
For the better part of a decade, digital health has lived in a comfortable shade of gray. We had mandates, sure. But we also had excuses, valid ones! If a patient app wanted data in a specific format, and your 15-year-old EHR couldn’t spit it out, you could raise your hand and say, technically infeasible. And for the most part, the regulators nodded and backed off. It was a safety net woven out of our own technical debt.
The HTI-5 proposed rule just took a pair of shears to that net. When we say shears, we refer to the HTI-5 proposed rule (Health Data, Technology, and Interoperability: ASTP/ONC Deregulatory Actions to Unleash Prosperity) explicitly removing the Information Blocking exceptions that acted as loopholes.
Specifically, the rule proposes:
- Eliminating the TEFCA-specific manner exception: You can no longer delay data sharing by insisting on using a specific Trusted Exchange Framework if a direct connection is possible.
- Narrowing the infeasibility exception: It drastically reduces the valid reasons a provider can claim technical difficulty to deny a data request, forcing a shift to FHIR-first exchange regardless of legacy system limitations.
Essentially, the net was the legal ability to say “no” based on tech limits; HTI-5 removes that option.
While much of the industry is celebrating the deregulation aspect, the removal of functional certification criteria, they are missing the sting in the tail. The Office of the National Coordinator (ONC) isn’t just cutting red tape; they are cutting the slack. By proposing the removal of key Information Blocking exceptions, specifically the TEFCA-specific Manner Exception, the message is brutal in its simplicity: The limitations of your software are no longer a valid excuse for blocking patient data.
The HTI-5 approach
Let’s talk about what this actually looks like on the ground. Previously, if a third-party app requested data, you could often negotiate the terms of that exchange based on what your system could easily handle. It was a meet me where I am approach.
HTI-5 flips this. It is now a meet the standard where it is approach. The proposed changes require that if you have the data, you must share it. The friction caused by proprietary formats, closed APIs, or we’ll get to it in the next roadmap update defenses is evaporating.
This creates a terrifying reality for decision-makers at mid-sized health systems and specialized clinics. You are likely sitting on a tech stack that was finalized five years ago. You cannot simply turn on FHIR (Fast Healthcare Interoperability Resources) capabilities if your underlying architecture speaks HL7 v2 or proprietary SQL.
The compliance trap: When your EHR becomes your liability
Here is the scenario keeping CIOs up at night: A patient connects a new health management app to your portal. The app pings your system for longitudinal records. Your system blocks the request or offers a PDF because it cannot parse the discrete data request.
Under the old rules, you had cover. Under HTI-5, this is Information Blocking.
The regulators are betting that by removing these exceptions, they will force the market to modernize. They are right. But they are also putting providers in a vice. You have two bad options:
- Rip and replace: Spend millions and years migrating to a monolithic EHR that promises compliance but kills your specialized workflows.
- Wait and pay: Absorb the penalties and reputational damage while you patch holes in a sinking ship.
But there is a third option. One that the big monolithic vendors don’t want you to focus on because it doesn’t involve signing a ten-year contract.
The FHIR wrapper strategy
The smartest players in the US healthcare segment aren’t replacing their legacy systems; they are wrapping them. They are acknowledging that while their core database might be dumb when it comes to FHIR, their interface doesn’t have to be.
This is where blueBriX enters the narrative. We don’t ask you to change your source of truth. We ask you to let us translate it.
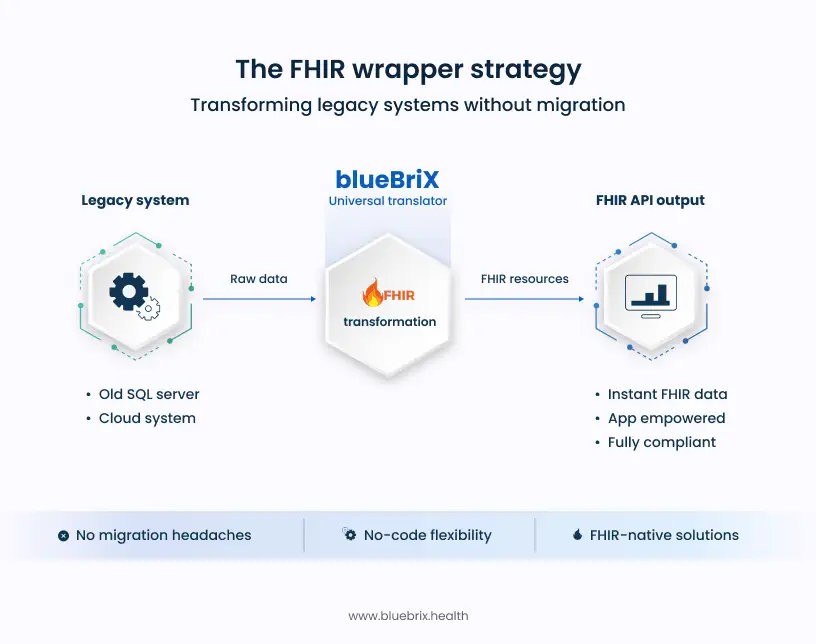
Think of blueBriX not as another piece of software, but as the universal translator for your ecosystem. Our low-code/no-code platform sits on top of your existing infrastructure, whether it’s a dusty on-premise SQL server or a fragmented cloud setup, and acts as the FHIR-native lung that breathes life into it.
When that patient app requests data, it hits the blueBriX layer. We pull the raw data from your legacy backend, structure it instantly into FHIR resources, and hand it over. The app is happy. The patient is empowered. And you? You are compliant. No migration nightmares. No technical infeasibility excuses needed.
Ready to turn your compliance gap into a competitive edge?
Schedule a 15-Minute HTI-5 Readiness Assessment with a blueBriX Architect
Schedule a demo