How can the claim get denied when the authorization is approved?
The authorization existed, but the system that generated the claim had no live connection to the system that tracked it. That disconnect, not a documentation failure or a coverage gap, is the cause of most PRTF per-diem denials.
Your utilization review coordinator confirmed the authorization. The dates are right. The patient is in the bed. Your billing team submits the claim.
And the remittance comes back at zero.
No remark code explains it clearly. The clearinghouse didn’t catch it. And because the denial looks like a standard authorization issue — the kind that happens every week — it gets logged, set aside, and maybe appealed if someone has bandwidth. Most of the time, it doesn’t get appealed. It gets absorbed.
This is the operational reality for most psychiatric residential treatment facilities (PRTFs) billing on a Medicaid per-diem model: authorization failures that look administrative on the surface are actually structural. The authorization existed. The problem was that the system generating the claim had no live connection to the system tracking the authorization. At some point in the chain — a concurrent review extension, a revenue code entry, an expiration date — the link broke. And a legitimate claim paid zero.
blueBriX has a psychiatric residential EHR and RCM platform purpose-built for organizations like yours. This article draws on how integrated, episode-level RCM workflows close the auth-to-claim gap — for billing managers and revenue cycle leaders who want to understand exactly where that break happens, what it costs, and how to fix it permanently.
Why does PRTF per-diem billing create authorization risk that outpatient billing doesn’t?
PRTF billing is structurally different from outpatient billing because the billable unit is not a service — it is a day of residential occupancy at an authorized level of care. That single distinction creates a category of authorization tracking risk that does not exist in encounter-based billing.
In outpatient behavioral health, billing is encounter-based. One session, one note, one claim. If an authorization was required, it typically covers a service type or a session count. The link between auth and claim is simple and short.
PRTF billing — the revenue cycle management process specific to Psychiatric Residential Treatment Facilities, which are residential programs providing 24-hour therapeutically staffed treatment for children and adolescents under age 21 — is a different category of complexity entirely. Because PRTFs bill per day of occupancy rather than per service encounter, every occupied day must be individually matched to an active, valid authorization.
A single authorization covers a block of days, usually between 7 and 30 depending on the payer and level of care. Each day in that block has to be individually matched to the authorization on file.
Concurrent review — a utilization management process in which a payer’s clinical reviewer assesses whether continued residential treatment is medically necessary while the patient is still admitted, functioning as a rolling prior authorization renewal — is required by most Medicaid MCOs every 7 to 14 days for active residential stays. Each completed concurrent review generates a new or extended authorization that carries a different authorization number than the original admission auth. A 45-day stay may involve three to five distinct authorization records before the patient discharges.
The level of care approved in the authorization maps to specific revenue codes on the claim. Revenue codes — the four-digit codes on a UB-04 claim form that identify the type of service provided — are payer-specific in PRTF billing and must match exactly to what the payer has recorded on their end. Not approximately. Not by clinical equivalence. Exactly.
Discharge and re-admission events, therapeutic passes, and leaves of absence each create additional tracking requirements that affect which days are billable and at what level.
The scale of the authorization burden in behavioral health
Behavioral health services face approximately three times the prior authorization volume of medical and surgical services on a per-encounter basis, according to the American Medical Association’s 2024 Prior Authorization Physician Survey. For a facility with 30 to 40 active patients, each generating multiple auth records over multi-week stays, the volume of authorization data that has to stay synchronized with claims generation is substantial. Managing that synchronization manually is where the failures start.
What are the three authorization-to-claim failure modes costing PRTF’s revenue?
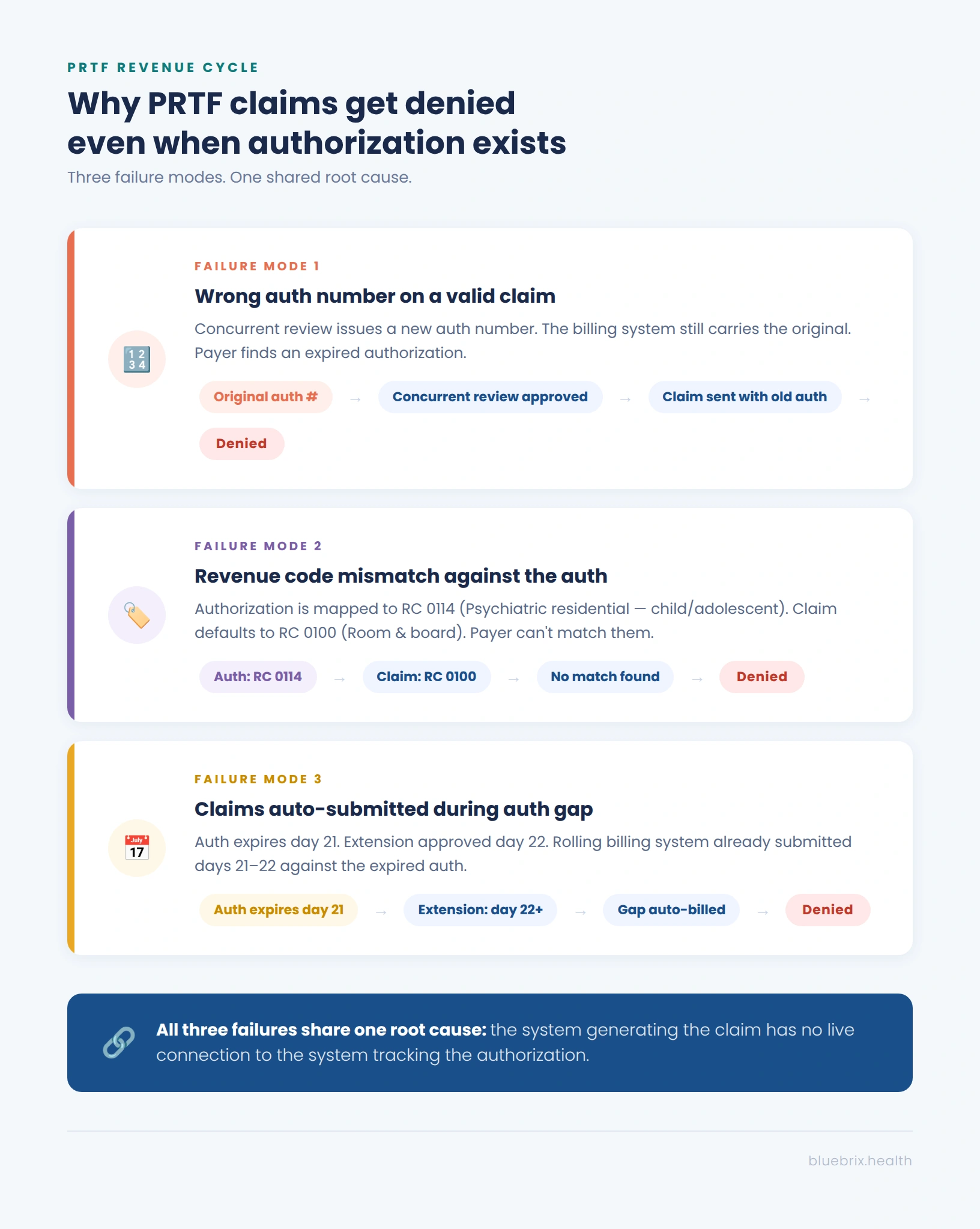
The three most common causes of PRTF authorization-related claim denials are: submitting claims against a superseded authorization number after a concurrent review extension, a revenue code mismatch between the claim and the authorization on file, and claims auto-generated during the gap between an expired authorization and a new extension.
Understanding why denials happen is more useful than counting them. These are the three most common failure modes in PRTF auth-to-claim workflows.
Failure mode 1: the wrong authorization number on a valid claim
A patient is admitted under an initial authorization covering Days 1 through 14. On Day 12, a concurrent review is completed and coverage is extended through Day 30 — under a new authorization number. The billing team submits claims for Days 15 through 30 carrying the original auth number, because the billing system was never updated when the extension came through. The payer’s adjudication system looks up the auth number on the claim. It finds an authorization that expired on Day 14.
Failure mode 2: revenue code mismatch against the authorization on file
A commercial plan authorizes a 14-year-old patient for Revenue Code 0114, which corresponds to Psychiatric Residential Treatment for children and adolescents. The billing team’s charge master defaults to Revenue Code 0100, Room and Board — Routine. The claim is submitted with RC 0100. The payer’s system has RC 0114 mapped to the authorization. The revenue codes don’t match.
Failure mode 3: claims submitted against expired authorizations during concurrent review gaps
A patient’s authorization covers through Day 21. Concurrent review was submitted on Day 18. The payer responded on Day 22, one day after the current auth expired, approving an extension effective Day 22. Days 21 and 22 now fall in a gap: the original auth expired and the extension doesn’t cover them retroactively. The billing system, set to auto-generate per-diem claims on a rolling schedule, already submitted claims for those days carrying the expired auth number.
What is the real financial cost of auth-to-claim disconnect at a PRTF?
Authorization-to-claim disconnect is one of the most financially significant and least visible failure modes in PRTF revenue cycle management. Because the denials blend into broader authorization categories on the 835 remittance, the true cost is routinely underestimated by billing teams.
The financial exposure from authorization-to-claim failures is difficult to quantify precisely because it hides inside broader denial categories on the 835. But the aggregate picture from credible sources is significant.
A 2023 federal report found that Medicaid MCOs denied more than 2 million prior authorization requests in 2019, for an overall prior authorization denial rate of nearly 13%, according to KFF analysis of federal data. Behavioral health services are disproportionately represented in those figures. The 2024 Mental Health and Substance Use Disorder Parity Report published by HHS found that insurers applied more restrictive prior authorization requirements to behavioral health benefits than to medical and surgical benefits in the majority of plans reviewed.

For a PRTF operating 40 beds at 85% average occupancy and billing a $600 per-diem Medicaid rate, annual claims total approximately $7.4 million. Authorization-related failures that contribute to even 10% of initial denials represent $740,000 entering a rework queue annually.
Not all of that is permanently lost — but a meaningful portion is, because denial appeals in behavioral health are filed at very low rates. KFF’s 2024 analysis of marketplace claims found that fewer than 1% of denied claims were appealed, with insurers upholding their original decision 66% of the time when appeals were filed. For PRTF billing teams managing high census with limited staff, the decision to absorb a denial rather than appeal it is often rational in the moment and expensive in aggregate.
What does CMS-0057-F change for PRTF billing and what it doesn’t cover?
CMS-0057-F improves payer-side authorization transparency and decision timelines. It does not address how a PRTF facility tracks, routes, or links authorization data to its claims generation workflow. That gap remains the provider’s responsibility.
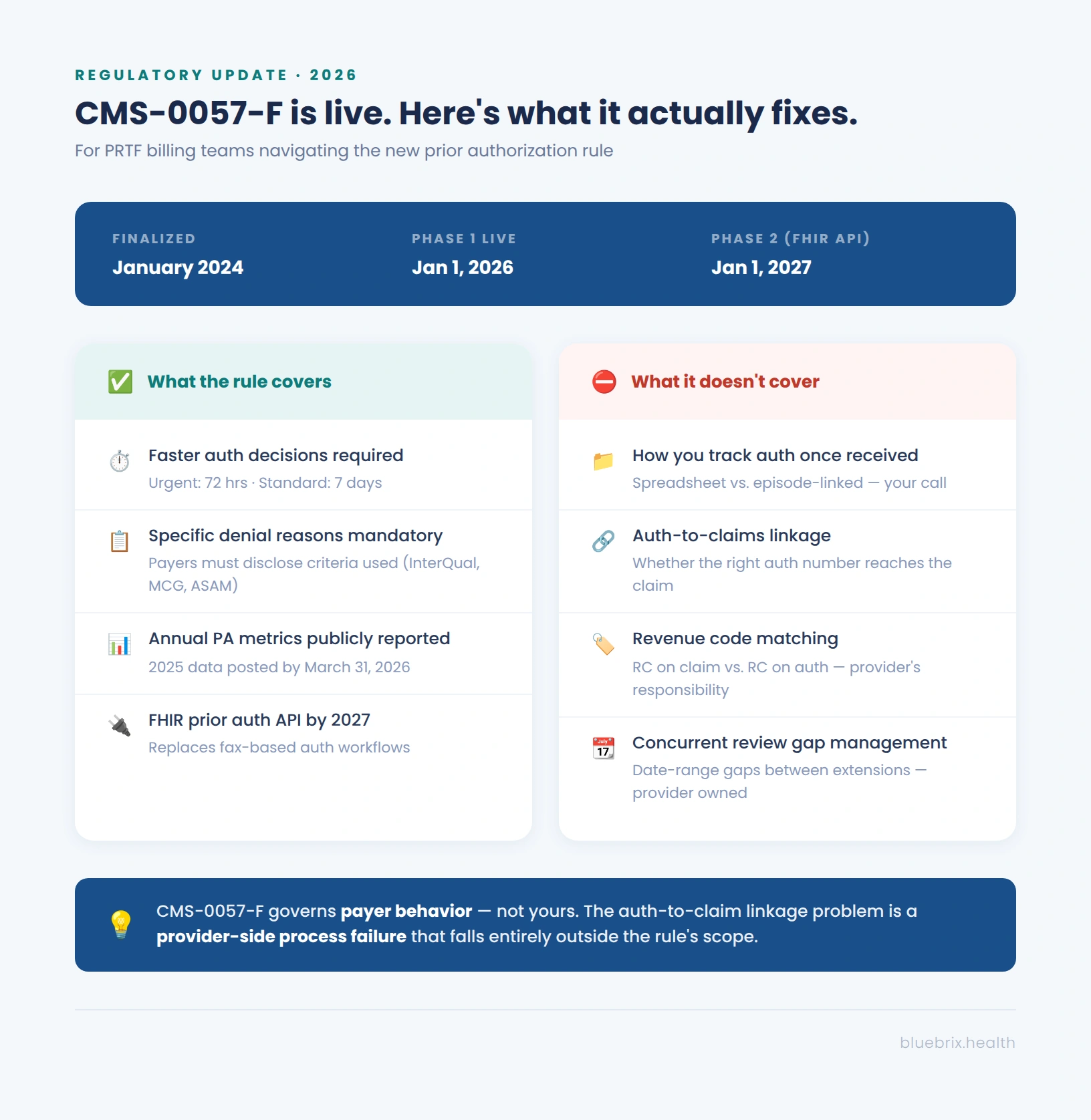
PRTF billing managers and compliance leaders should understand both the opportunity and the limitation of the CMS Interoperability and Prior Authorization final rule — CMS-0057-F, the federal rule finalized in January 2024 that governs how covered payers must handle prior authorization decisions.
Under Phase 1, covered payers including Medicare Advantage organizations, Medicaid managed care organizations, CHIP managed care entities, and qualified health plan issuers on federal exchanges, are required to provide a specific reason for every denied prior authorization decision, meet defined decision timelines, and publicly report prior authorization metrics annually. Impacted payers were required to collect 2025 metrics and post them publicly by March 31, 2026.
Phase 2, effective January 1, 2027, requires those same payers to implement a FHIR-based Prior Authorization API using the HL7 Da Vinci PAS implementation guide enabling electronic, real-time prior authorization submission and response.
This enables PRTF billing teams with faster decisions, required specificity on denial reasons, and eventually electronic auth submission that eliminates fax-based workflows. The requirement for payers to disclose the clinical criteria set they used to deny, whether InterQual, MCG, ASAM criteria, or a proprietary standard, gives facilities significantly better grounds for appeals.
What CMS-0057-F does not cover
The rule governs payer behavior — not yours. It does not govern how your facility tracks the authorization once received, how it flows from the UR team into the claims generation workflow, or whether the revenue code on the claim matches the auth on file. The auth-to-claim linkage problem is a provider-side process failure, and it falls entirely outside the scope of CMS-0057-F. Facilities that rely on the rule to reduce their denial rate without addressing internal workflow gaps will be disappointed.
For facilities whose denial problem is rooted in payer behavior such as overly restrictive criteria, unreasonable concurrent review timelines etc., CMS-0057-F is meaningful relief. For facilities whose denial problem is rooted in internal workflow gaps, the rule changes the payer environment but leaves the core problem intact.
How does integrated RCM automation fix the auth-to-claim disconnect?
Integrated RCM automation fixes the auth-to-claim disconnect by bringing the authorization record and the claims engine onto the same data model, anchored to the patient’s active episode of care, so that every claim is validated against a live authorization before it submits, not after it’s denied.
The reason auth-to-claim disconnect persists despite manual oversight is that it’s an architecture problem, not an attention problem. The UR coordinator manages authorizations in one system or spreadsheet. The clinical team documents in another. The billing team generates claims from a third data source. At every handoff between those systems, data can lag, be miskeyed, or simply fail to transfer.
No volume of manual reconciliation fully closes a structural gap because the gap regenerates with every new authorization, every concurrent review, and every rolling claims batch.
The architectural fix is to bring the authorization record and the claims engine onto the same data model, anchored to the patient’s active episode of care.
Authorization lives on the episode, not in a document
When authorization data lives on the episode, the auth number, approved dates, authorized level of care, revenue code mapping, and payer-specific requirements are all available to the claims engine at the moment of claim generation. The claims engine doesn’t pull from a spreadsheet someone updated this morning. It pulls from the same record the UR coordinator updated yesterday.
Concurrent review extensions update the episode automatically
When a concurrent review extension is issued, the new auth number is reflected in the next claims batch without a manual update, a notification from UR to billing, or a handoff that can fail.
Revenue code validation runs before the claim submits
When a per-diem claim is generated, the platform validates the revenue code against the authorization on file before the claim leaves the system. If there’s a mismatch, the claim is held and surfaced to the billing manager — not sent out to generate a denial that takes weeks to resolve.
Auth expiration alerts fire before the claims batch runs
When an authorization is approaching its expiration date with no concurrent review extension on file, the system alerts the UR team ahead of the deadline and holds at-risk claims from the submission batch until the issue is resolved.
This is the difference between managing denials and preventing them. The billing manager’s role shifts from investigating last week’s remittance to reviewing a pre-submission exception queue where problems are named, specific, and fixable before they cost anything.
Why should PRTFs consider blueBriX for revenue cycle management?
blueBriX’s psychiatric residential EHR is purpose-built to manage clinical, operational and revenue cycle management so that your teams have a proactive, real-time edge and get to focus fully on your patients.
For PRTF billing specifically, blueBriX brings authorization tracking, concurrent review management, and claims generation onto a single, integrated episode-level workflow. Authorization records attach to the patient’s active episode of care at admission. Concurrent review extensions update the episode record directly. Revenue code validation happens at the pre-submission stage, not after denial. Auth expiration alerts fire before the claims batch runs.
The result is a billing workflow that enforces auth-to-claim linkage systematically. Claims go out with the right authorization number, the right revenue codes, and the right date ranges — not because a billing specialist checked each one manually before the batch ran, but because the platform makes the correct claim the path of least resistance.

For compliance leaders, the same integrated record that prevents billing errors also creates the audit-ready documentation trail that Medicaid auditors require: a linked record showing the authorization on file, the level of care authorized, and the days billed, available on demand without manual reconstruction from multiple systems.
blueBriX also supports multi-payer environments, payer-specific billing rule configuration, and pre-built compliance reporting for Medicaid — meaning the platform handles the operational complexity that PRTF billing teams face daily without requiring custom development or workaround processes.
Book a PRTF billing demo with blueBriX
The auth-to-claim disconnect is not a staffing problem, a training problem, or a process discipline problem. It is a systems architecture problem — and the solution is an integrated platform where the authorization record and the claims engine operate from the same source of truth.
See exactly how blueBriX closes the gap for PRTFs — authorization tracking, concurrent review management, revenue code validation, pre-submission scrubbing, and Medicaid-ready compliance reporting — in a live demo tailored to your payer mix, census size, and current workflow.