The OHFLAC compliance scramble
It is a phrase that makes every Executive Director in West Virginia freeze: “The surveyors are in the lobby.”
It doesn’t matter if you run a gold-standard operation. It doesn’t matter if your clinical outcomes are the best in the Appalachians. In that moment, your entire reputation hinges on your ability to pull specific, fragmented pieces of data out of your system.
- “Show me the staff training logs for the Chapter 513 unit for the last six months.”
- “Pull the incident report from the residential fall last Tuesday—and the follow-up investigation.”
- “Prove that your new hires were screened against the Cares registry before they touched a patient.”
What makes this moment dangerous isn’t missing data, its data trapped in the wrong format. Generic EHRs can store information, but they cannot reshape it on demand into program-specific, audit-ready reports. Compliance fails at extraction, validation, and presentation, exactly where most systems go rigid.
In a perfect world, you would click a button and hand them a tablet. But in the real world, the world of fragmented, legacy healthcare software, you are likely sprinting to a filing cabinet, texting a manager to check a spreadsheet, or frantically logging into three different portals.
This is a failure of technology.
The generic Behavioral Health EHR you bought was built for a hypothetical clinic in California or Florida. It wasn’t built for the specific, overlapping, and often contradictory demands of West Virginia Code 64-11 or the nuances of OHFLAC oversight. More than better features, you need a system that understands West Virginia.
Multi-program illusion: one roof, three rulebooks
The biggest trap for growing providers in the Mountain State is the Multi-Program Illusion. You might see your organization as one unified entity, but the state sees distinct regulatory islands.
If you are expanding from Substance Use Disorder (SUD) treatment into Intellectual and Developmental Disabilities (IDD) waivers, you aren’t just adding a new service line. You are stepping into a different legal universe.
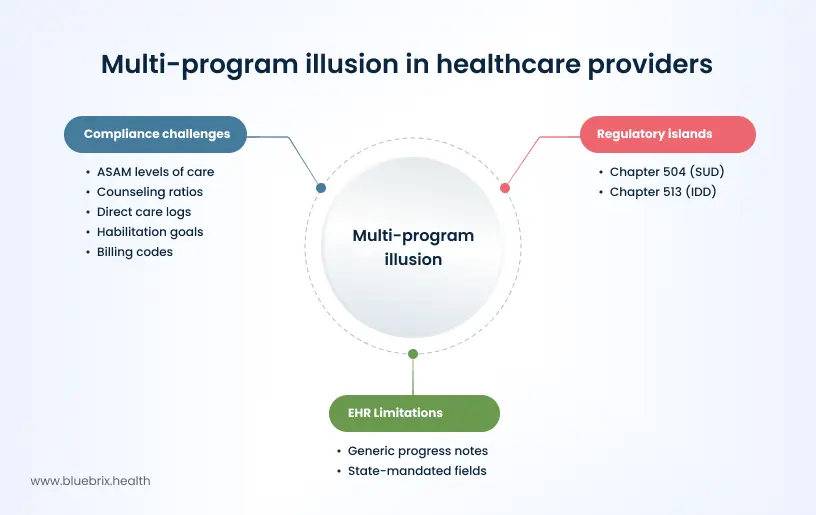
- Chapter 504 (SUD): Demands rigorous tracking of ASAM levels of care and specific counseling ratios.
- Chapter 513 (IDD): Shifts the focus entirely to direct care logs, distinct habilitation goals, and a completely different set of billing codes.
The conflict: Most off-the-shelf EHRs try to force these round pegs into square holes. They offer a generic progress note that doesn’t capture the specific state-mandated fields required for a Chapter 513 audit.
The result? Your staff adopts the spreadsheet band-aid. They document what they can in the EHR to get the bill out, but they track the real compliance data that keeps your license safe, in Excel.
This shadow data is invisible to you until an auditor asks for it. And by then, it is often too late.
The OHFLAC factor: safety vs. spreadsheets
The Office of Health Facility Licensure and Certification (OHFLAC) is not interested in your billing efficiency. They are interested in patient safety and strict adherence to state legislative rules.
Consider the Incident report.
In a standard EHR, an incident report is a static form. You fill it out, save it, and it sits in the database. But in West Virginia, the timeline for reporting specific allegations (abuse, neglect, misappropriation) is aggressively short, often immediate or within 24 hours.
If your system doesn’t actively push that data to your Compliance Officer the second it is saved, you are exposed.
The legacy failure: A staff member logs a critical incident on Friday afternoon. The system files it. Nobody sees it until Monday morning. You have now missed the mandatory reporting window. You are non-compliant.
The need: You need a system that triggers workflows, not just storage. You need a system where Incident Type = Abuse automatically triggers an SMS to the Director and generates the specific PDF format required by the state.
Why ‘wait for update’ is a broken strategy
Managing healthcare compliance in West Virginia successfully means building efficient systems for tracking state-specific regulations. Yet, most providers are held hostage by their vendor’s roadmap.
When the Bureau for Medical Services (BMS) updates a fee schedule, or when OHFLAC revises a licensure standard, you typically have two options:
- Wait 6-12 months for your vendor to hard-code the change (if they ever do).
- Create a paper workaround (another form to scan).
The real bottleneck is reporting agility, more than form creation. When policy changes, providers don’t just need new fields. They need new reports, new dashboards, new audit extracts, often immediately.
Waiting for vendor updates means waiting for someone else to decide which metrics matter, how they’re grouped, and when they’re available. In compliance-heavy environments like West Virginia, that delay is a direct operational risk.
blueBriX report builder: compliance you can prove, on demand
blueBriX flips this model on its head. We don’t try to build a perfect static form for West Virginia, because we know the form will change next year.
Instead, we built a flexible reporting engine that puts the power back in your hands.
1. The no-code form builder
New OHFLAC requirement dropped this morning? With blueBriX, you don’t call us. You (or your admin) can drag-and-drop the new required fields into your intake or incident forms in minutes.
When a provider needs to start tracking housing instability for a new waiver pilot, in blueBriX, they add the field, link it to the client profile, and start reporting on it that afternoon.
2. State-specific logic layers
You can configure blueBriX to enforce West Virginia’s specific rules at the point of entry.
You can set a rule that prevents a “Chapter 504” progress note from being signed unless the “ASAM Level” field is populated. This stops the error before it becomes a billing denial or an audit finding.
3. No-code report builder with compliance-ready outputs
Compliance doesn’t end when data is captured—it begins when that data must be proven, compared, and submitted.
blueBriX’s no-code report builder allows administrators to create configurable report templates aligned to OHFLAC, BMS, OMH, and program-specific requirements—without writing SQL or waiting for vendor customization.
With blueBriX, your teams can:
- Build customizable data extracts for audits and compliance reviews
- Generate role-specific views for compliance officers, program heads, and executives
- Schedule automatic report distribution to internal teams or regulators
- Export reports in CSV, Excel, or XML, aligned with state submission formats
When surveyors ask for proof, you don’t scramble. You select the template and export.
4. Pre-configured outcome dashboards & longitudinal views
blueBriX goes beyond static reports with pre-configured outcome dashboards built for behavioral health and multi-program oversight.
Compliance leaders can track:
- Longitudinal patient views across programs and episodes of care
- Improvement trending and analytics to identify documentation drift before it becomes a citation
- Program-level performance comparisons across locations or licenses
- Peer benchmarking using standardized, customizable metrics
Instead of asking “Are we compliant?”, teams can see where risk is accumulating, weeks before an audit.

Solution in action: Automating mountain health trust reporting
- The scenario: Many multi-site providers in the Kanawha Valley struggle to transition to new managed care reporting requirements. Legacy systems often cannot export specific Utilization Review data without expensive custom coding.
- The blueBriX approach: Users can utilize the Custom Report View to pull the exact clinical and demographic fields required by West Virginia payers. They can utilize configurable report templates and customizable data extracts to pull exact clinical, demographic, and program-level fields filtered by Chapter, location, date range, or payer, without writing a single line of code.
- The projected impact: This workflow is designed to reduce monthly reporting labor from 40 hours of manual collation to roughly 15 minutes of automated export, eliminating the copy-paste errors that frequently lead to claim rejections.
- Audit readiness: Program-specific reports remain standardized, version-controlled, and reproducible across survey cycles.
Don't wait for the next audit to find the gaps in your reporting
See exactly how blueBriX simplifies OHFLAC and Chapter-specific compliance in a live walkthrough.
Contact us