Mid-size behavioral health practices are reconsidering their billing model because the numbers are not adding up anymore. Staffing costs are up. Payer complexity is up. Reimbursement rates are flat. And the in-house billing model that worked five years ago is quietly bleeding margin in ways that do not always show up on a single line in the P&L. 90% of medical groups report that operating costs in 2025 are higher than at the same point in 2024, according to MGMA, and billing overhead is a significant part of that pressure.
This article is for practice administrators and finance leads who want to make this decision. First, you need to understand what is driving this conversation across the industry and why the default answer of “we handle billing in-house” deserves more scrutiny than most practices give it.
- Billing staff costs have risen sharply. An experienced behavioral health biller in most US markets now earns between $45,000 and $62,000 in base salary[1]. Add benefits, payroll taxes, and paid time off and the fully loaded cost sits closer to $58,000 to $78,000 per year per biller. For a mid-size practice running two or three billing staff, that is a significant fixed cost line before you account for software, training, or the productivity lost during turnover.
- Most practices that have not seriously evaluated RCM outsourcing are not avoiding it because they ran the numbers and decided against it. They are avoiding it because no one has run the numbers at all. “We handle billing in-house” is an operational habit. It made reasonable sense when billing complexity was lower, when staff costs were more predictable, and when the gap between in-house and outsourced performance was smaller. In 2026, none of those conditions are as favorable as they once were.
The practices making the sharpest financial decisions right now are treating this as a straightforward business question: what does it cost us to run billing in-house, what would outsourcing cost, and which model produces better net revenue at our claim volume? That question has a calculable answer. The goal of this article is to help you find it for your specific practice.
Before you can do that, you need an honest picture of what in-house billing is actually costing you. That is where most practices have the biggest blind spot, and it is where we start.
The real cost of in-house medical billing (most practices undercount it)
Most practice administrators have a number in their head for what billing costs. It is usually the salary line for their billing staff. Sometimes it includes software. Rarely does it include everything else. The result is that most mid-size behavioral health practices are significantly underestimating what their in-house RCM function actually costs them per year, and that underestimation is distorting the entire in-house vs outsource comparison.
Before you can run a meaningful break-even calculation, you need an accurate cost baseline. Here is how to build one.
Direct costs: salaries, benefits, and training
Start with your billing staff. For each biller, calculate the fully loaded cost, not just base salary. A mid-size behavioral health practice typically runs one to three dedicated billing staff depending on claim volume. At current market rates, here is what that looks like fully loaded:
| Cost component | Per biller estimate |
|---|---|
| Base salary | $45,000 to $62,000 |
| Benefits and payroll taxes (approx. 25 to 30%) | $11,250 to $18,600 |
| Paid time off (15 to 20 days) | $2,600 to $4,800 |
| Annual training and certification | $800 to $2,000 |
| Total fully loaded cost per biller | $59,650 to $87,400 |
Base salary range reflects the BLS-reported May 2024 median wage of $50,250 for medical records specialists, with the range extending to reflect geographic and experience variation. U.S. Bureau of Labor Statistics, Occupational Outlook Handbook (2025). Benefits and payroll tax load reflects standard IRS employer contribution rates and typical benefits packages. Training cost estimate based on AAPC certification program pricing and continuing education requirements. Recruitment cost ($8,000–$15,000) represents direct hiring costs only.
For a practice with two billers, that is $119,000 to $175,000 in direct staffing cost annually. This is the number most practices are not using when they compare in-house to outsourced billing. They are using the salary line, which is materially lower and produces a false comparison.
Also factor in recruitment cost. When a biller leaves, the average cost to recruit, hire, and onboard a replacement in a specialized role runs between $8,000 and $15,000. If your billing team has turned over once in the last two years, that cost belongs in your baseline.
Indirect costs: software, compliance overhead, and staff turnover
Beyond staffing, in-house billing carries a set of indirect costs that are real but rarely aggregated into a single number.
- Practice management and billing software. Most mid-size practices pay between $12,000 and $35,000 annually for their PM or EHR billing module, depending on the platform and claim volume. If your billing staff uses a clearinghouse separately, add another $3,000 to $8,000 per year.
- Compliance and credentialing overhead. Behavioral health billing carries specific compliance demands. Payer credentialing, prior authorization management, and documentation audits all consume staff time. If your biller spends even five hours per week on compliance-adjacent tasks, that is 260 hours per year of billing capacity being used on non-billing work. At a $30 per hour effective rate, that is $7,800 in diverted labor annually per staff member.
- Turnover cost and productivity loss. This is the cost most practices never quantify. When a biller leaves, claims do not stop coming in. The backlog builds, denial follow-up slows, and collections lag. A conservative estimate for the revenue impact of a two to three month billing disruption at a mid-size practice runs between $18,000 and $40,000 in delayed or lost collections, depending on claim volume and payer mix.
The productivity gap no one puts in the spreadsheet
Here is the number that almost never appears in an in-house cost analysis: the revenue your billing function is not collecting because of preventable denials and slow follow-up.
Industry benchmarks for behavioral health billing put the average denial rate between 10% and 15% for in-house teams without dedicated denial management workflows. A well-run outsourced RCM operation typically targets a denial rate below 5%, with top-performing behavioral health billing vendors reporting first-pass denial rates in the 4% to 7% range. For a practice collecting $3 million annually, closing even half that gap represents $90,000 to $180,000 in additional recoverable revenue per year[2].
This is not a guaranteed number. It depends on your current denial rate, your payer mix, and the quality of your clinical documentation. But it belongs in the conversation. When practices compare in-house to outsourced billing purely on cost, they are looking at one side of the ledger. The revenue side, specifically what better billing performance would recover, is equally important to the decision.
Add it up: direct staffing costs, indirect overhead, and the productivity gap. For most mid-size behavioral health practices, the true annual cost of in-house billing lands between $180,000 and $280,000 when all three categories are counted honestly. That is the number you need to take into the break-even framework.
What RCM outsourcing actually costs for a mid-size behavioral health practice
Understanding what outsourcing costs is not straightforward. Vendors quote different pricing models, include different services, and are not always transparent about what falls outside the base contract. Before you can compare outsourcing against your in-house cost baseline, you need to know what you are actually buying and what it will realistically cost at your claim volume and payer mix. Most RCM vendors use one of two pricing structures.
- Percentage of collections is the most common model. The vendor charges a percentage of what they actually collect on your behalf. For behavioral health practices, this typically runs between 4% and 8% of net collections, depending on claim volume, specialty complexity, and the scope of services included. A practice collecting $3 million annually would pay between $120,000 and $240,000 per year under this model.
- Flat fee per claim is less common but worth understanding. Some vendors charge a fixed amount per claim submitted, typically between $3 and $8 per claim for behavioral health. For a practice submitting 2,500 claims per month, that is $7,500 to $20,000 monthly, or $90,000 to $240,000 annually. This model gives you more predictable monthly costs but removes the performance incentive that makes the percentage model attractive.
A small number of vendors offer hybrid models combining a lower base percentage with per-claim fees for specific service categories. These require careful review before signing.
The break-even framework: how to run the numbers for your practice
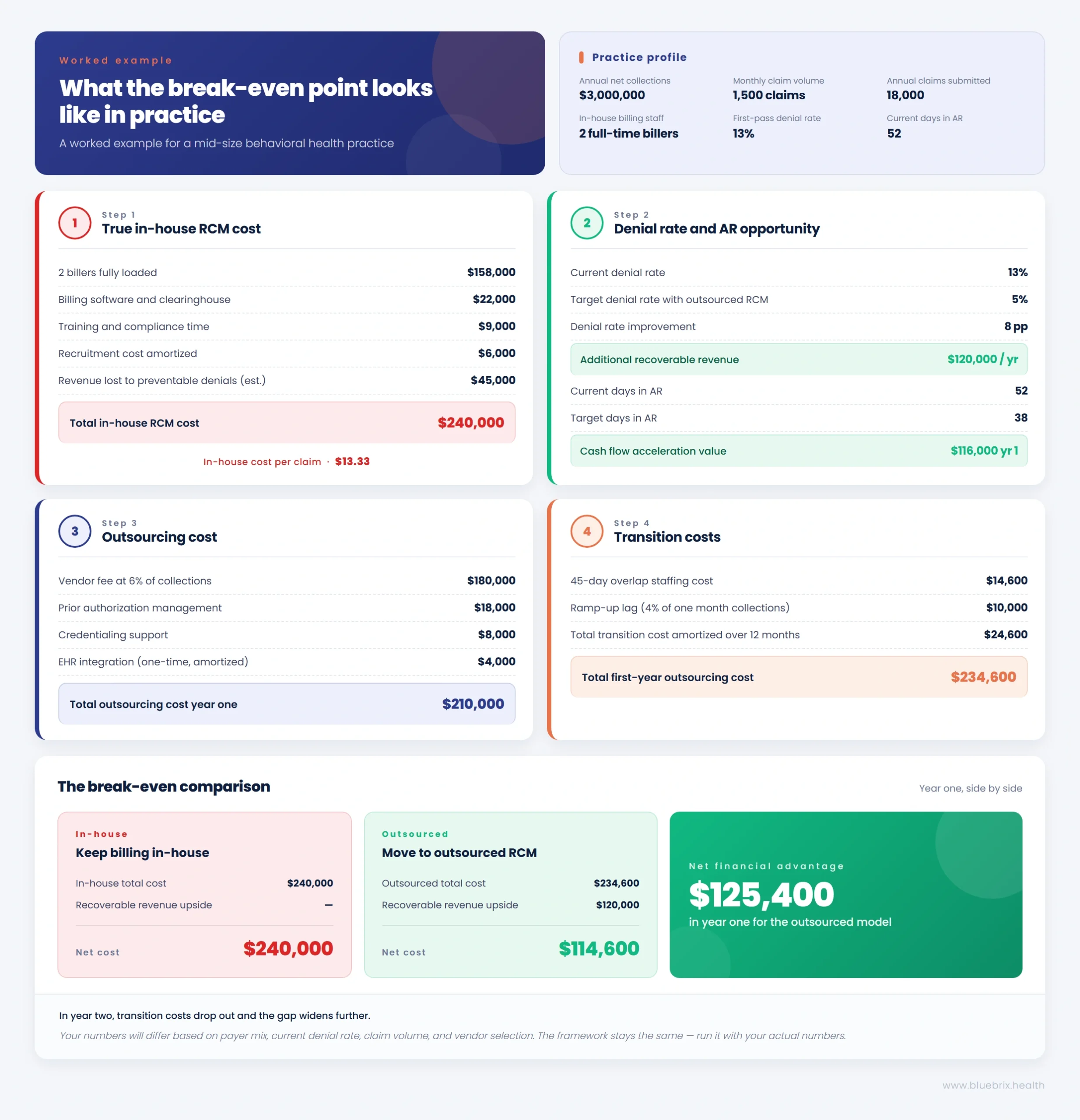
This section gives you a step-by-step calculation to determine whether outsourcing RCM makes financial sense for your practice. Work through each step with your actual numbers. The example scenario at the end shows you what the completed calculation looks like for a representative mid-size behavioral health practice.
Step 1: Calculate your true in-house RCM cost per claim
Start with your total annual in-house billing cost. Use the cost categories from Section 2 as your checklist.
Build your annual in-house cost total:
| Cost category | Your number |
|---|---|
| Fully loaded billing staff cost (all billers) | $ |
| Practice management or billing software | $ |
| Clearinghouse fees | $ |
| Recruitment and onboarding (amortized annually) | $ |
| Training and certification | $ |
| Compliance and credentialing staff time | $ |
| Estimated revenue lost to preventable denials | $ |
| Total annual in-house RCM cost | $ |
Enter your practice’s actual figures in the ‘Your number’ column. Do not use benchmark ranges as substitutes for your own data in a real break-even calculation.
Once you have your total, divide it by your annual claim volume to get your cost per claim.
Formula:
Total annual in-house RCM cost / Total claims submitted annually = In-house cost per claim
Example: A practice with $210,000 in total in-house RCM costs submitting 18,000 claims per year has an in-house cost per claim of $11.67.
This number matters because it gives you a unit economics baseline to compare directly against what an outsourced vendor would charge per claim at your volume.
Step 2: Benchmark your denial rate and collection lag
Your denial rate and days in accounts receivable (AR) are the two performance indicators that most directly affect net revenue. Before you can evaluate whether outsourcing would improve your financial position, you need to know where you currently stand.
Denial rate: Pull your denial data from your practice management system for the last 12 months. Calculate the percentage of claims denied on first submission.
Claims denied on first submission / Total claims submitted = First-pass denial rate
Behavioral health industry benchmark for in-house billing: 10% to 15% Target for a well-run outsourced RCM operation: 4% to 7%
If your denial rate is above 10%, you have a measurable revenue recovery opportunity that belongs in your break-even calculation.
Days in AR: Calculate your average days in AR over the last 12 months.
(Total AR balance / Average daily charges) = Days in AR
Behavioral health benchmark for in-house billing: 45 to 65 days[3]
Target for outsourced RCM: 30 to 45 days[4]
Every day you reduce your AR cycle translates directly into faster cash flow. For a practice with $250,000 in monthly charges, reducing days in AR by 15 days frees up approximately $125,000 in accelerated collections over the course of a year.
Why this step matters: Most break-even analyses only compare costs. This step forces you to also quantify the revenue upside of better billing performance. That upside is often larger than the cost difference between in-house and outsourced models.
Step 3: Model the outsourcing cost at your current claim volume
Now calculate what outsourcing would cost your practice using the pricing models from Section 3.
Percentage of collections model:
Annual net collections x Vendor percentage = Annual outsourcing cost
Example: $3,000,000 x 6% = $180,000 per year
Flat fee per claim model:
Monthly claims x Fee per claim x 12 = Annual outsourcing cost
Example: 1,500 claims per month x $6 per claim x 12 = $108,000 per year
Important: Add any services not included in the base contract. For behavioral health practices, prior authorization management and credentialing support are typically essential add-ons. Get a fully scoped quote from any vendor you are seriously evaluating and use that number, not the headline rate.
Build your total outsourcing cost estimate:
| Cost component | Estimated annual cost |
|---|---|
| Base vendor fee (percentage or per claim) | $ |
| Base vendor fee (percentage or per claim) | $ |
| Prior authorization management | $ |
| Credentialing support | $ |
| EHR or PM integration fees | $ |
| Patient billing and collections (if applicable) | $ |
| Total annual outsourcing cost | $ |
Always obtain a fully scoped quote from any vendor you are seriously evaluating and use the actual figure, not the benchmark range, in your calculation.
Step 4: Factor in transition costs and ramp-up time
Switching from in-house to outsourced billing is not cost-free. There is a transition period that carries its own financial impact and it needs to be part of your calculation.
One-time transition costs to account for:
Overlap period staffing. Most practices run their in-house team in parallel with the new vendor for 30 to 60 days during transition. If you are keeping existing staff through the transition before reducing headcount, calculate the overlap cost.
Monthly in-house staffing cost x Overlap months = Overlap cost
System integration and setup. Depending on your EHR and PM system, vendor integration can carry a one-time fee ranging from $2,000 to $10,000. Confirm this with your vendor upfront.
Ramp-up period performance lag. In the first 60 to 90 days of an outsourced arrangement, collection performance may dip slightly as the vendor learns your payer mix and documentation patterns. A conservative estimate for this lag is 3% to 5% of one month’s normal collections.
One month’s net collections x 4% = Estimated ramp-up lag cost
Amortize transition costs over 12 months to include them fairly in your first-year break-even calculation.
Total one-time transition costs / 12 = Monthly transition cost addition
Add this to your monthly outsourcing cost for the first year only. In year two, it drops out of the calculation entirely.
Note: All figures in this example are illustrative and based on industry benchmark ranges cited in this article. They do not represent actual client data or a guarantee of outcomes. Individual practice results will vary.
When in-house medical billing still makes sense (and when it does not)
Outsourcing RCM is not the right answer for every practice. There are specific conditions under which keeping billing in-house is the more defensible financial decision. There are also clear signals that your current model is underperforming and that outsourcing will produce better results. Here is how to read both sides honestly.
In-house medical billing still makes sense when:
- Your claim volume is low enough that one experienced biller can manage it without capacity strain, typically under 800 claims per month
- Your payer mix is simple, concentrated in one or two payers with straightforward billing requirements
- Your current denial rate is consistently below 5% and your days in AR sit under 35
- You have a long-tenured billing team with deep knowledge of your specific payer mix and no near-term turnover risk
- Your collections performance has been stable and your cost per claim is already competitive with outsourced pricing at your volume
Outsourcing will likely outperform your current model when:
- Your first-pass denial rate is above 10% and has not improved despite internal efforts
- Your days in AR consistently exceed 50 and cash flow unpredictability is affecting operations
- You have experienced billing staff turnover more than once in the last two years
- Your practice is growing and claim volume is outpacing your current team’s capacity
- Your billing staff is spending significant time on prior authorizations and credentialing instead of claims
- You cannot clearly state what your fully loaded in-house billing cost per claim is today
If you cannot answer that last point with confidence, that alone is a reason to run the break-even framework before making any decision in either direction.
The operational factors that tip the RCM outsourcing decision
The break-even framework gives you the financial picture. But cost is not the only variable that determines which billing model works better for your practice. Three operational factors consistently tip the decision in one direction or the other for mid-size behavioral health practices.
- Payer mix complexity: An in-house team managing a complex payer mix needs to stay current across all of it simultaneously. That is a significant ongoing training and oversight burden. A specialized RCM vendor handles this across multiple clients and payer relationships, which means their working knowledge of payer-specific rules is typically more current and more detailed than what an in-house team of two or three billers can maintain. If your practice bills across more than six to eight payers with materially different requirements, payer complexity alone is a strong operational argument for outsourcing.
- Behavioral health compliance exposure: Similarly, behavioral health carries specific compliance exposure around documentation, medical necessity, and audit readiness that general billing staff may not be equipped to manage without dedicated training. If your current billing team is also carrying credentialing and compliance responsibilities, your effective billing capacity is lower than your headcount suggests.
- Scalability: In-house billing scales in steps. When claim volume grows beyond what your current team can handle, you hire another biller. That means another fully loaded salary, another onboarding period, and another single point of failure if that person leaves. Outsourced RCM scales continuously. Your vendor absorbs volume increases without you hiring, training, or managing additional staff. For a practice that is actively growing, adding providers, or expanding service lines, this operational flexibility has real value that does not show up directly in the break-even calculation but affects your administrative overhead significantly over time.
What to look for in an RCM partner built for behavioral health
Not every RCM vendor is equipped to handle behavioral health billing. Choosing the wrong partner does not just fail to solve your current problems. It creates new ones. Here is what to evaluate before you sign a contract.
- Behavioral health billing expertise as a non-negotiable
- When evaluating a vendor, ask these questions directly:
- What percentage of your current client base are behavioral health practices?
- What is your average first-pass denial rate specifically for behavioral health claims?
- Which behavioral health payers do you have the most experience billing, and which have been the most challenging?
- How do you stay current on payer rule changes specific to behavioral health?
A vendor with real behavioral health experience will answer these questions with specifics. One without it will answer in generalities. That distinction matters more than any sales presentation they put in front of you.
Also confirm that the vendor has experience with your specific service lines. Outpatient therapy, intensive outpatient programs, medication-assisted treatment, and community mental health billing each carry their own billing nuances. A vendor experienced in one may not be equally strong in another.
Transparency, reporting, and accountability standards
You should never be in a position where you have less visibility into your revenue cycle after outsourcing than you had before. A credible RCM partner gives you more visibility, not less.
At minimum, your vendor should provide:
- Monthly reporting on denial rate, first-pass acceptance rate, days in AR, and net collection rate
- Claim-level transparency so you can audit individual denials and resubmissions
- Clear escalation protocols for high-value claim disputes and payer audits
- A named account manager who knows your practice and is reachable when issues arise
Be cautious of vendors who offer summary-level reporting only. If you cannot see what is being denied, why, and what action was taken, you have no way to hold the vendor accountable or identify patterns that need to be addressed upstream in your clinical documentation.
Performance benchmarks should be written into the contract, not just discussed during the sales process. Specifically, your contract should define target denial rates, days in AR, and net collection rates, along with what happens if those benchmarks are not met consistently.
How blueBriX approaches RCM for mid-size behavioral health practices
blueBriX brings over 20 years of RCM experience to behavioral health practices, with documented outcomes that speak to exactly the performance gaps this framework is designed to measure. Across its client base, blueBriX delivers a 98% clean claim rate, a 30% reduction in AR, and up to 60% in billing cost savings. For behavioral health practices specifically, that translates to fewer denials, faster cash flow, and a billing function that no longer requires constant internal oversight to perform.
Dr. Janak Kumar Mehtani, Owner and CEO of Fair Oaks Psychiatric Associates, describes the impact directly: blueBriX’s work in addressing root causes, from manual processes and outdated payment methods to credentialing challenges, enabled his practice to stabilize cash flow and build a foundation for sustained growth.
For mid-size practices evaluating RCM outsourcing, blueBriX offers:
- Behavioral health billing expertise across outpatient, IOP, MAT, and community mental health service lines, backed by certified coders with specialty-specific training
- Full transparency through real-time dashboards covering denial rates, AR aging, and collection performance, so you always have visibility into how your revenue cycle is performing
- Prior authorization management and credentialing support included as part of the service scope, not priced as add-ons
- A dedicated account team with direct knowledge of your payer mix and practice workflows
- Contract terms with defined performance benchmarks and accountability built in from the start, not discussed during the sales process and absent from the agreement
The goal is to produce measurably better revenue cycle outcomes than your current model is delivering while giving you the visibility to verify that performance at any point.
A decision checklist for practice administrators ready to evaluate RCM outsourcing
You have the framework. You have the cost categories, the performance benchmarks, and the operational factors. Before you make a final call, work through these ten questions. If you cannot answer most of them with confidence, that is a signal your current billing model lacks the visibility it needs regardless of which direction you decide to go.
The ten questions to answer before you decide
- What is your fully loaded in-house billing cost per year, including all direct and indirect costs?
- What is your current first-pass denial rate over the last 12 months?
- What are your current days in AR and how has that trended over the past year?
- How many times has your billing team turned over in the last two years and what did that cost you?
- What percentage of your billing team’s time is spent on prior authorizations and credentialing versus active claims work?
- Do you know your net collection rate by payer and how it compares to behavioral health benchmarks?
- Has your claim volume grown to a point where your current team is operating at or near capacity?
- Can your current billing model scale with your practice without adding headcount?
- Have you received a fully scoped outsourcing quote that includes all services your practice actually needs?
- Have you run the break-even calculation in Section 4 with your actual numbers?
If your answers to questions 2, 3, 4, and 8 point to underperformance or unsustainable scaling, outsourcing deserves serious evaluation. If you cannot answer questions 1, 6, and 10, start by building that visibility into your current billing performance. You cannot make a sound outsourcing decision without that baseline.