and workflow fixes — are real financial consequences that never appear on the original vendor quote.
Implementation is not a fixed cost. It scales with scope, and scope has a way of expanding. Every additional integration, every custom workflow template, every site added to the rollout adds time and budget. The organizations that manage implementation cost most effectively freeze scope at contract signing and budget for phased additions rather than configuring everything in year one.
3. Data migration and conversion
Moving existing records — from a legacy EHR, paper charts, or a combination — into a new system is one of the most consistently underestimated costs in an EHR project. A peer-reviewed systematic review of EHR-to-EHR transitions published in the Journal of General Internal Medicine[5] identifies data migration as one of the most complex and risk-prone phases of any EHR transition, with no two organizations reporting identical approaches or outcomes. Costs vary significantly depending on record volume, legacy data format, and how much historical data must be actively migrated versus archived.
For behavioral health organizations, data migration carries additional complexity. 42 CFR Part 2-protected substance use disorder records must be handled separately from general clinical data, requiring segmentation that a migration vendor unfamiliar with behavioral health compliance may not anticipate.
4. Training and change management
Training and change management is consistently the most underinvested element of EHR implementation. According to KLAS Arch Collaborative data[6] drawn from over 40,000 clinicians, physicians are 3.5 times more likely to report a poor EHR experience without adequate training. The same data shows clinicians who receive 11 or more hours of onboarding training report the highest long-term EHR satisfaction, with a minimum effective threshold of 3–5 hours — yet the majority of organizations fall short of this. A separate KLAS finding shows that 57% of clinicians report their organization and IT department did not support the implementation well, with gaps in workflow-specific training cited as the primary reason. The cost of remedial training, help desk volume, documentation errors, and prolonged productivity loss that follow undertrained implementations consistently exceeds the cost of training done properly from the outset[7].
The cost of remediating a training failure — through help desk volume, documentation errors, prolonged productivity dip, and workflow fixes — consistently exceeds the cost of investing in training properly from the outset. Organizations that treat training as a line item to minimize, rather than a risk to manage, pay for that decision twice.
5. Productivity loss
This is the cost category that most frequently surprises organizations because it does not appear on any invoice. EHR Source’s 2026 analysis[8] cites approximately 8% drops in RVUs and visits per physician FTE in the first six months following go-live, with recovery typically occurring by twelve months.
The revenue impact is not abstract, and it scales directly with practice size. Applying that same 8% productivity decline (EHR Source, 2026) to a ten-provider behavioral health practice billing $3 million annually: an 8% reduction in revenue-generating throughput, sustained across the six-month adjustment period, is calculated as $3,000,000 × 8% × (6/12) = $120,000 in foregone revenue — before any direct implementation costs are counted. This is illustrative math applying the EHR source productivity-decline figure cited above to a representative practice size; it is not an independently sourced statistic, and actual impact will vary by organization. The exercise is still worth doing for every EHR budget: take that published productivity-decline rate, apply it to your own annual revenue, and treat the result as a real line item, not a rounding error.
Best practice is to reserve 5–10% of the total implementation budget to manage operational downtime.
6. Ongoing maintenance, upgrades, and compliance
After go-live, annual maintenance or subscription fees recur — commonly 15–25% of the initial license cost for on-premise deployments. Cloud models typically bundle routine upgrades, but organizations should budget separately for retraining on major version changes, updating third-party integrations with each EHR release, and the compliance configuration work triggered by regulatory changes.
Technology and IT expenses typically consume 2–3% of revenue for outpatient medical groups, and these costs are growing year over year. For behavioral health organizations, compliance-driven configuration costs are higher and more frequent than for general medical practices — for reasons addressed in the next section.
Why behavioral health organizations face a wider TCO gap
The TCO categories above apply to any EHR implementation. Behavioral health organizations face three additional cost drivers specific to their regulatory and operational context — ones a general EHR vendor is unlikely to raise in a sales conversation.
42 CFR Part 2 compliance: now in effect
The 42 CFR Part 2 final rule[9] published February 16, 2024 and effective February 16, 2026 is the most significant change to substance use disorder record confidentiality in over 50 years. The rule aligns Part 2 with HIPAA by enabling a single consent for treatment, payment, and health care operations disclosures; applying HIPAA breach notification requirements to SUD records; and shifting enforcement authority to the HHS Office for Civil Rights.
For EHR cost planning, the implications are direct. Organizations must now support granular consent tracking, comprehensive audit logging of every Part 2 disclosure, data segmentation that isolates SUD records from general PHI, and breach notification workflows. EHR source estimates implementation costs for a standalone SUD program at $15,000–$50,000[10] for policy development, staff training, template creation, and technical implementation. EHR configuration costs on top of that vary by vendor: some include Part 2 compliance features in the base subscription; others price them as add-on modules.
What this means for EHR selection
Ask every vendor specifically whether 42 CFR Part 2 consent management, data segmentation, and audit logging are included in the base subscription or priced as add-on modules. An EHR that cannot support these requirements natively will require custom configuration or a third-party compliance layer — both of which increase TCO. Organizations currently operating out of compliance are subject to OCR enforcement as of February 16, 2026.
USCDI v3 and ONC HTI-1: the interoperability cost floor
The ONC Health Data, Technology, and Interoperability (HTI-1) final rule established USCDI v3 as the mandatory interoperability baseline, effective January 1, 2026[11]. Any EHR seeking ONC certification in 2026 must support USCDI v3 data elements. For behavioral health organizations using platforms that have not completed this update, a compliance timeline and potential reconfiguration cost follow.
EHR platforms that require significant custom development to meet USCDI v3 standards will pass those costs through to clients as upgrade fees, add-on modules, or scope-creep items in the implementation statement of work. Configuration-first platforms that handle regulatory changes through their core architecture absorb these costs more efficiently.
CCBHC and program expansion: the cost-of-scale problem
Certified Community Behavioral Health Clinics are subject to eight required service types, state-specific reporting requirements, and federal prospective payment system documentation standards[12]. Adding a CCBHC program is not an administrative change — it is a clinical, operational, and compliance transformation that the EHR must support.
Under module-based EHR pricing, adding a CCBHC program often triggers re-licensing for documentation templates, reporting modules, or care coordination tools not included in the base subscription. Under a platform model where program expansion does not automatically increase licensing cost, the organization pays only for the additional users the program requires — not for the clinical complexity it introduces.
What are the most common EHR budget mistakes behavioral health organizations make?
Treating EHR as an IT project
When EHR selection and implementation is owned entirely by IT leadership without active involvement from clinical, finance, and compliance stakeholders, scope is consistently underestimated. Clinical staff identify workflow needs during implementation rather than before it. Finance teams discover billing integration requirements after contract signing. Compliance officers identify regulatory gaps during go-live rather than during vendor evaluation. Each late discovery adds cost.
Building the budget on year-one figures
An EHR is a 7–10 year commitment. A budget built on year-one cost does not capture year-four subscription escalations, the retraining cost of a major version upgrade in year three, or the integration rebuild triggered by a payer system change in year six. A 5% annual maintenance fee escalation compounds to a significant dollar figure over a decade. Organizations that model 5–10 year cost scenarios before signing are those not renegotiating or replacing under financial pressure.
No contingency reserve
Every EHR implementation encounters unexpected scope. An integration that was not scoped. A data format that was not anticipated. A state reporting requirement that emerged after contract signing. Best practice is to reserve 5–10% of the total implementation budget as a contingency. Organizations that do not build this reserve fund surprises by cutting training, deferring integrations, or extending timelines — all of which increase total cost.
Underfunding training
Only 38% of healthcare leaders consider their EHR implementations successful, according to KLAS 2025 data cited by EHR Source. The same report found that 57% of clinicians say their organization and IT department did not support the implementation well, with gaps in training and change management cited as the primary driver. Undertrained staff produce documentation errors, generate help desk volume, work slower than their pre-EHR baseline for longer, and create conditions for compliance gaps. The cost of remediating a training failure is consistently higher than the cost of training done properly from the start.
Ignoring vendor escalation clauses
Annual maintenance fee escalation clauses are often expressed as percentages that look modest in year one and compound significantly by year five. Negotiate caps. Require fixed-rate or inflation-indexed multi-year agreements. This is one of the most controllable TCO variables in an EHR contract.
How do transparent pricing and modular architecture reduce EHR financial risk?
Pricing transparency
Transparent pricing means that every anticipated charge — software, implementation, data migration, training, integrations, support, hosting, compliance configuration, upgrades — is disclosed line-by-line before contract signing. It means that usage thresholds (encounters, API calls, data storage, e-prescriptions etc.) are defined contractually, so the cost impact of growth can be modeled before it happens rather than invoiced after.
The practical test: ask every vendor to provide a detailed TCO proposal — not just a subscription quote — covering a five-year scenario for your organization’s projected size and usage. Vendors whose pricing model cannot produce this document are the vendors whose pricing will produce surprises.
Configuration-first architecture
Custom code is expensive. It requires paid engineering effort, introduces technical debt, creates long-term vendor dependency, and must be rebuilt — at cost — when the platform updates. Configuration-first platforms built around low-code configuration engines allow organizations to adapt workflows, templates, and forms to their needs without triggering engineering work.
In TCO terms, this is one of the most significant cost stabilizers available. Organizations on configuration-first platforms can onboard new programs, modify workflows, and respond to regulatory changes through configuration rather than development. This difference compounds over a five-year ownership period.
What to negotiate in an EHR contract
- Full TCO disclosure: Require vendors to disclose all anticipated charges — software, implementation, data migration, integrations, training, support, hosting, compliance, upgrade policies, and escalation clauses — before signing. Escalation caps: Fix or cap annual price increases. A specific percentage cap or inflation-indexed adjustment prevents open-ended market-rate escalations.
- Usage threshold documentation: Ensure encounter limits, API call thresholds, storage caps, and e-prescription volumes are documented contractually.
- Service level guarantees: Uptime and performance SLAs with defined penalties for breaches protect against the revenue impact of downtime.
- Data portability clause: Guarantee export of patient data in standard formats without prohibitive fees. This preserves leverage and flexibility for the future.
- Phased implementation scope: Define phases and budget separately. Scope changes that arise after signing should go through a formal change order process.
How blueBriX approaches EHR pricing to reduce TCO risk
blueBriX prices with one governing principle: make cost predictable as organizations scale, without penalizing complexity.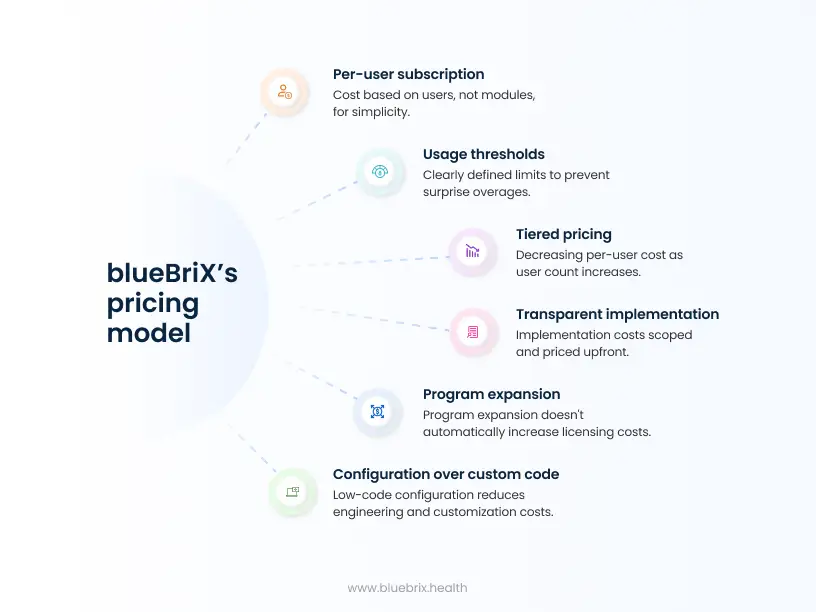
Per-user pricing, not per-module confusion
blueBriX pricing is per user, per month. A user is anyone with system access — clinicians, care coordinators, administrative staff. This aligns cost directly with actual operational footprint.
Core EHR functionality, practice management, scheduling, billing, telehealth, and the patient portal are included in the per-user per-month price. Organizations are not re-licensed when they add programs or care models. This eliminates one of the most common EHR cost traps: paying multiple times for the same capability under different module names.
Usage thresholds defined upfront
Each user license comes with clearly defined usage limits — encounters, API calls, e-prescriptions, and data storage. These thresholds are disclosed early and documented contractually. There are no surprise overage invoices. Finance and operations teams can forecast spend accurately. When usage increases, pricing scales linearly and predictably.
Tiered pricing that rewards scale
Per-user cost decreases as user count increases. This matters specifically for multi-program behavioral health organizations, community agencies expanding services, and value-based care organizations adding care teams. Growth reduces marginal cost instead of inflating it.
Implementation scoped transparently
Implementation, data migration, training, and configuration are scoped upfront, priced transparently on a time-and-materials basis, and documented in the statement of work. This ensures accountability for delivery, clear budget visibility, and the flexibility to phase work based on budget and readiness.
Configuration over custom code
blueBriX is built around low-code configuration engines. Most workflow adaptations, template modifications, and program additions do not require paid engineering effort. Over a five-year ownership period, the absence of recurring custom development costs is one of the most consequential TCO differences between this approach and legacy EHR models.
Program expansion does not automatically increase licensing cost
Adding a new program, service line, or care model — including a CCBHC program, a psychiatric residential track, or a value-based care population health workflow — does not automatically increase licensing cost. Cost increases when user count or usage meaningfully increases. Organizations can grow horizontally without renegotiating contracts every year.
How that changes the five-year cost picture
The structural drivers of cost escalation in traditional EHR models — add-on module sprawl, custom development dependency, opaque overage thresholds, and re-licensing on program expansion — are removed from the equation. These drivers compound precisely where most organizations are least prepared to manage them: KLAS Research found that only 38% of organizations consider their EHR implementation successful, and 75% of organizations with a poor implementation continue to report low EHR satisfaction two or more years later. Every add-on module, every custom integration, and every re-licensing event triggered by program expansion is another point at which that initial implementation experience can degrade further. A pricing model that controls what happens after year one — through predictable tiers, configuration-first design, and transparent contract terms — is where the five-year cost difference is made.